
Abstract
Objectives
To evaluate the cost-benefit of implementing an expanded newborn screening programme for hyperphenylalaninemias due to 6-pyruvoyl-tetrahydropterin synthase (PTPS) deficiency in Hong Kong.
Setting
Regional public hospitals in Hong Kong providing care for cases of inborn errors of metabolism.
Methods
Implementational and operational costs of a new expanded mass spectrometry-based newborn screening programme were estimated. Data on various medical expenditures for the mild and severe phenotypic subtypes were gathered from a case cohort diagnosed with PTPS deficiency from 2001 to 2009. Local incidence from a previously published study was used.
Results
Implementation and operational costs of an expanded newborn screening programme in Hong Kong were estimated at HKD 10,473,848 (USD 1,342,801) annually. Assuming a birthrate of 50,000 per year and an incidence of 1 in 29,542 live births, the medical costs and adjusted loss of workforce per year would be HKD 20,773,207 (USD 2,663,232). Overall the annual savings from implementing the programme would be HKD 9,632,750 (USD 1,234,968).
Conclusions
Our estimates show that implementation of an expanded newborn screening programme in Hong Kong is cost-effective, with a significant annual saving for public expenditure.
Keywords
Introduction
Since its introduction in the early 1960 s, newborn screening (NBS) has become one of the most effective public health measures in preventing childhood disability and mortality.1,2 Tandem mass spectrometry (MS/MS), electrospray ionization MS/MS, and recent advances in molecular genetics have expanded the scope of screening to include more conditions.3–6 The American College of Medical Genetics now includes 29 conditions in the core panel of expanded newborn screening, with 25 additional conditions as secondary targets. 7 Many areas, including Mainland China, India, Japan, Malaysia, Pakistan, Philippines, Singapore, South Korea, Taiwan, and Thailand provide some degree of expanded NBS.
In contrast, the Hong Kong NBS programme screens for only two metabolic conditions (congenital hypothyroidism and glucose-6-phosphate dehydrogenase [G6PD] deficiency), with well-established local infrastructure.8,9 The local incidence of classical inborn errors of metabolism (IEM) is 1 in 4,122 live births 10 (69% amino acidemias, 12% organic acidemias, and 19% fatty acid oxidation defects). Conditions with the highest incidences in the three individual groups are hyperphenylalaninemia and citrin deficiency, holocarboxylase synthetase deficiency, and carnitine-acylcarnitine translocase deficiency respectively. The incidence is comparable with worldwide incidences, particularly among those of Chinese descent.11–13 In early 1970s, there was no PKU identified with the screening of 18,000 newborns in Hong Kong. 14
Without expanded NBS, local patients with IEM are likely to eventually present at the symptomatic stage, by which time severe and irreversible damage may have already developed. Following the death of a previously healthy 14-year-old boy from multiple acyl-CoA dehydrogenase deficiency (glutaric aciduria type II) in 2008 15 , a postmortem report urged the conduct of a feasibility study on expanded NBS (http://www.judiciary.gov.hk/en/publications/coroner_report_july08.pdf), but IEM patients continued to present late and severe.16–19 In 2013 the first pilot study on expanded NBS in public hospitals demonstrated a feasible service model (“namely the OPathPaed model”) for expanded NBS in Hong Kong. 20
We therefore carried out a cost-benefit analysis on screening for 6-pyruvoyl-tetrahydropterin synthase (PTPS) deficiency, one of the more frequently occurring disorders likely to be detected by MS/MS. The incidence of hyperphenylalaninemias in Hong Kong is 1 in 29,542; all Hong Kong Chinese patients with hyperphenylalaninemias were genetically confirmed to have PTPS deficiency. 10 Hyperphenylalaninemias encompass several enzyme defects in the phenylalanine metabolism, including classical phenylketonuria (PKU) with phenylalanine hydroxylase deficiency, and atypical PKU affecting the tetrahydrobiopterin synthetic pathway where PTPS deficiency belongs to and is the only defect reported among Hong Kong Chinese so far. In addition to the typical PKU phenotype, patients with PTPS deficiency suffer from neurological deficiency of neurotransmitters. Treatment requires high protein restriction and replacement of tetrahydrobiopterin, L-dopa and 5-hydroxytryptophan. Patient intelligence quotient is significantly inversely correlated with the timing of treatment 21 , although normalization of intelligence quotient has been reported in patients identified by NBS who receive early treatment. 22
We believe this is the first cost-benefit analysis conducted for an NBS programme for hyperphenylalaninemia due to PTPS deficiency.
Methods
The comparative costs of screening versus not screening should take into account, among other factors, hospitalization and treatment, social consideration, laboratory investment in screening, and follow-up service. Conventionally, comprehensive epidemiological data showing frequencies of health outcomes in screened and unscreened cohorts and cost economic data are required. Population-based data rather than a clinical case series should be used in epidemiological analysis, as a clinical case series may over-represent those who are most severely affected. For example, among all children born with hyperphenylalaninemia in Hong Kong, the number of patients who suffer from mental retardation and the number of patients with normal development (if any) must be known for a cost-effectiveness analysis. The outcomes of treated unscreened children versus those of treated screened children should then be compared, to assess the impact of expanded NBS. The total cost of treatment, both for the disorder and for the complications of poorly treated disease must then be calculated, to demonstrate any difference between the total costs for a cohort with and without screening.
To complete the cost-effectiveness analysis, a measure of health outcomes is needed. For non-fatal diseases, the standard measure is the quality-adjusted life-year (QALY). The calculation requires estimates of preference-based QALY weights for each outcome, multiplied by the frequencies of each health state in the two cohorts. For expanded NBS with one-test-multiple-disease, the same process is required for each IEM, as each condition is different in terms of types of outcomes and costs. Because of the rarity of IEM and the lack of population data, proper cost-effective analyses are rarely performed.
A simplified model is commonly applied to calculate the average screening cost per case detected and compare this with the cost of treatment in non-screened patients. Cost-effectiveness of PKU23–25, congenital hypothyroidism26–28, medium-chain acyl-CoA dehydrogenase deficiency29–31 and MS/MS screening30,32–35 are well documented. To inform that analysis, we first analyzed the cost of care for six unscreened symptomatic patients with hyperphenylalaninemia, and for two asymptomatic screened patients who received NBS because of their positive family history.
Costs of Operations for a Local NBS Programme for IEM
The NBS programme in Hong Kong screens for congenital hypothyroidism and G6PD deficiency. Umbilical cord blood samples are collected from maternity hospitals where all babies are delivered. The screening coverage is over 99%.
36
A new system is required for implementing expanded NBS (Figure 1). The costs of a local expanded NBS programme include costs of its establishment and operational costs. The capital investment involves addition of two MS/MS instruments in the existing infrastructure. Assuming a 50,000 birth rate and 250 working days a year, 200 dried blood spot would be processed each day. The sample preparation time requires about 3 hours using underivatized assay including succinylacetone in batch analysis. Analytical time required for one sample is 2 minutes; at least 6.6 hours of analytical time are required to run 200 DBS samples. Including the instrument optimization time and quality control measurements, eight hours are required per day. Although most NBS laboratories will perform overnight analysis, the MS/MS also needs to perform repeat testing on questionable samples or positive cases in daytime. In the local setting, operating mainly in daytime, with an expected turnaround time requirement within 24 to 48 hours, and the need for instrument back-up, two MS/MS is optimal. We depreciated the cost over eight years
33
, in which time we assume that each would be replaced by another instrument.
Cost-to-screen for expanded NBS on top of the existing cord blood programme.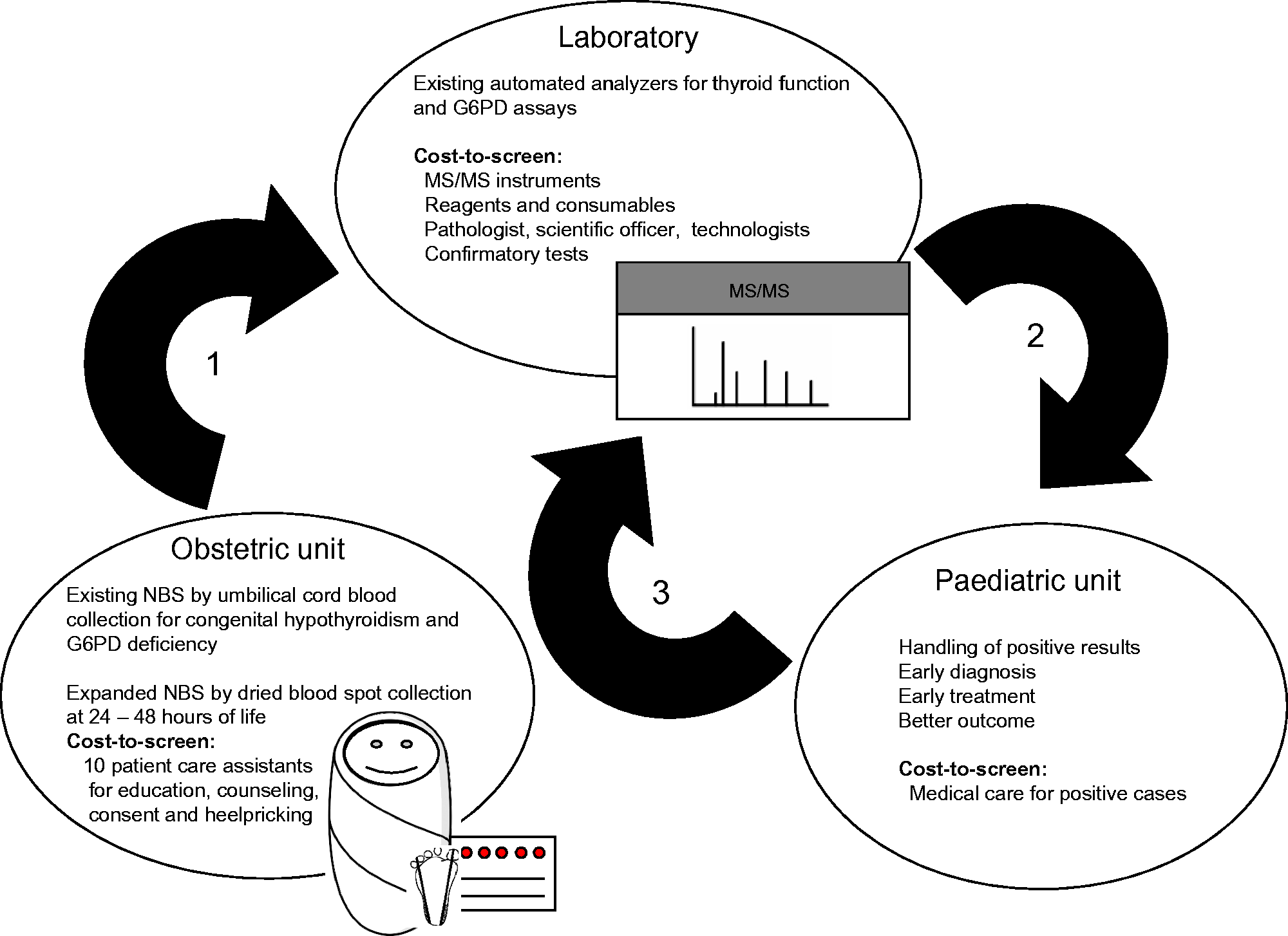
The operational costs include personnel and test consumables, as well as the costs of patient recall to follow up abnormal results. The majority of the deliveries in Hong Kong occur at the eight public maternity hospitals. Ten patient care assistants are required to perform education, counseling, obtaining consent, conducting heel prick tests, and to assist with the clerical work. One pathologist, one scientific officer, and two technologists are required to run the expanded NBS laboratory work, including sample accessioning, analysis, and reporting. In our previously published OPathPaed model 20 , the pathologist with expertise in biochemical genetics also conducted counseling of parents of babies with suspected IEM, rechecked the babies’ blood for further diagnostic investigations, referred babies to paediatric specialist care for treatment and monitoring, and conducted case tracking and regular clinical liaison. This system will reduce the false positive rate. As this is a new programme, the pathologist can also provide training and education for technical and clinical colleagues, and promote public health education to the public. The cost of training is therefore included in the personnel cost in our calculation. The wages of personnel were estimated from public hospital pay scales, and a notional annual mid-point salary is used. The costs of the equipment and consumables and confirmatory tests were retrieved from the financial records of a public hospital laboratory. The average cost per attendance/visit by specialty/service for a specialist out-patient clinic overall as a group was also based on local public hospital specialty cost information. All the costs are referenced to the 2012 year standard.
Benefits of Screening
For both cases diagnosed at presentation and by NBS, the medical costs were estimated as including attendance at emergency departments and specialist out-patient clinics, in-hospital care by number of days, computer tomography and magnetic resonance imaging during the diagnostic process and/or post-diagnosis monitoring, as well as the allied healthcare costs. The estimated savings from the loss of workforce and long-term residential care was also taken into account. The patient-specific episode numbers and/or lengths of attendance at various clinics/services for individual patients were retrieved from patient records; the average costs of services (per episode for out-patient services and attendances at emergency department, per day for hospitalization) were retrieved from 2012 specialty costs. The cost of long-term residential care was taken, from the same document, as average cost of extended care (rehabilitation). Costs of imaging were estimated from the reference list used by public hospitals on the prices of private computer tomography and magnetic resonance imaging. The loss of workforce was calculated based on the wage share of gross domestic product (GDP) in Hong Kong (latest from 2008, Extended Penn World Tables) and 2012 GDP. All costs are expressed in 2012 Hong Kong dollars (1 USD = 7.8 HKD).
Results
Costs of Operations for a Local NBS Programme for IEM
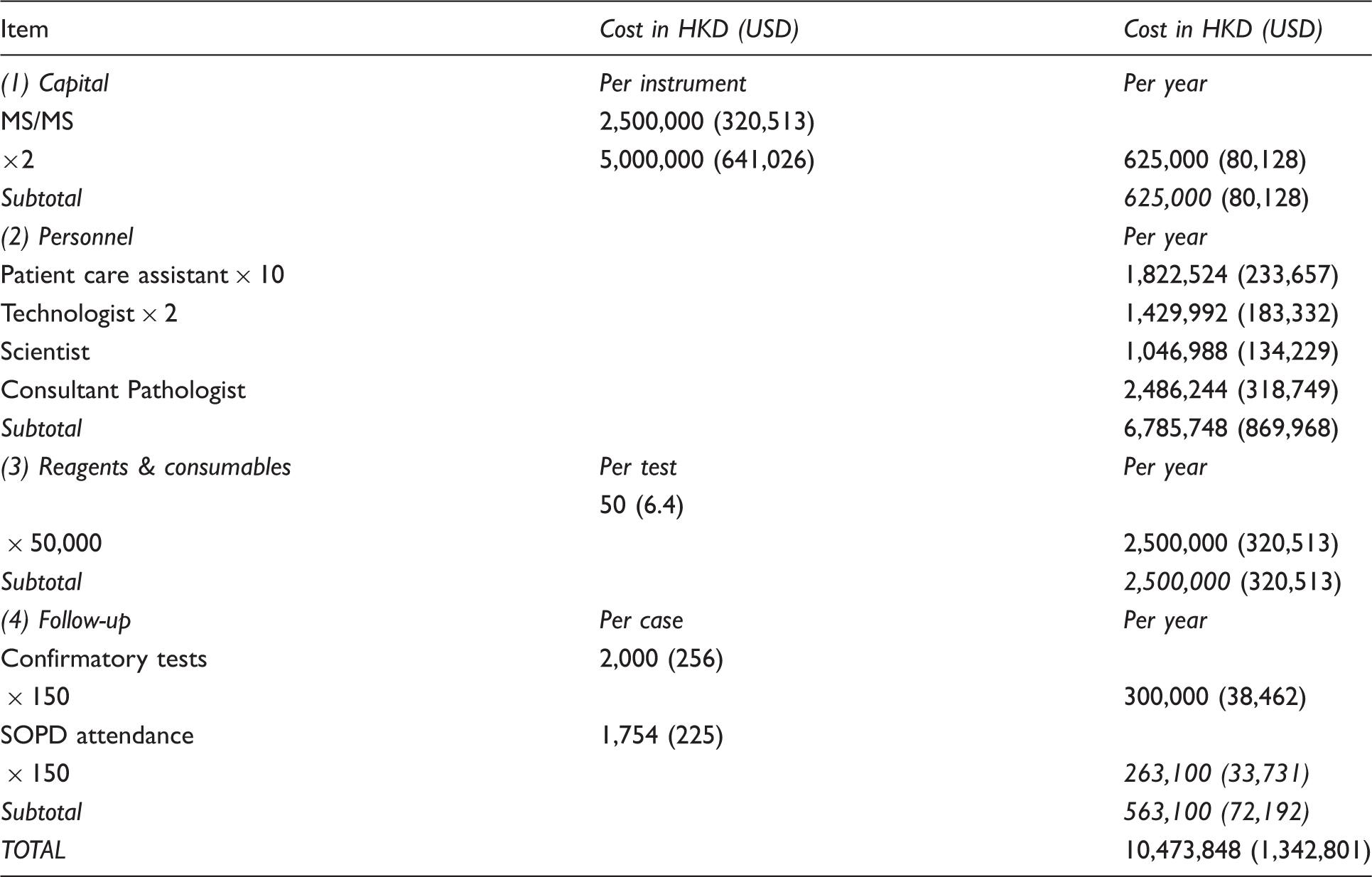
The two MS/MS instruments cost around HKD 2,500,000 (USD 320,513) each at the time of purchase (annual cost HKD 625,000 or USD 80,128). The operational costs include employing the necessary personnel: ten patient care assistants (HKD 1,822,524 per year; USD 233,657), two technologists (HKD 1,429,992; USD 183,332), one scientist (HKD 1,046,988; USD 134,229) and one consultant-grade pathologist (HKD 2,486,244; USD 318,749), ie. a total of HKD 6,785,748 (USD 869,968) per year. The consumables, including filter paper cards, reagents, and other laboratory consumables were estimated to cost HKD 2,500,000 (USD 320,513) assuming a constant annual birth rate of 50,000 and a test cost of HKD 50 (USD 6.4).
The operational costs also included follow-up and further investigations for screen-positive cases. Taking the average cost of a specialist clinic attendance (HKD 877 (USD 112)) and two visits for every screen-positive case, the costs of confirmatory testing of plasma amino acid, plasma acylcarnitine, and urine organic acid profiles (HKD 2,000 (USD 256), and a call back rate of 0.3% 37 (ie. 150 cases per year), the annual follow-up costs were estimated to be HKD 563,100 (USD 72,192).
Implementation and operational cost of expanded NBS programme in Hong Kong.
Benefits of Screening
Cases diagnosed at presentation
Six cases diagnosed with PTPS deficiency from 2001 to 2009 were included in the study. One patient (Case 4) left the Hong Kong medical system in 2007 and the clinical data were therefore only evaluated up to that time and adjusted accordingly. Two other patients (Cases 5 and 6) were only diagnosed in their adolescence and complete medical records prior to 2002 around the time of presentation were not available for evaluation. For these two patients, the annual medical care costs were HKD 8,266 (USD 1,060) and 21,334 (USD 2,735) at the age of 23 and 27 years, respectively. The average annual medical care cost of HKD 14,800 (USD 1,897) was used for calculation because their conditions, and thus medical utilization, were considered static.
Of the four cases evaluated from birth, three suffered from mild or moderate neurological insult, while the other was severely affected and dependent on long-term residential care. The present value of the future loss of workforce productivity for each was estimated to be HKD 4,863,267, or USD 623,496 (calculated taking the per capita GDP for 2012 of HKD 285,403 or USD 36,590 [http://www.censtatd.gov.hk/hkstat/sub/sp250.jsp?tableID=030&ID=0&productType=8] and the wage share of GDP to be 42.6%). It was assumed that, on average, people join the workforce at 21 years and retire at age 60. The expectation of life in 2012 was 83 years in Hong Kong (http://www.censtatd.gov.hk/hkstat/sub/so160.jsp). Even assuming a decrease in lifespan due to complications for PTPS deficiency, the duration of long-term residential care was assumed to be 50 years 38 and the cost of care was estimated to be HKD 35,843,000 (USD 4,595,256). The assumed cost per patient day for extended care for mental retardation was HKD 1,964 (USD 252).
The cost of medical care was estimated to be HKD 2,798,525 (USD 358,785) for the patient with severe retardation at age 3; for the other three more mildly affected patients this was estimated to be HKD 328,817 (USD 42,156) to HKD 585,419 (USD 75,054) at age 8-12. Assuming a lifespan of 50 years and an annual cost of medical care of HKD 14,800 (USD 1,897), these four patients were estimated to incur a total of lifetime medical costs of HKD 3,488,203 (USD 447,206) for the severely handicapped patient, and HKD 907,496 (USD 116,346) to HKD 1,198,138 (USD 153,607) for the milder three patients (Table 2). Costs in future years need to be discounted to present values.
Cases diagnosed by expanded NBS
In the same period (2001 to 2009), in addition to the six cases, two patients with a positive family history were diagnosed soon after birth, and were used as surrogates for patients diagnosed by an established expanded NBS programme. Although these two cases still require a number of hospitalization episodes for long-term monitoring of treatment and management of metabolic decompensation, the costs of medical care were significantly lower: HKD 260,562 (USD 33,405) and HKD 264,441 (USD 33,903) at the age of 7 and 9 respectively. As the average annual medical care cost was HKD 14,800 (USD 1,897), the lifetime medical costs for these patients were roughly projected to be HKD 393,859 (USD 50,495) each, presuming they survive to age 83 with a static condition and medical utilization (Table 2).
Calculations
The estimated incidence of hyperphenylalaninemia was 1 in 29,542 live births 10 , ie. 1.69 patients per year, assuming a birth rate of 50,000. The loss of workforce and GDP due to PTPS deficiency was estimated to be HKD 4,863,267 (USD 623,496) per case, while the cost of long-term residential care for 50 years was estimated to be HKD 5,973,833 (USD 765,876). Assuming the probability for unscreened patients to develop severe intellectual disabilities is one out of six (as observed in the cohort), and the lifetime medical costs for mild to moderate presentation and severe presentation are HKD 1,026,208 (USD 131,565) and HKD 3,488,203 (USD 447,206) respectively, the total spending for unscreened PTPS deficiency patients adds up to HKD 20,773,207 (USD 2,663,232) per year (per 1.69 patients).
The annual cost of operating an expanded NBS programme was estimated to be HKD 10,473,848 (USD 1,342,801). If the lifetime medical cost for every screened PTPS deficiency patient is HKD 393,859 (USD 50,495), and for 1.69 patients screened each year, the total lifetime medical cost is HKD 666,609 (USD 85,463), the total spending is HKD 11,140,457 (USD 1,428,264) per year. Therefore, a total of HKD 9,632,750 (USD 1,234,968) per year would be saved by the expanded NBS programme (Table 3).
Discussion
For outcome comparison and the assessment of effectiveness, a randomized controlled trial is considered to be the gold standard. However, it is impractical to conduct such a trial in rare diseases. Therefore, a cross-sectional study is usually used.30,32–35 Two United Kingdom Health Technology Assessment systematic reviews in 199734,39 concluded that screening for PKU is cost-effective. The life-long cost of taking care of one cerebral palsy patient, including medical charges, developmental services, special education, and lost wages, is estimated be up to 1 million USD as of 1998. 40 In comparison, the cost of MS/MS screening accounting for laboratory expenditure and staffing in the local setting was only about HKD 209 (USD 26.9) per newborn.
There has been no single previous study evaluating the cost effectiveness of PTPS deficiency screening. NBS has successfully reduced the prevalence of childhood mental retardation. 41 Through expanded NBS, more treatable causes of mental retardation can be detected in the asymptomatic phase, thus preventing costly lifelong disability. In our study, we have demonstrated that the cost-not-to-screen, at HKD 20.77 million (USD 2.66 million), is 1.9-fold higher than the cost to screen at HKD 11.14 million (USD 1.43 million). The cost-to-screen per infant is HKD 209 (USD 26.9) excluding the annual medical cost for treating positive cases. The cost-to-screen includes implementation and operational costs of such a programme, as well as the medical expenditure on the positive cases. As the MS/MS assays can detect other disorders in addition to hyperphenylalaninemia, the annual saving would in fact be greater. Our study proves that an expanded NBS programme is cost-beneficial when implemented in Hong Kong.
The major principles in decision making for population screening are outlined by two landmark reports issued by World Health Organization.42,43 When considering IEM, however, the Wilson and Jungner criteria are often not adequate, compared with a cost-effective analysis. The first criterion states that the condition being sought should be an important health problem, and implies that a rare disease is not justified for population screening as large numbers would have to be screened before one positive case can be identified. Cost effectiveness analysis for a given IEM, however, evaluates multiple factors, including disease incidence, frequency of symptomatic patients detected and adverse outcomes without screening, sensitivity and specificity of the screening test, harms of false positive results, costs of screening, recall and confirmatory tests, benefits and reduction of cost with screening and early treatment. Cost effectiveness analysis compares the cost of screening with the cost of not screening.
When the cost of screening is affordable, and early diagnosis leads to a significant outcome improvement, screening is still considered to be cost-effective despite the low incidence of the disorder in question (in this example, phenylketonuria). The majority of PKU patients have moderate to severe mental retardation (intelligence quotient below 50). There are considerable data showing that the cost-to-screen is substantially exceeded by the cost-to-treat in unscreened patients.23,24,30,34,44–48 There are claims that some patients may not have irreversible mental retardation, that less long-term institutionalization is now preferred, and that the requirement for lifelong expensive treatment may reduce the cost-effectiveness of screening,49–51 but our data still show that the cost-not-to-screen is 1.9-fold of the cost-to-screen.
There is a lack of data concerning the natural course for the unscreened PTPS deficiency patients in Hong Kong. In our study, the social outcomes for these patients were only determined by gross group prediction. One in six patients in our study suffered from severe mental retardation. A recent study in Mainland China estimated that only 37.3% of patients had an intelligence quotient below 85, but did not indicate the proportion requiring long-term residential care, and their figures included diseases other than PTPS deficiency and those already picked up by an expanded NBS programme. 52 Other studies have reported that delayed diagnosis and treatment could result in severe disability in 80% of patients in whom PTPS deficiency is the main genetic defect.21,22
It is usually recommended that indirect costs (for which there is no payment made but for which a cost nonetheless exists) should be included in economic evaluation studies for health policies.53–55 In our calculations there would have been an annual saving of HKD 1,401,643 (USD 179,698) if the indirect costs of loss in productivity were excluded, however, we included the indirect costs because the disorder for which we were screening (PTPS deficiency), is readily treatable and the indirect costs incurred by the medical condition due to permanent neurological damage are significant. The long-term sequelae of this disorder are easily preventable by tetrahydrobiopterin, L-dopa and 5-hydroxytryptophan replacement and dietary management, and patients can essentially assume a normal life. When compared with acquired medical conditions, or those of complex genetic traits, there are also fewer uncertainties in autosomal recessive inherited metabolic diseases with regard to the penetrance, prognosis and treatment response. Penetrance is usually high, while rehabilitation or medical intervention could not reverse existing damages caused by phenylalanine accumulation.
The study has limitations, due to several unavoidable assumptions utilized in the calculation. Only the operational costs for the expanded NBS programme were taken into account. There may be some overestimate of the costs of reagents and consumables, as a lower price may be achievable by bulk procurement. However, the estimated savings were significant, and the expanded NBS programme is a cost-beneficial public health strategy.23,24,29,30,32,34,35,37,40,56–64 Using MS/MS, more than 30 different IEM can detected in addition to hyperphenylalaninemias; by incorporating these additional disorders into the screening panel the savings are likely, as suggested by Cipriano et al, 62 even greater.
Estimated medical costs for unscreened and screened PTPS deficiency patients.
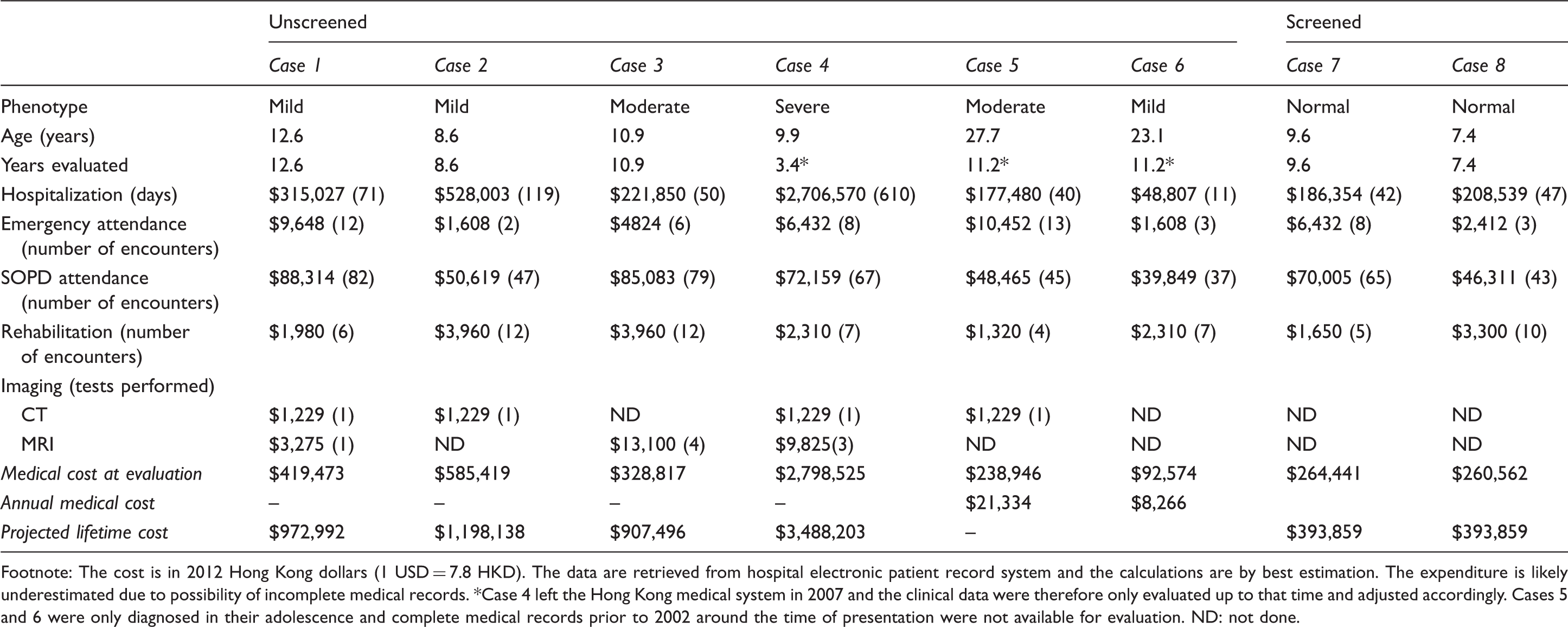
Footnote: The cost is in 2012 Hong Kong dollars (1 USD = 7.8 HKD). The data are retrieved from hospital electronic patient record system and the calculations are by best estimation. The expenditure is likely underestimated due to possibility of incomplete medical records. *Case 4 left the Hong Kong medical system in 2007 and the clinical data were therefore only evaluated up to that time and adjusted accordingly. Cases 5 and 6 were only diagnosed in their adolescence and complete medical records prior to 2002 around the time of presentation were not available for evaluation. ND: not done.
Cost-benefit analysis of expanded NBS programme in Hong Kong.
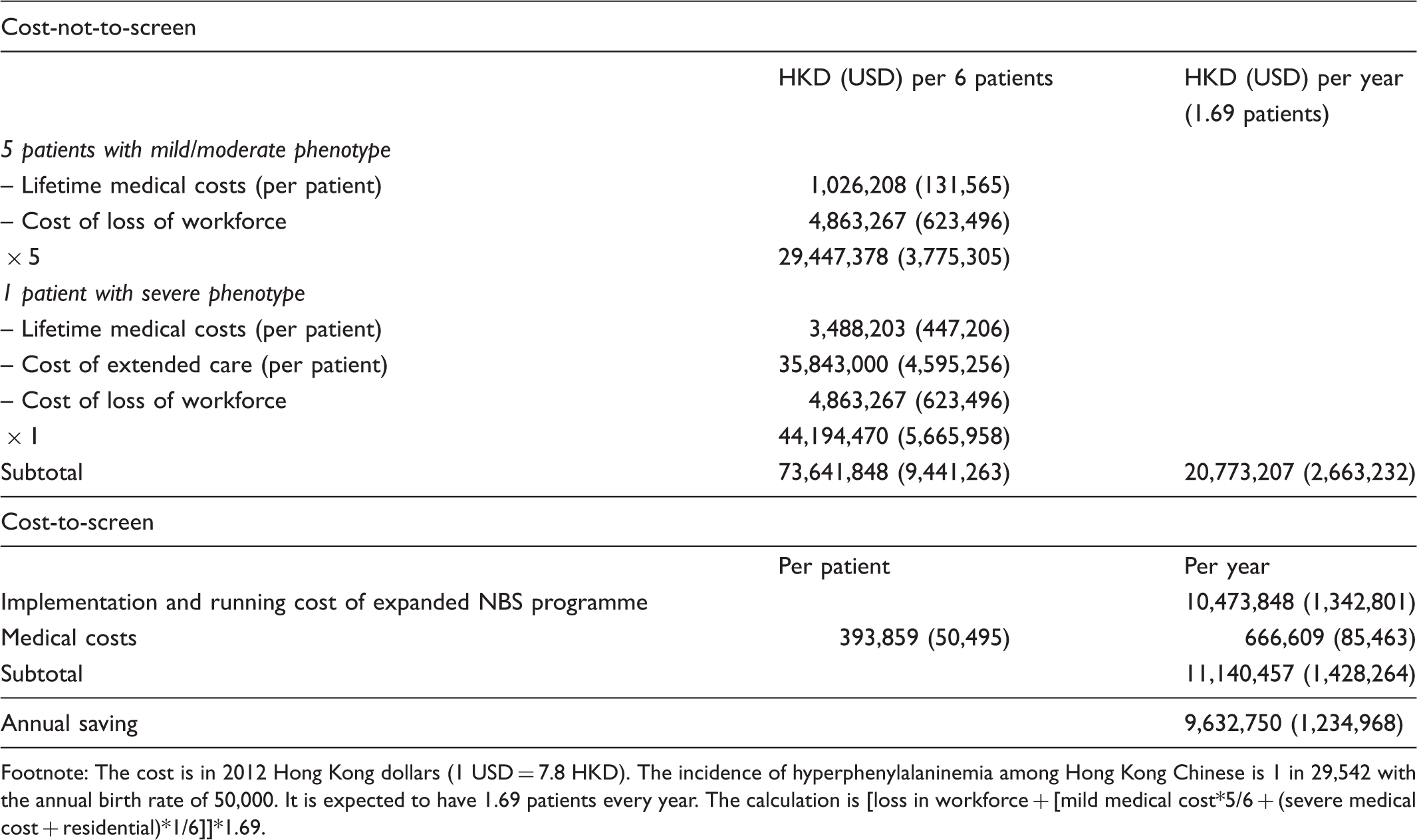
Footnote: The cost is in 2012 Hong Kong dollars (1 USD = 7.8 HKD). The incidence of hyperphenylalaninemia among Hong Kong Chinese is 1 in 29,542 with the annual birth rate of 50,000. It is expected to have 1.69 patients every year. The calculation is [loss in workforce + [mild medical cost*5/6 + (severe medical cost + residential)*1/6]]*1.69.
PTPS deficiency screening in newborns, with MS/MS-based screening, is proven to be a cost-beneficial programme.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgement
We are indebted to Dr Scott Grosse, senior health economist at the National Center on Birth Defects and Developmental Disabilities, USA Centers for Disease Control and Prevention, for his invaluable comments on our study design and the final manuscript.