
Abstract
Objectives
To estimate the burden of metabolic disorders detectable by tandem mass spectrometry in Egypt, through a pilot expanded newborn screening programme at Cairo University Children's Hospital in 2008, and examining the results of 3,900 clinically at-risk children, investigated at Cairo University Children’s Hospital for the same disorders over the past 7 years using the same technology.
Methods
Dried blood spots of 25,276 healthy newborns from three governorates in Upper, Middle, and Lower Egypt were screened, to give a representative sample of the Egyptian newborn population. Based on the pilot study outcomes and the results of clinically suspected children, we estimated the total birth prevalence of tandem mass spectrometry detectable metabolic disorders, and the relative frequency of several individual disorders.
Results
Among the healthy newborns, 13 metabolic disorder cases (five phenylketonuria [1:5,000], two methylmalonic acidemia, and isovaleric acidemia [1:12,500], one each of maple syrup urine disease, propionic acidemia, β-ketothiolase deficiency, and primary carnitine deficiency [1:25,000]) were confirmed, giving a total birth prevalence of 1:1944 live births. Among the clinically suspected children, 235 cases were diagnosed, representing a much wider disease spectrum.
Conclusions
Egypt has one of the highest reported birth prevalence rates for metabolic disorders detectable by tandem mass spectrometry. Early diagnosis and management are crucial for the survival and well-being of affected children. A nationwide NBS programme by tandem mass spectrometry is recommended.
Introduction
The main aim of newborn screening (NBS) is to prevent morbidity and mortality. Since the pioneering work of Guthrie and Susi 1 in the diagnosis of phenylketonuria (PKU) using neonatal dried blood spots, additional inherited disorders, including congenital hypothyroidism, biotinidase deficiency, cystic fibrosis, galactosaemia, and maple syrup urine disease (MSUD), have been included in NBS. 2 Tandem mass spectrometry (MS/MS), characterized by high sensitivity, specificity, throughput, and a low sample volume (a single blood spot), 3 is now routinely used to screen for several aminoacidopathies, organic acid disorders, and fatty acid oxidation defects;4–6 however, the relatively high costs preclude its nationwide application in many developing countries. The NBS panel for each country, and sometimes for each region in the same country, varies according to the prevalence of each disorder in the target population, and the health care system funding policies. 7 Prevalence data are necessary tools to evaluate cost-effectiveness. 8 Developing countries face challenges in implementing and expanding their NBS programmes, including financial issues, medical and logistical support, society education, policy development, programme evaluation, and sustainability; 9 however, Egypt, a developing country with a population of over 85 million and an annual birth rate of about 2.5 million, 10 is one of the few African and Arab nations with a national NBS programme for congenital hypothyroidism (introduced in April 2000). 11
Due to the autosomal recessive nature of most metabolic disorders and the tradition of consanguineous marriage in the Arab region, higher prevalence rates of these disorders have been reported in Saudi Arabia and Lebanon.12,13 In response to the large number of children with manifestations suggestive of hereditary metabolic disorders referred to inpatient and outpatient sectors at Cairo University Children’s Hospital (CUCH), we conducted the first NBS pilot study for disorders detectable by MS/MS in Egypt. We calculated the needed sample size to detect the approximate total prevalence of these disorders in the Egyptian newborn population, and attempted to evaluate the relative frequency of individual disorders, based on the outcomes of the NBS pilot study and the CUCH selective screening programme established in 2008. Our results may assist Egyptian health policy makers to identify the magnitude of the problem and to reach decisions to address it.
Methods
Through the European Union funded programme for prevention, early detection and early intervention in Egyptian children with genetic disability and children at risk, an MS/MS pilot study was launched in January 2008 at CUCH, using the same dried blood spot cards adopted in the national NBS programme for congenital hypothyroidism taken at 3–7 days of age. From January to November 2008, 25,276 healthy newborns from three governorates in Upper, Middle, and Lower Egypt (8756 from Assiut, 8573 from Cairo, and 7947 from Kaliobeya, respectively) were screened, to give a representative sample of the Egyptian newborn population. The study was conducted in accordance with the ethical guidelines provided in the Helsinki declaration of human rights 1975 and as modified in 1989, and was approved by the ethical review board at CUCH.
We estimated our needed sample size based on the prevalence in Saudi Arabia, the closest country to our geographic distribution. The reported frequency of inborn errors of metabolism (IEMs) in the Saudi newborn population is 1:1381, 12 but as the consanguineous marriage rate in Saudi Arabia is higher than in Egypt, 14 we estimated our expected prevalence to be slightly lower. Based on the equation provided by Daniel 15 and the recommendations of Naing et al. 16 for calculating sample size in prevalence studies, we calculated a required newborn sample size of approximately 23,600 to derive a dependable total prevalence rate of disorders detectable by MS/MS. We increased this to above 25,000 to correct for minor calculation errors.
Blood spot samples were analyzed by a quadropole MS/MS with an electrospray ionization probe (Quattro Micro, Waters, Manchester, UK) using derivatized non-kit method for amino acids and acylcarnitines evaluation. Deuterated internal standards were purchased from Cambridge Isotope laboratories (Massachusetts, USA). Details of methodology, work flow, cut-off, and reference values in the Egyptian setting were described previously. 17 We performed internal and external validation of results. Three levels of a mixture of amino acids were prepared in-house to ensure reliable performance, and we participated in CDC NBS quality assurance programme (NSQAP) for both quality control and proficiency testing samples. Our laboratory was also the first in Africa to join and submit data to the international region 4 genetics project.18,19 Newborn samples flagged positive on primary screening were repeated in duplicate in a second run. If proven abnormal, the infant was called to visit the inherited metabolic disease unit (IMDU) at CUCH for clinical evaluation and confirmatory testing.
Before and during the pilot study period, we performed six awareness workshops for junior paediatricians and nurses at CUCH, and for ministry of health medical personnel in the governorates included in the study. A tracking system for positive cases was established for immediate referral to the metabolic centre, for medical assessment and early intervention by the paediatric metabolic team at CUCH. All confirmed cases were documented and submitted to the centre database. Full instructions were given to parents regarding proper dietary protocols, and the supply of dietary formulas for patients’ management was provided during and after the study period through the IMDU. Paediatricians caring for positive cases in distant locations were provided with cell phone numbers and email addresses of paediatric and laboratory metabolic specialists at CUCH, in case they needed any help in patients’ management. Patients and their parents were given the opportunity to attend metabolic classes, and to see older patients who had not received NBS, to observe the full effect of the diseases, because some Egyptian parents initially refused to give dietary formulas to their apparently healthy neonates.
From January 2008 to January 2015, about 3900 dried blood spot samples were obtained from children (1 week to 15 years) presenting to the inherited metabolic clinic at CUCH from all over Egypt with suspected IEMs. The clinical presentations and complications of the diagnosed disorders were described previously. 20
Results
Cases detected by MS/MS among 25,276 healthy Egyptian newborns.
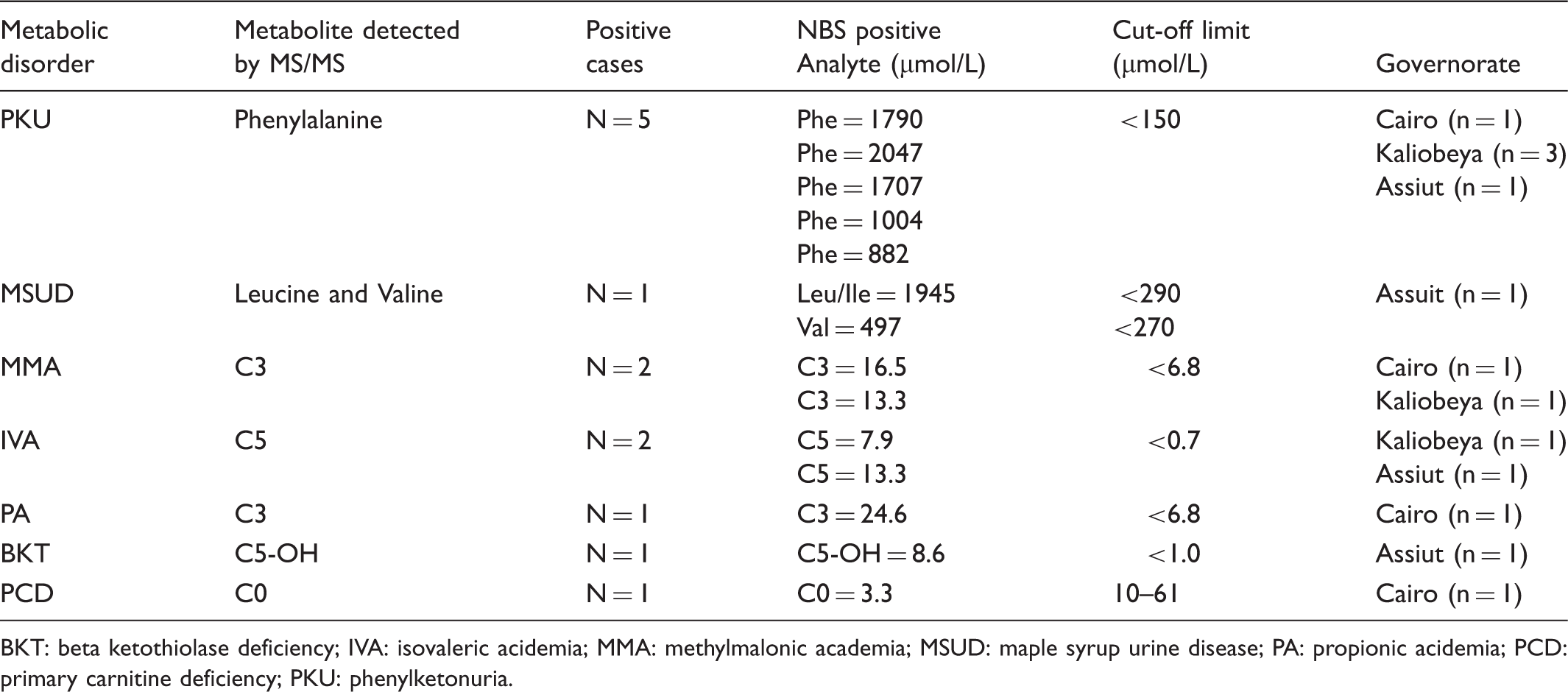
BKT: beta ketothiolase deficiency; IVA: isovaleric acidemia; MMA: methylmalonic academia; MSUD: maple syrup urine disease; PA: propionic acidemia; PCD: primary carnitine deficiency; PKU: phenylketonuria.
During the study period, 38 samples were flagged on initial screening (15/10,000), giving an initial false positive rate of 10/10,000. After the samples were repeated in duplicate only 31 remained flagged in at least two runs, and were recalled to the IMDU for clinical evaluation, giving a total recall rate of 12/10,000. Thirteen cases were confirmed and 18 cases were found to have non-significant elevations (7.3/10,000). True positive cases constituted 42% of those recalled, which is reasonable for a multiplex NBS programme. False positive rates were much higher for certain analytes, such as C3, C5-OH, and Tyrosine (together these constituted about 72% of non-significant elevations upon recall). Using ratios such as C3/C2, C3DC/C10, Phe/Tyr, and Leu/Phe can reduce the false positive rate of some analytes, especially C3; however, they were introduced later in our laboratory during the course of the clinically orientated study, and we therefore expect now to have lower false positive rates. To our knowledge, none of the healthy newborns who screened negative during our pilot study manifested later with a disease detectable by MS/MS.
Estimated birth prevalence of different IEMs detectable by MS/MS in a hypothetical annual Egyptian newborn cohort.
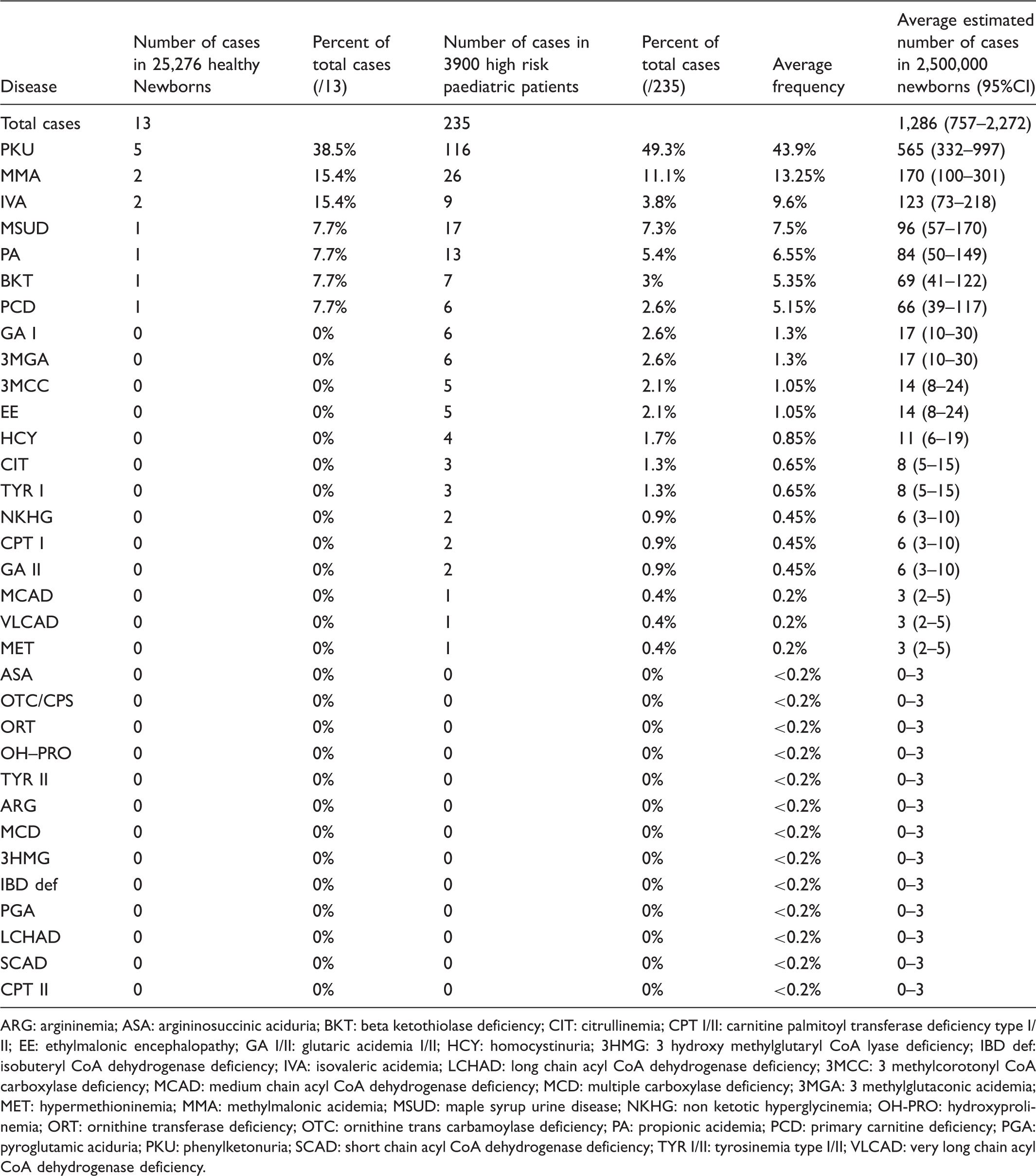
ARG: argininemia; ASA: argininosuccinic aciduria; BKT: beta ketothiolase deficiency; CIT: citrullinemia; CPT I/II: carnitine palmitoyl transferase deficiency type I/II; EE: ethylmalonic encephalopathy; GA I/II: glutaric acidemia I/II; HCY: homocystinuria; 3HMG: 3 hydroxy methylglutaryl CoA lyase deficiency; IBD def: isobuteryl CoA dehydrogenase deficiency; IVA: isovaleric acidemia; LCHAD: long chain acyl CoA dehydrogenase deficiency; 3MCC: 3 methylcorotonyl CoA carboxylase deficiency; MCAD: medium chain acyl CoA dehydrogenase deficiency; MCD: multiple carboxylase deficiency; 3MGA: 3 methylglutaconic acidemia; MET: hypermethioninemia; MMA: methylmalonic acidemia; MSUD: maple syrup urine disease; NKHG: non ketotic hyperglycinemia; OH-PRO: hydroxyprolinemia; ORT: ornithine transferase deficiency; OTC: ornithine trans carbamoylase deficiency; PA: propionic acidemia; PCD: primary carnitine deficiency; PGA: pyroglutamic aciduria; PKU: phenylketonuria; SCAD: short chain acyl CoA dehydrogenase deficiency; TYR I/II: tyrosinemia type I/II; VLCAD: very long chain acyl CoA dehydrogenase deficiency.
Discussion
The birth prevalence of metabolic disorders detectable by MS/MS varies greatly in different NBS studies. In the United States it ranges from 1:3367 in California 21 to 1:4310 in North Carolina. 4 Most Northern European countries have a similar birth prevalence to the United States (e.g. Germany 1:3315 22 ). In Southern Europe it is higher (e.g. Italy 1:2105 23 and Spain 1:2060 2 4 ). The lowest reported birth prevalence is in the Far East (Taiwan 1:6219 25 and Japan 1:9300 26 ), and the highest is in Arab nations, where consanguinity is much more common (Saudi Arabia 1:1381 12 and Lebanon 1:1482. 13 Based on our NBS data, Egypt has a high prevalence rate, similar to reported Arab and Mediterranean populations.
While 25,000 newborns is a relatively small cohort for an NBS pilot study, and most individual IEMs have a birth prevalence of less than 1:100,000, financial and logistical limitations meant we had to rely on the total prevalence rate rather than those of individual disorders. Furthermore, the IMDU clinic at CUCH receives patients from all over Egypt, so we assumed that the relative frequencies of different IEMs in the high-risk population can be also representative of their national frequencies, and can be used in association with the NBS pilot study frequencies to derive more dependable estimates of the expected burden of individual IEMs in Egypt, especially for the diseases not detected in the 25,000 screened healthy newborns. The approach is not perfect. Many symptomatic patients will not proceed as far as clinical diagnosis during childhood, either due to the rapid fatality of the disease or in milder cases because of later onset during adolescence or adulthood. However, we believe that the true burden of individual metabolic disorders in Egypt is not far from our estimates, presented in Table 2.
The estimated number of IEM cases in a hypothetical annual Egyptian birth cohort of 2.5 million newborns is 1286 (95% CI: 757–2272 IEMs patients). PKU cases are expected to constitute 40–50% of all MS/MS detected cases, with a prevalence of 1: 5000 live births. When considering that the birth prevalence of PKU ranges in the developed nations between 1:10,000 and 1:19,000 live births, 27 the effect of high consanguinity on PKU in Egypt is clear.
As with NBS results from ethnically similar populations to that of Egypt,12,13 fatty acid oxidation defects were uncommon in our Egyptian healthy and high-risk cohorts (7.7% and 5.1% of diagnosed patients, respectively). Primary carnitine deficiency (PCD) was the most common fatty acid oxidation defect, while medium chain acyl CoA dehydrogenase deficiency (MCAD), which approximates the birth prevalence of PKU in most western populations, was extremely rare in Egyptian patients.
Apart from determining the burden of metabolic disorders in Egypt, the current pilot study also aimed to gain practical experience in using the technology and evaluating the overall effectiveness of the new method when applied in an Egyptian setting. This experience would help to determine the disorders for which to screen and how best to incorporate the new technology into the existing mandatory NBS programme for congenital hypothyroidism in Egypt.
The debilitating clinical presentations of most IEMs made it extremely important to diagnose and treat them as early as possible, as almost 90% of our clinically manifested patients had treatable disorders. Thus the attempt to prevent disease progression and complications and to provide diagnosed children with a tolerable standard of living is only possible with the application of a nationwide screening programme detecting metabolic defects in the first few days of life, with prompt treatment and care. The benefits of such a programme would include societal, ethical, and economic aspects, as the current health expenditures on handicapped children and adults in Egypt are enormous. Although most nations had much lower birth prevalence of metabolic disorders than that of Egypt, the technology has been cost-effective for NBS in many developed countries,8,28,29 and recently it was also confirmed as cost-effective in Lebanon, a developing country with similar consanguinity rates to Egypt. 13
Egyptian health policy makers must consider MS/MS technology for the IEM screening in Egypt, at least for the most common disorders as elucidated in our study. We believe that this is the right step in the right moment.
Footnotes
Acknowledgments
The authors thank the patients and their families and Dr Mohamed S Rashed and Dr Mohamed Abdel-Hamid for their kind advice and technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through a European Union funded project: Program for prevention, early detection and early intervention in Egyptian children with genetic disabilities and children at risk (EuropeAid/122327/D/G/EG).