
Abstract
Objectives
To assess time trends in colorectal cancer screening uptake, time-to-colonoscopy completion following a positive fecal occult blood test and associated patient factors, and the extent and predictors of longitudinal screening adherence in Israel.
Setting
Nation-wide population-based study using data collected from four health maintenance organizations for the Quality Indicators in Community Healthcare Program.
Methods
Screening uptake for the eligible population (aged 50–74) was recorded 2003–2018 using aggregate data. For a subcohort (2008–2012, N = 1,342,617), time-to-colonoscopy following a positive fecal occult blood test and longitudinal adherence to screening guidelines were measured using individual-level data, and associated factors assessed in multivariate models.
Results
The annual proportion screened rose for both sexes from 11 to 65%, increasing five-fold for age group 60–74 and >six-fold for 50–59 year olds, respectively. From 2008 to 2012, 67,314 adults had a positive fecal occult blood test, of whom 71% eventually performed a colonoscopy after a median interval of 122 (95% confidence interval 110.2–113.7) days. Factors associated with time-to-colonoscopy included age, socioeconomic status, and comorbidities. Only 25.5% of the population demonstrated full longitudinal screening adherence, mainly attributable to colonoscopy in the past 10 years rather than annual fecal occult blood test performance (83% versus 17%, respectively). Smoking, diabetes, lower socioeconomic status, cardiovascular disease, and hypertension were associated with decreased adherence. Performance of other cancer screening tests and frequent primary care visits were strongly associated with adherence.
Conclusions
Despite substantial improvement in colorectal cancer screening uptake on a population level, individual-level data uncovered gaps in colonoscopy completion after a positive fecal occult blood test and in longitudinal adherence to screening, which should be addressed using focused interventions.
Introduction
Colorectal cancer (CRC) is the second most commonly diagnosed malignancy in Israel. 1 The stepwise and gradual development of colorectal tumors 2 enables early detection through various modalities, including annual or biannual fecal occult blood tests (FOBTs), sigmoidoscopy, colonoscopy, and computerized-tomography colonography. 3 Screen-detected cancers are generally of lower stage and are associated with improved survival compared to interval cancers and those in the unscreened population. 4 The lack of clear advantage of a particular modality 5 has led to a variety of options being included in national screening programs.6,7
Stool-based fecal occult blood testing using guaiac-based or immunochemical tests (FIT) is feasible on a population level and is associated with decreases in both mortality and incidence of CRC. 8 However, the effectiveness of this method relies on longitudinal adherence to screening every 1–2 years to diminish the risk of interval cancer. 9 In contrast, colonoscopy requires repetition only every 10 years if normal 10 ; abnormal findings can be directly addressed (via biopsy and polypectomy) at the time of the screening procedure. Factors related to longitudinal adherence to CRC screening include both personal characteristics and health system features.11–14
Timely visualization of the colon after a positive FOBT is required in order to definitively rule in or out colonic tumors.7,15 Current guidelines recommend that colonoscopy be completed following a positive FOBT within a limited timeframe, ranging from 30 days in Australia 16 to 60 days in Canada. 17 Waiting time guidelines are based mainly on expert opinion or consensus statements of professional organizations, since the optimal timing of colonoscopy after positive FOBT has not yet been established by clinical trials. Furthermore, observational studies indicate that waits of up to 6 18 or even 10 months 19 are not associated with adverse outcomes. Numerous factors may affect the performance and timing of colonoscopy following positive FOBT including those related to the patient, 20 the physician/provider, 21 and the healthcare system (including infrastructure and accessibility). 22
Israel’s National Health Insurance Law stipulates that preventive and curative healthcare for the entire civilian population be delivered by one of four health maintenance organizations (HMOs), all of which are non-profit and publicly administered and funded. 23 Adult citizens are free to choose whichever HMO they wish to join and switching membership to another fund, though relatively simple, rarely occurs. Electronic medical records (EMRs) are in universal use for primary care in the four HMOs.
Israel’s Health Ministry guidelines recommend yearly FOBT screening for individuals aged 50–74 at standard risk of CRC. 24 The screening program is administered by the HMOs. Individuals in the target age group receive yearly invitations and kits, and screening uptake is monitored annually by the National Quality Indicators Program in Community Healthcare (QICH). 25 The HMOs have gradually transitioned from guaiac-based to FIT, and screening is considered adequate if a FOBT was performed in the measurement year or if colonoscopy, for any indication, was performed within the last 10 years. Each HMO provides the QICH directorate with aggregate data, derived from individual members’ EMRs. QICH reports uptake of CRC screening, and other indicators, on a national level annually. 26
The purpose of this study was to perform a comprehensive review of CRC screening in Israel at the national level. To this end, we assessed the time trends in screening uptake using annual aggregate data (Aim 1). Furthermore, using individual-level data, we examined the timing and patient factors associated with colonoscopy completion following a positive FOBT (Aim 2), and as well as the extent and factors associated with longitudinal adherence to screening guidelines (Aim 3).
Methods
We describe the outcome, study population, data source, and statistical analysis for each Aim separately.
Aim 1—Time trends for CRC screening uptake on a national level 2003–2018
The outcome in this analysis was the annual proportion of individuals in the target age group 50–74 years who performed FOBT in the measurement year or colonoscopy within the previous 10 years. Annual data based on individual members’ EMR were provided by the four Israeli HMOs in aggregated five-year age and sex groups. Denominators included all members of the HMOs in the target age group, essentially comprising the entire permanent population of Israel, since military personnel (who may receive health services via the Department of Defense) are generally discharged by age 50 years. Results were stratified according to two age groups (50–59 and 60–74 years) and displayed graphically.
Aim 2—Measuring time-to-performance and patient factors associated with colonoscopy completion following a positive FOBT
The outcomes assessed were any performance of a follow-up colonoscopy, time-to-performance, and median time-to-performance of colonoscopy following a positive FOBT. The study population for this Aim was a subcohort of that described in Aim 1, comprising individuals insured by the four HMOs, aged 50–74, with a positive FOBT (regardless of kit type used) during the years 2008–2012. Patients with a diagnosis of CRC prior to FOBT were excluded. We also excluded those who had performed a colonoscopy in the two years prior to the positive FOBT, since the cause of positive FOBT may have already been determined and physicians may have decided that early repeat colonoscopy was unnecessary.
The analysis of time-to-colonoscopy was performed using anonymized individual-level data from EMRs from the four HMOs, which were pooled into a single dataset. We visualized time-to-performance using Kaplan–Meier plots and then assessed the independent contribution of patient-related covariates on time-to-performance of colonoscopy using Cox proportional hazards models, or completion. Follow-up time was counted from date of positive FOBT result (last entry 30 September 2012, to allow at least 90 days of follow-up) to date of performance of colonoscopy, date of death, last membership date in an HMO, or end of follow-up (31 December 2012). The proportionality assumption was verified by inspecting log-minus log plots.
Covariates were chosen for multivariable analysis based on their importance in the literature (e.g. age, 20 sex, 27 socioeconomic position 28 ) or based on their association (P < 0.05) on univariate analysis with any completion and or time-to-completion (by Chi square and log rank test, respectively). Variables selected for entry in the multivariate models included demographic characteristics (age, sex, and exemption from co-payments—a proxy for low socioeconomic status (SES)), health behaviors (smoking, other cancer screening tests performed (PSA or at least two mammograms in the study period)), comorbidity (diabetes, hypertension, cardiovascular disease (determined by previous documented percutaneous or surgical vascular procedures), anemia (<14 g/dl for men and <12 g/dl for women)), and body mass index (BMI). All covariates were binary (yes/no) except age (assessed in categories of 50–54, 55–59, 60–64, 65–69, and 70–74 years) and BMI which was examined in categories of <18.5, 18.5–24.9 (reference), 25–29.9, 30–34.9, 35–39.9, and ≥40 kg/m2.
Aim 3—Assessing the extent of and predictors associated with longitudinal adherence to CRC screening
For this aim we used a historical prospective design. The outcomes assessed were any adherence to CRC screening and longitudinal adherence, which was categorized according to four levels: “Non-adherence” was defined as non-performance of any FOBT during 2008–2012 or any colonoscopy since 2003. “Full adherence” was defined as performing a colonoscopy at least once since 2003 or yearly FOBT from 2008 to 2012, “incomplete adherence” was defined as performing 3–4 FOBT tests in the years 2008–2012, and “partial” (inconsistent) adherence was defined as performing only 1–2 FOBT tests in the sub-study years.
For this Aim, the data source was individual-level data collected from the EMRs of the four HMOs and pooled into a single dataset. For individuals in this subcohort, in addition to data on annual FOBT between 2008 and 2012 we obtained information on whether a colonoscopy had been performed since 2003.
The study population included individuals in the target age group 50–70 in 2008 who could potentially be followed up for a full five years until 2012. Thus, individuals aged >70 were excluded from the assessment of longitudinal adherence, as well as those whose duration of membership in a particular health fund was less than one year.
After pooling data from all four HMOs, we assessed the factors associated with any adherence using logistic regression models and with degrees of adherence using multinomial logistic regression. The covariates assessed included demographic variables, health behaviors, and comorbidities (except anemia) as above in Aim 2, as well as average frequency of primary care visits (>8 versus ≤8) over the study period. Variables entered into the models were chosen based on their association with adherence on bivariate analysis (P < 0.05, using chi square tests) or from the literature. In these models, all covariates were binary: BMI was dichotomized as obese/non-obese (>30 kg/m2 versus ≤30 kg/m2) as was age (50–59 years versus 60–70 years).
Statistical significance was determined using P-values (cutoff <0.05) and 95% confidence intervals (CIs). Analyses were performed using IBM-SPSS Statistics for Windows, Version 22.0 (Armonk, NY).
Ethical issues: Data on screening uptake by five-year age groups, exemption from co-payments, and sex are transferred in aggregate fashion annually to the QICH directorate. Additionally, for the purposes of this study, approval was granted by the institutional review boards (Helsinki Committee) of Hadassah University Hospital and the individual HMOs to obtain and analyze anonymized individual-level data for a full five-year period (2008–2012) for a pooled analysis of Aims 2 and 3. There was a waiver for individual informed consent, since the study used existing, de-identified data.
Results
Aim 1
Annual denominators ranged from 1,146,875 to 1,585,895, reflecting population growth. At the initiation of the QICH program in 2003, only 11.5% of Israeli adults (N = 132,019) in the appropriate age group performed FOBT in the previous year or underwent colonoscopy screening. By 2018, this proportion increased to 64.7% (N = 1,026,579) and was similar for men and women. Overall, individuals in the 50–59-year age group showed a 618% rise in proportion screened while those aged 60–74 experienced a 500% rise (Figure 1).
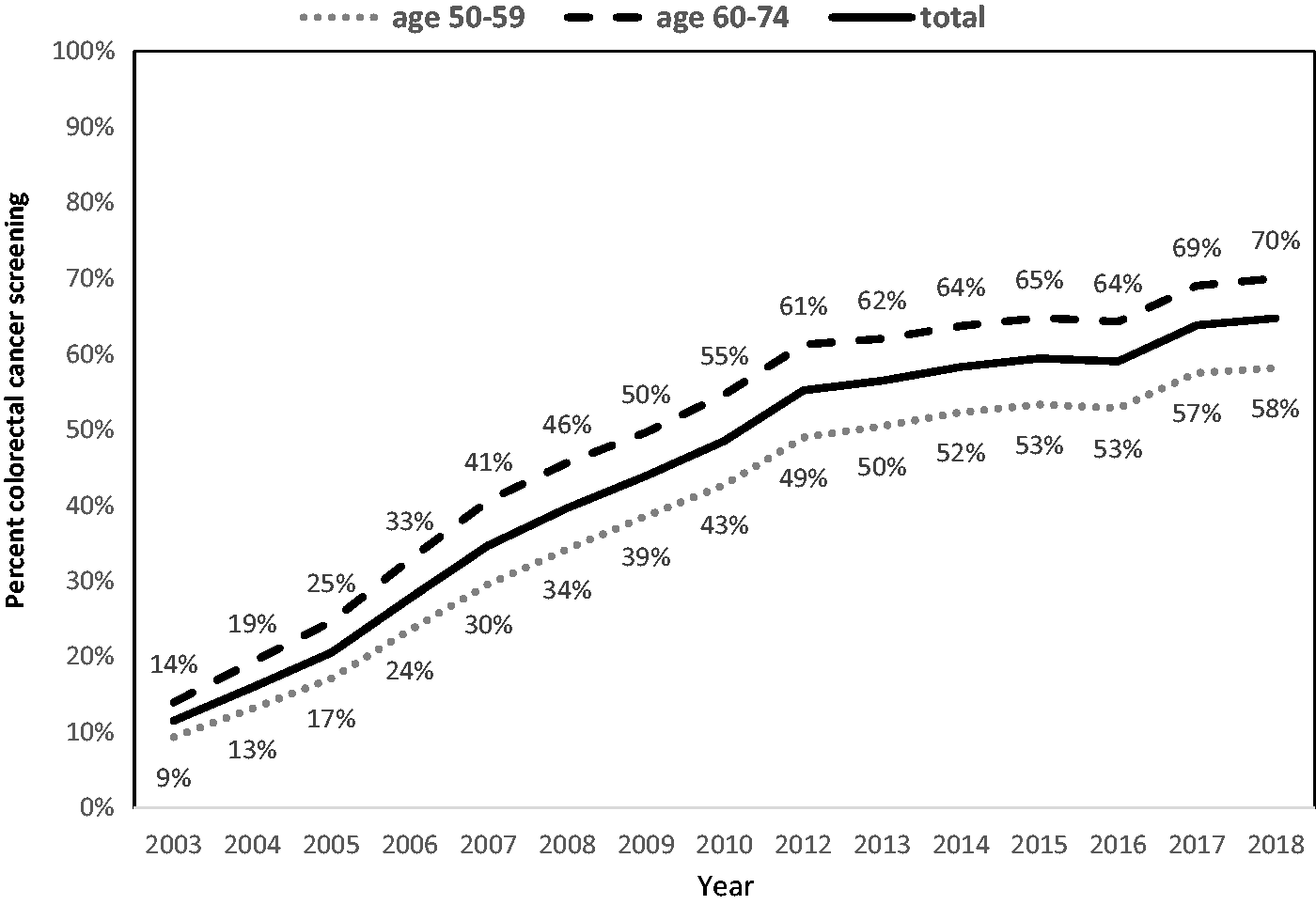
Annual percentage of adults aged 50–74 undergoing adequate screening for CRC in Israel, 2003–2018, overall and by age group.Note: Performed FOBT in the measurement year or colonoscopy within the previous 10 years.
Aim 2
Baseline characteristics for the subcohort forming the basis of the analysis of Aim 2 and 3 are shown in Table 1. As shown in Figure 2(a), 67,314 (5%) members of the four Israeli HMOs aged 50–74 on 1 January 2008 had a positive FOBT at least once in the follow-up period. As shown in Table 2, gender was roughly balanced among individuals with a positive FOBT, the age distribution was just over 20% in each five-year age category for ages 50–69 years, but only 11.3% of this sub-population was aged 70+. As opposed to the general population of this age group (Table 1), in which approximately 21% received exemption from co-payments, the group with positive FOBT included 29.2% with low SES.
Baseline characteristics of 1,317,647 Israeli adults aged 50–74 in 2008 without prior colorectal cancer and with membership in a health maintenance organization of at least one year.
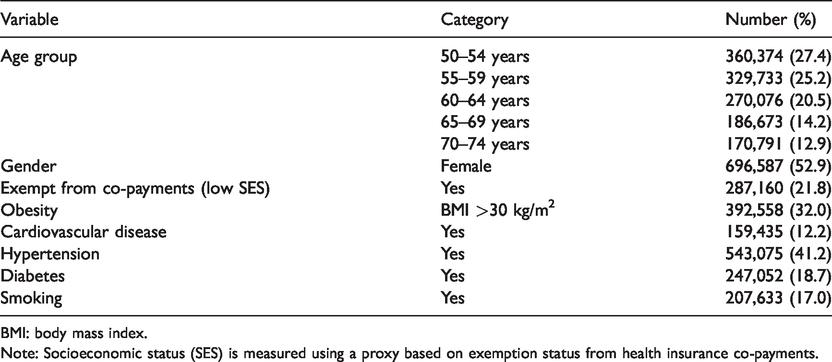
BMI: body mass index.
Note: Socioeconomic status (SES) is measured using a proxy based on exemption status from health insurance co-payments.
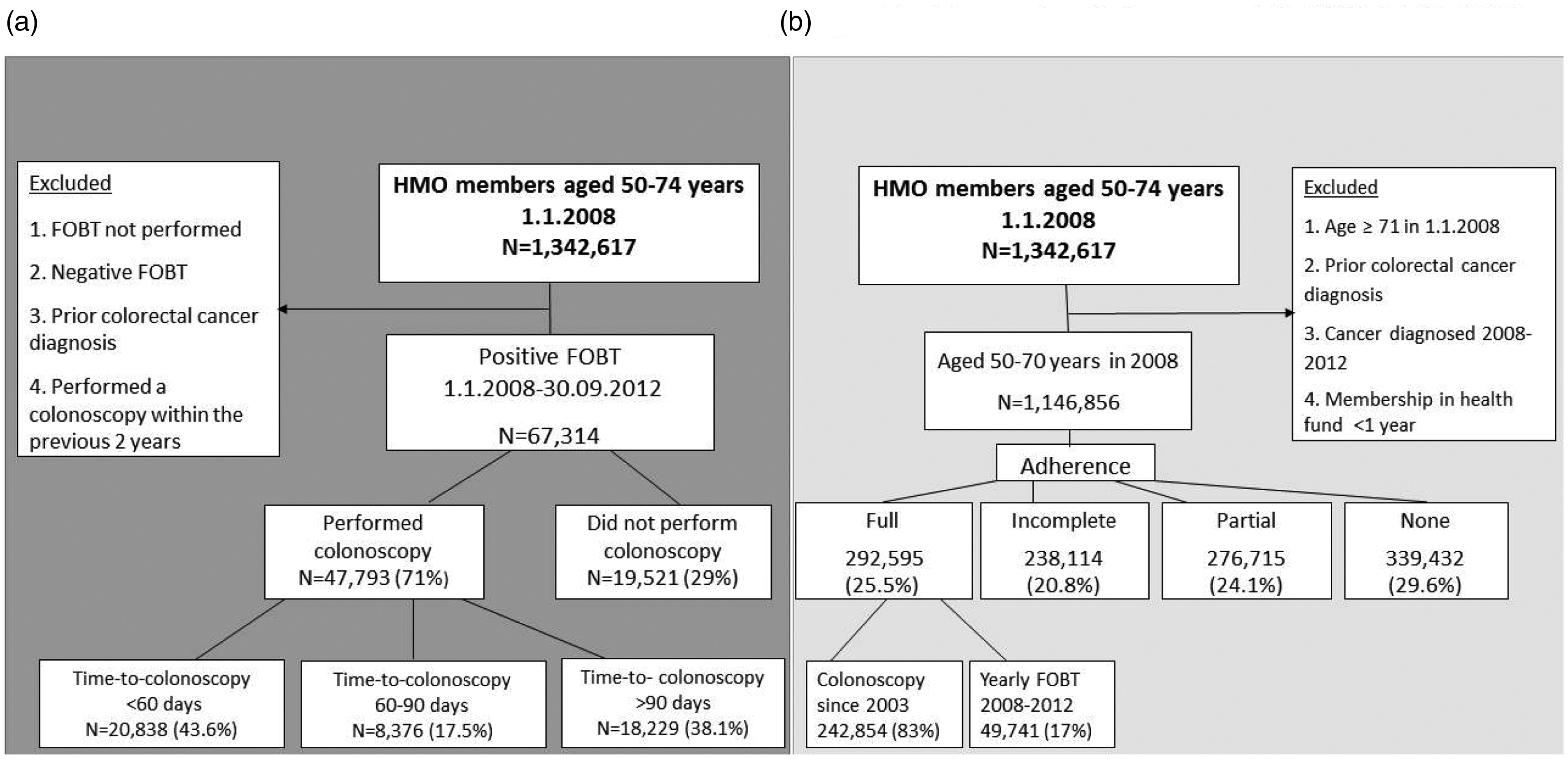
Flow diagrams showing the sub-study populations and outcomes for (a) Aim 2: colonoscopy completion following positive FOBT and (b) Aim 3: longitudinal screening adherence 1 January 2008–31 December 2012.
Multivariate Cox proportional hazards models showing association of covariates on time from positive FOBT results to colonoscopy, Israel 2008–2012 (N = 67,314 a ).
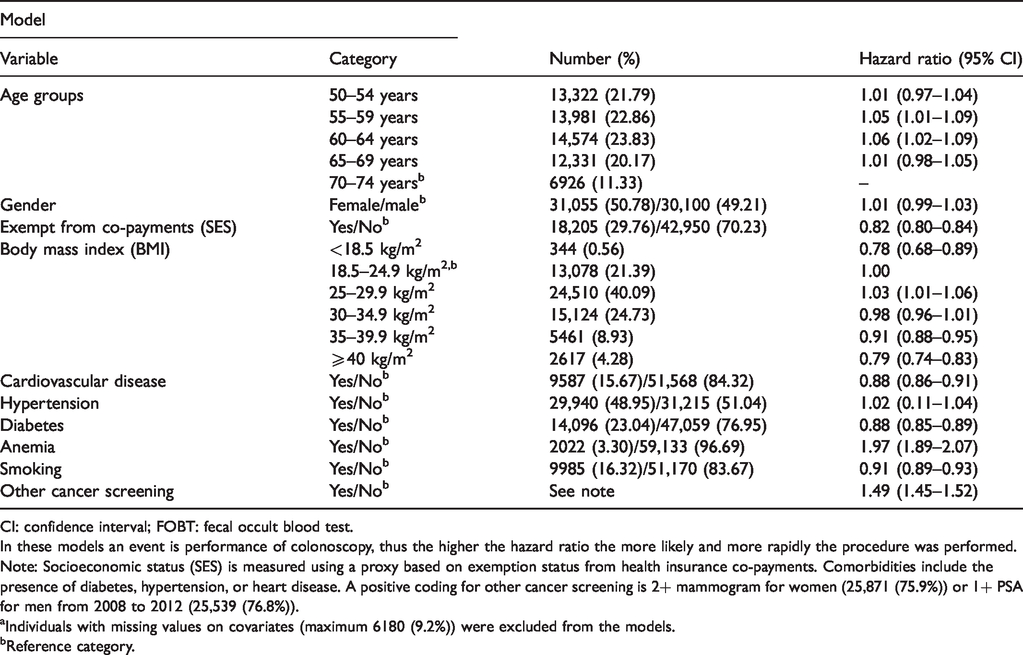
CI: confidence interval; FOBT: fecal occult blood test.
In these models an event is performance of colonoscopy, thus the higher the hazard ratio the more likely and more rapidly the procedure was performed.
Note: Socioeconomic status (SES) is measured using a proxy based on exemption status from health insurance co-payments. Comorbidities include the presence of diabetes, hypertension, or heart disease. A positive coding for other cancer screening is 2+ mammogram for women (25,871 (75.9%)) or 1+ PSA for men from 2008 to 2012 (25,539 (76.8%)).
aIndividuals with missing values on covariates (maximum 6180 (9.2%)) were excluded from the models.
bReference category.
While 47,793 (71%) eventually performed a colonoscopy following a positive FOBT, only 20,838 (31% of the total with positive FOBTs and 43.6% of those performing any follow-up colonoscopy) completed the examination within 60 days, with a median time for completion of 112 days (95% CI 110.2–113.7) (Figure 1 supplemental).
Cox models were performed in order to assess independent effects of covariates on the time-to-colonoscopy following a positive FOBT. Note that since the event is performance of colonoscopy, a higher hazard ratio (HR) denotes a shorter time-to-performance (Table 2). We examined the effects of age, gender, and SES as well as comorbidities (cardiovascular disease, hypertension, diabetes, and anemia), smoking, and BMI and other screening behaviors (mammogram for women/PSA for men). Factors associated with time-to-colonoscopy included age (Wald-21.84, 4 degrees of freedom, P < 0.0001), smoking, BMI (Wald = 141.65, 5 degrees of freedom, P < 0.0001), comorbidities, but not gender. Both underweight and obesity were associated with significantly prolonged wait times, as was low SES, diabetes, and smoking. Factors associated with shorter time-to-colonoscopy following a positive FOBT included age 55–64 years, performance of other screening tests during the study period (HR 1.49, 95% CI 1.45–1.52), and presence of anemia, HR= 1.97 (95% CI: 1.89–2.07). Similar factors were shown to be associated with performing colonoscopy within 60 or 90 days (not shown).
Aim 3
There were 1,146,856 people insured in the Israeli HMOs in 2008 aged 50–70, the age group for whom the relevant CRC screening guidelines apply and for whom adherence could potentially be assessed for a full five years. Their baseline characteristics are shown in Table 3. Of these, 29.6% did not perform any screening tests (non-adherence), 24.1% followed the guidelines for only one or two out of the five consecutive years of follow-up (inconsistent adherence), 20.8% followed the relevant guidelines three or four years out of the five (incomplete adherence), and only 25.5% fully complied. Of those defined as fully adherent, 83% were individuals who had performed colonoscopy during the preceding 10 years, and only 17% consistently performed annual FOBT, comprising a mere 4.3% of the entire population (Figure 2(b)).
Multinomial logistic regression of factors associated with full, incomplete, and partial (inconsistent) adherence to CRC screening compared to total non-adherence over five years in the Israeli population aged 50–70 in 2008 (N = 1,146,856).
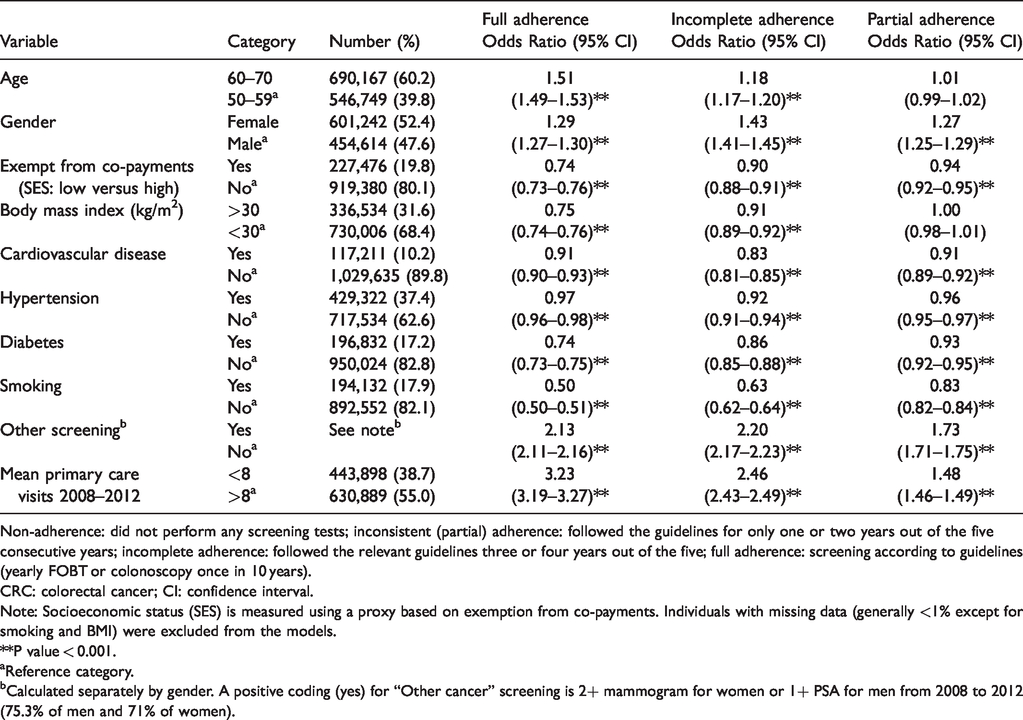
Non-adherence: did not perform any screening tests; inconsistent (partial) adherence: followed the guidelines for only one or two years out of the five consecutive years; incomplete adherence: followed the relevant guidelines three or four years out of the five; full adherence: screening according to guidelines (yearly FOBT or colonoscopy once in 10 years).
CRC: colorectal cancer; CI: confidence interval.
Note: Socioeconomic status (SES) is measured using a proxy based on exemption from co-payments. Individuals with missing data (generally <1% except for smoking and BMI) were excluded from the models.
**P value < 0.001.
aReference category.
bCalculated separately by gender. A positive coding (yes) for “Other cancer” screening is 2+ mammogram for women or 1+ PSA for men from 2008 to 2012 (75.3% of men and 71% of women).
Smoking, comorbidities, low SES, and obesity were inversely associated with performance of CRC screening, while performing other screening tests, frequent visits to the family doctor, age 60–70 compared to 50–59 years, and female sex were positively associated with any performance of screening tests (Supplemental Table 1).
We performed a multinomial logistic regression assessing the factors associated with different levels of adherence, with non-adherence as the reference (Table 3). This model demonstrates that older age (60–70 years versus 50–59 years) was associated with adherence (OR 1.18 for partial and OR 1.51 for full adherence). Smoking, diabetes, low SES, cardiovascular disease, and hypertension were inversely associated with adherence. For instance, smokers were only about half as likely to be fully adherent as nonsmokers (OR 0.5, 95% CI 0.50–0.51). Factors which were strongly associated with adherence included health behaviors such as performing other screening tests (OR 2.13, 95% CI: 2.11–2.16) and a high average frequency of visits to the family doctor during the follow-up period (OR 3.23 95% CI: 3.19–3.27 for full adherence, with statistically significant but somewhat weaker associations for incomplete and partial adherence).
Discussion
In this large study encompassing the entire Israeli population, we observed a substantial rise of at least 500% in screening uptake for CRC over a 15-year period. This increase was seen in men and women, both younger and older. Unlike data from many countries, the data were based on EMRs from the entire population with universal health coverage, and are not estimates based on samples or surveys. Increased access to screening programs has been observed globally, 7 although the pace of improvement has varied by country and by screening modality. Improved screening rates in Israel are reflected in a decreased proportion of CRCs diagnosed at advanced stages, indicating an overall success of the screening program at the population level. 1 Incidence and mortality from CRC has also fallen as it has in most high-income countries.1,29
Notwithstanding this observed success, our findings indicate that cross-sectional aggregate data, even if collected and tabulated on a yearly basis, may obscure gaps in the long-term screening habits of the populace, and may over-estimate adherence. 14 The latter can only be discerned using individual-level data with adequate follow-up. The current analysis shows that despite improvements in uptake of screening at the population level, individual longitudinal adherence to repetitive annual FOB testing is very rare, with most “full” adherence attributable to performance of colonoscopy every 10 years. These results are in line with those of others who have assessed repetitive FOBT performance. Gellad et al. 11 found that over five years only 41% of insured individuals were adequately screened (defined as four FOBTs performed out of five) when assessed longitudinally, with no difference between men and women. 11 In a study directly comparable with ours, among continually insured individuals in a US managed care organization, although 64% were assessed as “adequately screened,” this assessment in almost all cases (99.6%) was attributed to performing colonoscopy once per decade, whereas only 0.3% of individuals were adherent to yearly FOBT testing over 10 years. 12 Our study reinforces this finding and underscores the difficulty of maintaining adherence to yearly FOBT on a long-term basis.
Enhancing the regularity of screening performance has the potential to further reduce morbidity and death from CRC. We found, as did Benito et al. 30 that increased age is associated with a higher odds of consistent adherence. Similarly to Fenton et al. 13 and Nielson et al. 31 we found that performance of other cancer screening tests (whether or not recommended, such as PSA) strongly predicted longitudinal adherence to FOBT. Sanford et al. 32 reported, as we did, that smokers were less likely to be screened for CRC. Targeting smokers, women who have not had recommended mammography and younger age groups for interventions to augment screening adherence may be worthwhile.
The screening cycle cannot be considered complete unless definitive tests are performed following a positive FOBT result. In the Israeli population, almost one-third of such results were not unacceptably long followed up by colonoscopy. Of the ones that were followed up, the time to definitive testing was in many cases. Recent data from a single Israeli HMO showed a similar proportion without follow-up colonoscopies following positive FOBTs; the authors reported that wait times of 12+ months were associated with overall CRC risks, with intervals of 10+ months specifically associated with right-sided lesions. 33
Predictors of timely colonoscopy performance following a positive FOBT included: younger age, higher SES, performance of other screening tests, and absence of comorbidities. Our study was not able to assess delays in referral or health system factors such as availability of facilities and human resources required to improve compliance and reduce waiting times. Age, gender, absence of health insurance, physician decisions, non-white ethnicity, rurality, geographic factors, socioeconomic deprivation of the area of residence, and greater distance to regional capital have been shown to be associated with colonoscopy uptake after a positive FOBT.27,28,34,35 The QICH has recently introduced a quality indicator for performing colonoscopy after positive FOBT within 180 days and this has the potential to improve the completion of the diagnostic cycle for those with positive screening tests.
Although patient-related factors, including sociodemographic characteristics and comorbidities, showed a statistically significant association with adherence to screening, other factors remain unmeasured. We were unable to assess personality and motivational characteristics. A smaller study of members of a single Israeli HMO showed no association with the “Patient Activation Measure” which assesses knowledge, skills, beliefs, and confidence in managing health. 36 Regarding system-related factors, there is evidence that systemic interventions can have moderate effects on improving uptake and adherence to FOBT testing, and can lead to increased performance of follow-up colonoscopy. 37 Furthermore, patient-level interventions which have been found to be successful in reducing waiting times after FOBT include cellphone reminders 36 and patient navigators, while reporting performance or sending reminders are effective provider-level interventions. 38
Our finding, noted by others, that increased contact with the healthcare system, as measured by the frequency of physician visits,22,39 was related to longitudinal adherence to screening reinforces the role of health professionals in enhancing screening uptake and consistency.
Our study strengths include data for the entire population based on EMRs, without sampling or surveys. We assessed aggregated cross-sectional data which enabled the assessment of screening uptake in the national CRC screening program by gender and in broad age categories for 13 years of follow-up. In addition, we had access to an enriched dataset comprising five of these years which included longitudinal individual data on screening adherence, sociodemographic factors, health behaviors, and comorbidities. Our study is one of the largest examining longitudinal adherence and factors related to colonoscopy completion. On the other hand, we had limited data on SES, and no data on patient motivational factors and physician or clinic-based maneuvers to enhance adherence. Furthermore, we could not assess whether the screened population was at average or high risk, as information on family history or previous detection of high-risk polyps was absent from our dataset. It is possible that full adherence was slightly underestimated, as some members of the subcohort studied for Aim 2 may have had colonoscopies prior to 2003, years for which we did not have data on colonoscopy, but this is unlikely to change the overall pattern of adherence.
In conclusion, further efforts are required in order to increase longitudinal adherence to CRC screening, as well as to improve colonoscopy completion rates and decrease the timeframe for completion of work-up following a positive FOBT. Economic evaluation of screening modalities must take into account real-world data regarding actual long-term repetitive adherence, and may favor colonoscopy, given current evidence and the observed rarity of adequate longitudinal adherence to FOBT. This and the morbidity associated with delayed colonoscopy argue for enhancing colonoscopy infrastructure and access in national programs. Alternatively, biannual FIT, which is well-accepted 30 and also considered cost-effective, 40 augmented with active reminders, advice and navigation could be a feasible recommendation to ensure improved longitudinal coverage of the entire population. Future research and interventions will need to address system barriers to effective and consistent CRC screening on a population level in order to further reduce CRC morbidity and mortality.
Supplemental Material
sj-pdf-1-msc-10.1177_0969141320919152 - Supplemental material for Adherence to national guidelines for colorectal cancer screening in Israel: Comprehensive multi-year assessment based on electronic medical records
Supplemental material, sj-pdf-1-msc-10.1177_0969141320919152 for Adherence to national guidelines for colorectal cancer screening in Israel: Comprehensive multi-year assessment based on electronic medical records by Ora Paltiel, Aravah Keidar Tirosh, Orit Paz Stostky, Ronit Calderon-Margalit, Arnon D Cohen, Einat Elran, Liora Valinsky, Eran Matz, Michal Krieger, Arye Ben Yehuda, Dena H Jaffe and Orly Manor in Journal of Medical Screening
Footnotes
Acknowledgements
Aravah Keidar Tirosh and Orit Paz Stotsky performed parts of this work as Master’s Theses in the Hebrew University, Braun School of Public Health and Community Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Israel Cancer Association and National Institute for Health Policy Research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.