
Abstract
Background
The incidence of inborn errors of metabolism varies widely across countries. Very few studies have analyzed the incidence of these disorders in Mainland China. We aimed to estimate the overall and disease-specific incidences of inborn errors of metabolism in Chinese newborns and investigate the geographical distribution of these disorders.
Methods
A national cross-sectional survey was conducted to investigate newborn inborn errors of metabolism screening by tandem mass spectroscopy in Mainland China between 2016 and 2017. A total of 246 newborn screening centers were surveyed using a standardized questionnaire. We examined the cumulative and disease-specific incidences of inborn errors of metabolism in Mainland China as a whole and in different geographical locations.
Results
Over 7 million newborns were screened and 2747 were diagnosed with inborn errors of metabolism, yielding an overall incidence of 38.69 per 100,000 births (95% confidence interval: 37.27–40.17). The most common disorders were amino acid disorders (17.14 per 100,000 births, 95% confidence interval: 16.21–18.13), followed by organic acid disorders (12.39 per 100,000 births, 95% confidence interval: 11.60–13.24) and fatty acid oxidation disorders (9.16 per 100,000 births, 95% confidence interval: 8.48–9.89). The overall and disease-specific incidence rates differed significantly across geographical locations (P < 0.001).
Conclusions
The overall incidence of inborn errors of metabolism in Chinese newborns is relatively high. It is urgent to establish the recommended uniform screening panel for inborn errors of metabolism to guide the national and regional tandem mass spectroscopy newborn screening programs.
Introduction
Inborn errors of metabolism (IEM) comprise a diverse group of disorders primarily caused by defects in a specific enzyme, cofactor, or transporter involved in a particular metabolic pathway, resulting in metabolic malfunction and/or the accumulation of toxic intermediate metabolites. Most of these disorders may lead to serious consequences for the affected neonates, such as lethargy, irreversible mental retardation, physical handicaps, autism, and even death.1,2 Expanded newborn screening programs by tandem mass spectrometry (MS/MS) have been implemented in most developed and developing countries to facilitate the early diagnosis and presymptomatic treatment of IEM and substantially reduce the morbidity and mortality associated with these diseases. 3
While individually rare, the cumulative incidence of IEM has been shown to be around 1 in 800 live births. 4 A 2018 systematic review of studies primarily conducted in high-income countries reported that the estimated birth prevalence of all-cause inborn metabolic disorders globally was 50.9 per 100,000 live births. 5 The incidence of inborn metabolic disorders substantially varies between and within countries, depending on the disorders screened for, neonatal screening programs used, diagnostic approaches adopted, and clinical follow-up services available. Moreover, genetic heterogeneity among populations also contributes to variation in the incidence of IEM. 6
The number and subtype distribution of IEM screened by MS/MS varies across countries. 7 Understanding the disease-specific incidence of IEM in a region or country is important for implementing effective expanded newborn screening programs by MS/MS, particularly in developing regions or countries. However, there is a lack of data on the frequency and disease-specific incidence of IEM in Asian populations, despite the fact that expanded newborn screening programs by MS/MS were implemented in Asia a number of years ago. A limited number of small-scale and pilot studies have estimated the cumulative and disease-specific incidences of IEM in Singapore, Malaysia, India, Taiwan, South Korea, and Japan.8–13
In Mainland China, expanded newborn screening programs by MS/MS were implemented as a pilot project in Shanghai in early 2003 and in Zhejiang and Guangdong later.14,15 As of 2017, this program has been individually implemented in more than 100 advanced newborn screening centers, approximately accounting for half of all centers, which were mainly distributed in the developed areas (data from an unpublished report). Currently, MS/MS newborn screening is not mandatory, and there are no uniform technical specifications for IEM screened by MS/MS in China. Each of the newborn screening centers set the screening panel by MS/MS based on their respective incidence of IEM. Although expanded newborn screening programs by MS/MS were recommended for all babies, participation was voluntary, and the screening test was often given as a chargeable service. The charge for MS/MS screening was approximately US $50–100 per infant.14–16 A pilot study of 371,942 neonates from four newborn screening centers in eastern China previously estimated the overall incidence of IEM to be 1 in 3795 live births. 16 Later studies also reported the incidence of IEM among high-risk populations and in local regions.15,17,18 However, there is a lack of knowledge about the incidence of these disorders at the national level.
The present study aimed to estimate the overall and disease-specific incidences of IEM screened by MS/MS in Chinese newborns using data from a nationwide cross-sectional survey and to investigate the geographical distribution of IEM in Mainland China.
Materials and methods
Data sources
The data used in our analysis were sourced from the 2018 Chinese MS/MS Newborn Screening Cross-sectional Survey. This survey was authorized by the National Health Commission of China and was the first national survey conducted to assess the implementation of MS/MS newborn screening programs in Mainland China between 2016 and 2017. As of 2018, a total of 246 newborn screening centers (31 provincial-level and 215 city-level centers) were authorized and administered by provincial health departments, and they all participated in this survey. Provincial-level centers were responsible for guiding and supervising all neonatal screening practices at city-level centers. Each center was responsible for IEM screening, diagnosis, treatment, and follow-up in a specific region. Besides these newborn screening centers, some other hospitals and commercial laboratories have also carried out MS/MS newborn screening programs. However, we could not know how many such facilities have implemented these programs. Therefore, these facilities were not included in this survey and newborns who were screened at them were excluded from our analysis. The study was approved by the Ethics Committee of Sichuan University, China.
Measures
A standardized questionnaire was used to collect information on the implementation of MS/MS newborn screening programs, the number of newborns screened, and the number of newborns affected by each disorder. The questionnaires were filled in and checked by staff from each newborn screening center and were then sent to the National Office of Maternal and Child Health Surveillance, where a group of national experts comprising metabolic specialists, epidemiologists, and statisticians reviewed and evaluated the quality of the data. If unqualified, the data were required to be rechecked by staff from the corresponding center by telephone interview.
The diseases analyzed in this survey included amino acid disorders, organic acid disorders, and fatty acid oxidation disorders, which were detected by measuring acylcarnitines and amino acids by MS/MS. Often, cases of these disorders were diagnosed by experienced metabolic specialists at each center. Those more complicated were referred to provincial-level centers for confirmatory testing. In our analysis, cases with hyperphenylalaninemia were those who were detected by MS/MS screening and included mild hyperphenylalaninemia, phenylketonuria, and tetrahydrobiopterin deficiency. The cutoff value for hyperphenylalaninemia was 120 µmol/L according to the 2010 Technological Guideline on National Newborn Screening in China.
Statistical analysis
In our analysis, 31 provinces were classified into seven regions according to geographical location and socioeconomic status: northeast (Heilongjiang, Jilin, and Liaoning), east (Anhui, Fujian, Jiangsu, Jiangxi, Zhejiang, Shandong, and Shanghai), north (Beijing, Hebei, Inner Mongolia, Shanxi, and Tianjin), central (Henan, Hubei, and Hunan), south (Guangdong, Guangxi, and Hainan), northwest (Gansu, Ningxia, Qinghai, Shaanxi, and Xinjiang), and southwest (Chongqing, Guizhou, Sichuan, Tibet, and Yunnan) regions of China (Figure 1). The overall and disease-specific incidence rates of inborn metabolic disorders, expressed as the number of cases per 100,000 live births, were calculated by dividing the number of observed cases by the number of newborns screened. Following this, 95% confidence intervals (CIs) were calculated for these incidence rates assuming a Poisson distribution. Chi-square tests were performed to compare the incidence rates of specific disorders among regions. All statistical analyses were performed using SAS 9.1 software (SAS Institute Inc., Cary, NC, USA).
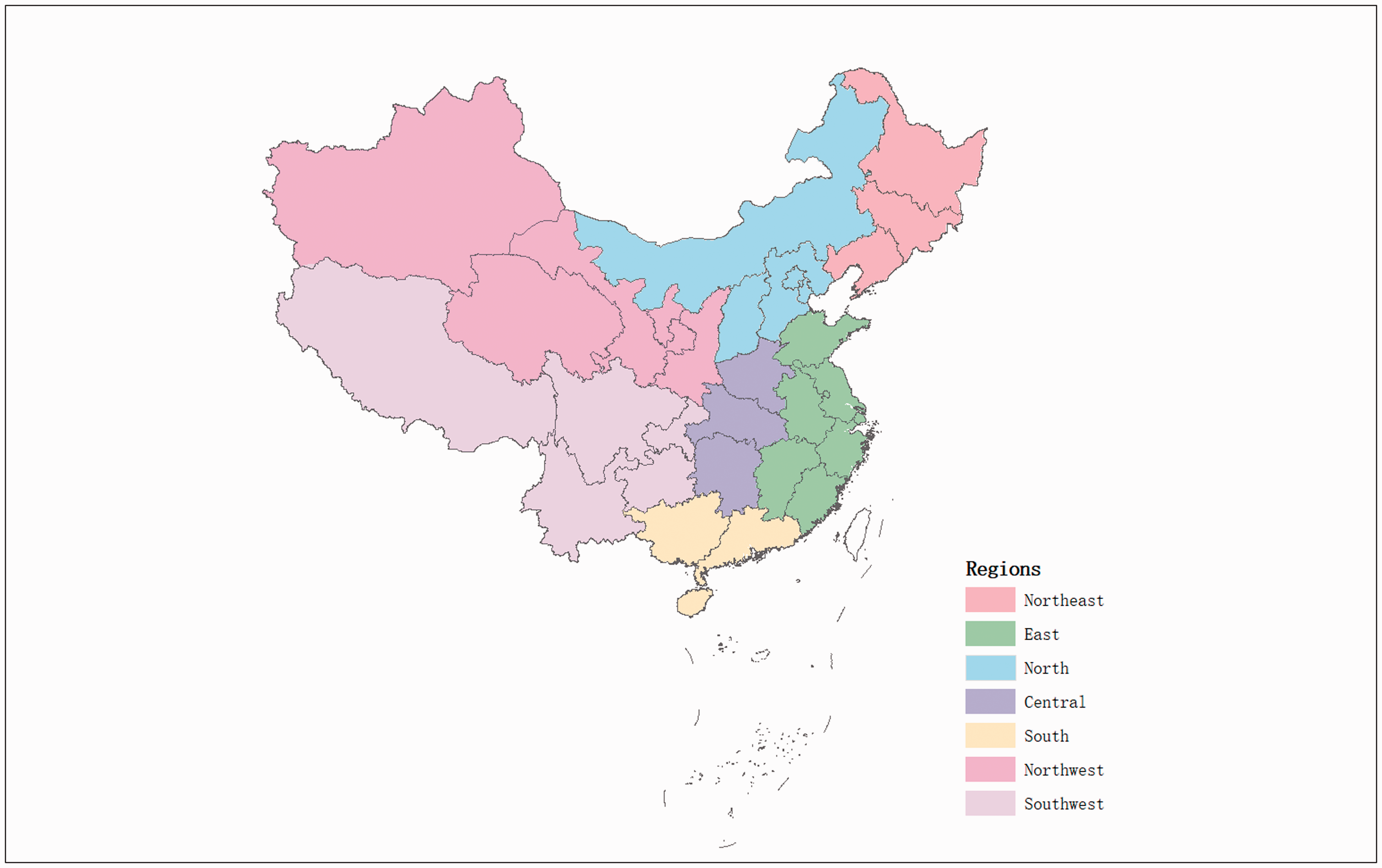
The geographical locations of 31 provinces in Mainland China.
Results
Between January 2016 and December 2017, over 7 million newborns were screened for amino acid, organic acid, and fatty acid oxidation disorders by MS/MS in Mainland China, accounting for approximately one-fifth of all live births who were born during the two-year survey period. A total of 2747 cases were identified, resulting in an overall incidence rate of 38.69 per 100,000 births (95% CI: 37.27–40.17). Overall, 1217 newborns had amino acid disorders (incidence 17.14 per 100,000, 95% CI: 16.21–18.13), 880 had organic acid disorders (incidence 12.39 per 100,000, 95% CI: 11.60–13.24), and 650 had fatty acid oxidation disorders (incidence 9.16 per 100,000, 95% CI: 8.48–9.89).
The number of screened newborns and cumulative and disease-specific incidence rates according to geographical location are presented in Table 1 and Figure 2. Most newborns screened by MS/MS were located in the east, while only a very small proportion was located in the northeast and southwest. The cumulative incidence rate of IEM was highest among newborns in the northwest due to the high incidence of amino acid disorders noted in that region. The highest incidence rate of organic acid disorders was noted among newborns in the southwest, while the highest rate of fatty acid oxidation disorders was found among newborns in the south. The lowest cumulative and disease-specific incidence rates were observed among newborns in the northeast. The cumulative incidence rate and all disease-specific incidence rates differed significantly across regions (P < 0.001).
Incidence of inborn errors of metabolism detected by tandem mass spectrometry according to geographical location and by disorder type in China between 2016 and 2017.
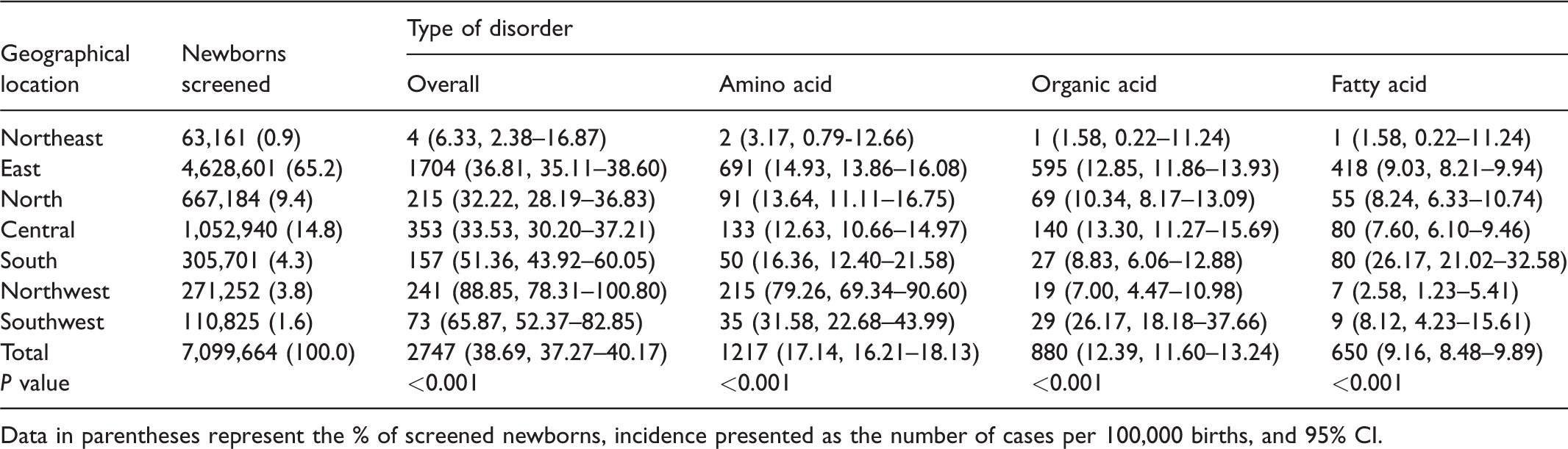
Data in parentheses represent the % of screened newborns, incidence presented as the number of cases per 100,000 births, and 95% CI.
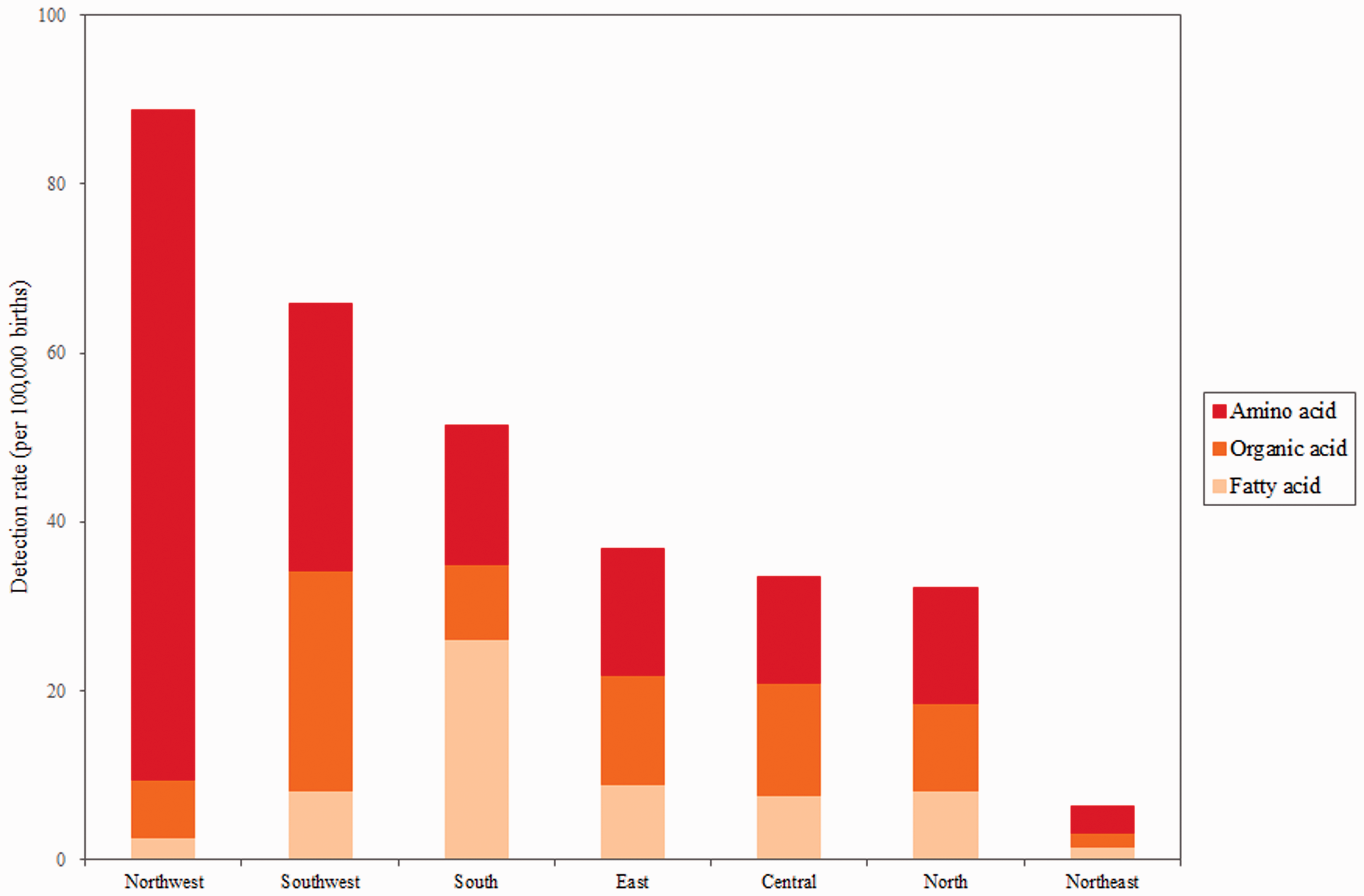
The incidence of inborn errors of metabolism detected by tandem mass spectrometry according to geographical location and disorder type in China between 2016 and 2017.
Table 2 shows the incidence of each type of metabolic disorder across all regions analyzed. Overall, 36 metabolic disorders were detected—14 amino acid disorders, 11 organic acid disorders, and 11 fatty acid oxidation disorders. Hyperphenylalaninemia was the most common of all screened disorders, and the incidence rate of this disorder was highest among newborns in the northwest, followed by those in the southwest and east. Methylmalonic acidemia was the second most common disorder, and the incidence rate of this disorder was highest among newborns in the southwest, followed by those in central China, the east, and the north. Primary carnitine deficiency was the most common fatty acid oxidation disorder, and the incidence of this disorder was highest among newborns in the south. Additionally, only one case of nonketotic hyperglycinemia, two cases each of hyperornithinemia, biotinidase deficiency, long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency, and medium-chain acyl-CoA thiolase deficiency, and three cases each of β-ketothiolase deficiency and ethylmalonic encephalopathy were detected.
Incidence of inborn errors of metabolism detected by tandem mass spectrometry according to the disorder subtype and geographical location in China between 2016 and 2017.
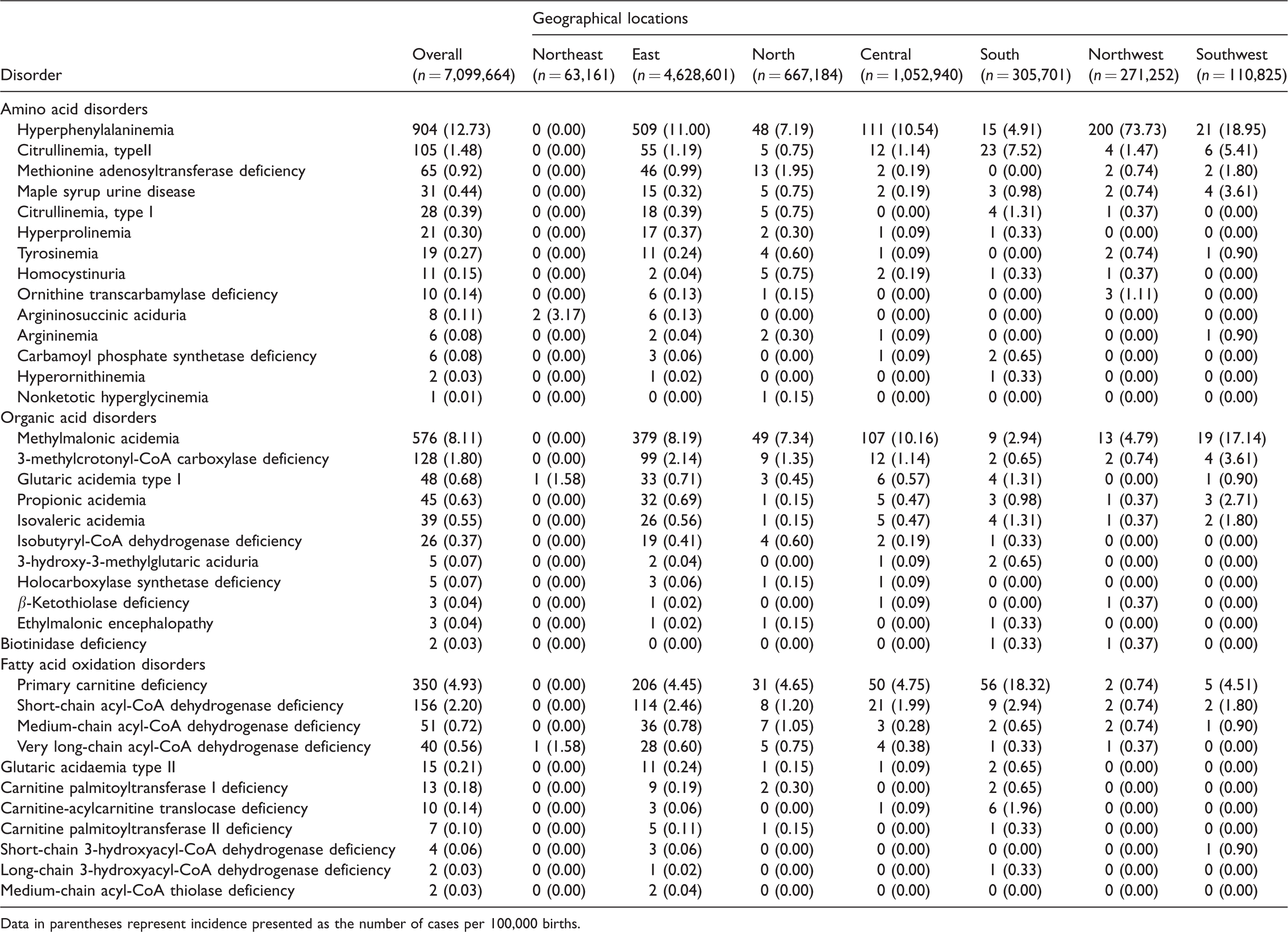
Data in parentheses represent incidence presented as the number of cases per 100,000 births.
Discussion
To date, this is the largest nationwide cross-sectional study to estimate the overall incidence of a wide range of inborn metabolic disorders in Chinese newborns using national data from expanded newborn screening programs by MS/MS. This study also demonstrates that the subtype distribution incidence of IEM differs according to geographical location.
Although MS/MS newborn screening programs have been widely implemented in many developed countries, there is a lack of data on the incidence of inborn metabolic disorders among newborns. The overall incidence of inborn metabolic disorders recorded in our study (38.7 cases per 100,000 births) is similar to that reported in Malaysia (34.3 cases per 100,000 births), 11 South Korea (35.7 cases per 100,000 births), 12 and Germany (42.4 cases per 100,000 births for amino acidemias, organic acidurias, and fatty acid oxidation disorders). 19 Another study conducted in the West Midlands, United Kingdom using retrospective data collected over five years reported a slightly higher rate (47.0 cases per 100,000 births) of inherited metabolic disorders, mostly owing to the greater number of disorders detected as a result of advances in diagnostic technology and the long clinical follow-up period. 20 However, due to differences in the populations studied and screening programs in place, the incidence rate of inborn metabolic diseases is reportedly lower in California (31.7 cases per 100,000 births), 6 North Carolina (23.3 cases per 100,000 births), 21 British Columbia (22.7 cases per 100,000 births), 22 Taiwan (16.08 cases per 100,000 births), 13 and Italy (8.51 cases per 100,000 births). 23 Additionally, a study in Australia reported that the prevalence rate of inborn metabolic disorders, excluding phenylketonuria, was 15.7 per 100,000 births. 3
Amino acid disorders were the most common disorders detected by MS/MS screening in our study, which is in line with the most previous studies.12,13,19,20 However, other studies found that organic acid and fatty acid oxidation disorders were more common than amino acid disorders.6,10 The incidence rate of amino acid diseases in our study (17.1 per 100,000) was lower than that in Germany (26.3 per 100,000) and the United Kingdom (26.7 per 100,000), but higher than that in California (9.3 per 100,000). These differences may be a consequence of multiple factors, such as differences in population ethnicity, diagnostic technology, and screening laboratory capacity (e.g. the set of cutoff values, the recall rate of suspected positive cases, and the screening panel). Through MS/MS screening, more newborns affected by organic acid and fatty acid oxidation disorders will be diagnosed within the first few days of life than diagnosed after clinical presentation, as demonstrated by Wilcken et al. 3 Similarly, a significant variation in the incidence of these disorder subtypes among newborns was noted across countries or regions. For example, the incidence of fatty acid oxidation disorders was reported to be 9.2 per 100,000 in our study, 7.7 per 100,000 in the United Kingdom, 20 9.6 per 100,000 in Germany, 19 and 13.1 per 100,000 in California. 6
The overall and disease-specific incidence of inborn metabolic disorders significantly differed across geographical regions in our study. The cumulative incidence of IEM was highest in newborns in the northwest, followed by those in the southwest and south. The incidence rate of each individual disorder also varied widely across regions. Newborns in the northwest were most likely to be affected by hyperphenylalaninemia, the most common amino acid disorder. This finding is consistent with a recent Chinese study 24 that showed that the incidence of phenylketonuria was highest in the provinces of Gansu, Ningxia, and Qinghai of China and may be related to the high proportion of minority groups residing in this region who are known to have a high risk of hyperphenylalaninemia. 25 Due to high sensitivity and specificity for MS/MS screening, the incidence of hyperphenylalaninemia in our study (12.7 per 100,000) is higher than those reported in the two previous studies in China, during which hyperphenylalaninemia was screened by the fluorometric method and quantitative enzymatic method and the rates of hyperphenylalaninemia were both around 8.5 per 100,000.14,16 Similarly, the highest incidence rates of methylmalonic acidemia and primary carnitine deficiency were noted in the southwest and south, respectively. These inconsistencies may be related to ethnic genetic differences and some other factors, including differences in the coverage rate for MS/MS screening, the recall rate of suspected positive cases, and the screening panel between regions. For instance, both the coverage rate for MS/MS screening and the positive recall rate were close to 100% in some local areas in the east, such as Quanzhou, 26 Suzhou, 27 and Zhejiang. 28 By contrast, according to our survey, the average coverage rate in the western regions was very low at less than 10% of live births, while the positive recall rate was also lower, at only about 70%.
A few limitations of our study should be considered. First, as a voluntary chargeable program in China, the MS/MS newborn screening coverage rate was low in the central and west regions because of poor medical and socioeconomic conditions. Consequently, the estimated incidence of inborn metabolic disorders in our study may not accurately represent the incidence in newborns in these regions. Second, there is no uniform panel of metabolic disorders screened by MS/MS throughout China. Therefore, the panel of disorders screened for may have varied between centers, although most common disorders were screened for at most centers. This means that the incidence of certain rarer disorders may have been under-reported in our analysis. Third, because each center had their respective screening panel for inborn metabolic disorders, some conditions that are not recommended for screening in developed countries were included, such as 3-methylcrotonyl-CoA carboxylase deficiency, nonketotic hyperglycinemia, and short-chain acyl-CoA dehydrogenase deficiency. This would overestimate the overall incidence of disorders that could be detected by MS/MS. More caution is needed to make international comparisons about the overall incidence of inborn metabolic disorders. Last, most newborns who tested positive for an inborn metabolic disorder were referred to a provincial newborn screening center for diagnosis and treatment, but a few may have been referred to other specialist hospitals. We were unable to acquire data on patients diagnosed at specialist hospitals, so the incidence of inborn metabolic disorders may have been underestimated. Therefore, coordinated management of the diagnosis, treatment, and follow-up of patients referred to specialist hospitals should be a focus of future research.
Conclusions
In conclusion, the overall incidence of inborn metabolic disorders in Chinese newborns is relatively high, although currently not all newborns are screened by MS/MS at birth in Mainland China. Many cases with IEM can be detected early through expanded newborn screening by MS/MS. The cumulative and disease-specific incidence of IEM varies widely across regions, given the different ethnic populations, the inconsistent screening panels, and some other factors. It is urgent to establish a recommended uniform screening panel for IEM to guide the national and regional MS/MS newborn screening programs.
Supplemental Material
sj-pdf-1-msc-10.1177_0969141320973690 - Supplemental material for Incidence of inborn errors of metabolism detected by tandem mass spectrometry in China: A census of over seven million newborns between 2016 and 2017
Supplemental material, sj-pdf-1-msc-10.1177_0969141320973690 for Incidence of inborn errors of metabolism detected by tandem mass spectrometry in China: A census of over seven million newborns between 2016 and 2017 by Kui Deng, Jun Zhu, Erling Yu, Liangcheng Xiang, Xuelian Yuan, Yongna Yao, Xiaohong Li and Hanmin Liu in Journal of Medical Screening
Footnotes
Acknowledgements
The authors would like to thank the staff of the newborn screening centers for their continued collaboration and support with respect to the collection and rechecking of data.
Authors’ contributions
KD, JZ, XHL, and HML contributed to the study design. KD, ELY, LCX, XLY, and YNY helped in the data collection and reviewing. KD and XHL contributed to the data analysis and interpretation. KD wrote the first draft of the manuscript. All authors reviewed and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Ethics Committee of Sichuan University, China.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (2017YFC1001700 & 2018YFC1002200).
Patient consent statement
Patients were not involved in the design of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.