
Abstract
Objective
Monitoring breast screening programmes is essential to ensure quality. BreastCheck, the national breast screening programme in the Republic of Ireland, commenced screening in 2000, with full national expansion in 2007, and digital mammography introduced in 2008. We aimed to review the performance of BreastCheck from 1 January 2004 to 31 December 2013.
Methods
Using the customised clinical and administrative database, performance indicator data were collected from BreastCheck and compared with programme and European guideline standards.
Results
Over the decade, 972,236 screening examinations were performed. Uptake initially rose following national expansion, but fell in the subsequent years to <70% in 2012–2013. Following the introduction of digital mammography, initial recall rates increased from 5.2% in 2004–2005 to 8.1% in 2012–2013. Subsequent recall rates remained within the target of <3%. On average, invasive cancer detection rates were 6.6/1000 for initial and 4.5/1000 for subsequent women. Small cancer detection rates were for <15 mm 43.4% (initial women) and 51.7% (subsequent) and for ≤10 mm 24.0% (initial) and 29.5% (subsequent). Ductal carcinoma in situ detection as a percentage of all cancers averaged 21.2% for initial and 20.0% for subsequent women. The majority were intermediate or high-grade ductal carcinoma in situ. The positive predictive value was 11.9% for initial and 21.8% for subsequent women. Standardized detection ratios remained above the programme target.
Conclusion
Revised indicators to reflect the digital mammography era are anticipated in revised European Guidelines on breast cancer screening.
Introduction
Mammography is claimed to reduce mortality from breast cancer, with such reductions primarily being attributed to national screening programmes.1–4 There have been notable improvements in mammographic screening and treatment over recent decades. 1 Despite these improvements, the benefits of breast cancer screening programmes have been questioned,5–7 reinforcing the importance of monitoring and assessing programme performance indicators against international standards. 8
BreastCheck, the national breast screening programme in the Republic of Ireland, provides free mammograms to women biennially. Introduced in 2000 in the eastern half of the country and expanded nationally from 2007 onwards, BreastCheck carries out screening at four screening units located in major university teaching hospital campuses and in 17 mobile units. Eligible women aged 50–64 are invited for screening by letter with an appointment. Women can reschedule this appointment by contacting the programme. A reminder invitation is sent. Following screening, women with a positive mammogram are recalled for further assessment in one of the four screening units. The performance of BreastCheck has been continually monitored and evaluated against programme and European guidelines, with updates on key performance indicators published annually. 9 Digital mammography was introduced in 2007 and has been fully employed throughout the programme since April 2008. Phased re-equipping of the two existing screening centres began in 2007 and was completed by mid-2008 (over a period of approximately 18 months). The two new screening centres in the West and South of the country were digitally equipped in advance of extension of screening beginning in January 2008. From 2000 to 2015, eligible women aged 50–64 were invited for screening.
In late 2015, age extension of the programme commenced, with the upper screening age being extended from age 65 to 69 on a phased basis. This age extension is in fulfilment of a Programme for Government commitment and aligns with European breast cancer screening guidelines. 10 By the end of 2021, all eligible women aged 50–69 will be invited for free routine mammograms. In light of these developments, it is an opportune time to examine the performance of BreastCheck over the 10 years prior to European Reference Organisation for Quality Assured Breast Screening and Diagnostic Services (EUREF) accreditation (awarded 2015) and the commencement of age extension.
This research aims to present a two-year interval analysis of key performance measures from BreastCheck over the decade 1 January 2004 to 31 December 2013, during which time it underwent national expansion and introduced digital mammography.
Methods
This study uses the BreastCheck administrative and clinical database to present a two-year interval analysis of performance measures. This database includes data from the invitation stage, through screening, and up to primary surgical treatment, where relevant. Performance indicators are compared with programme standards and targets presented by BreastCheck 11 in ‘Guidelines for Quality Assurance in Mammography Screening’ (3rd edition) and the European guideline standards and targets in ‘European Guidelines for Quality Assurance in Mammography Screening’ (4th edition). 10 The BreastCheck guidelines followed the European guidelines exactly, except where country-specific incidence rates were used to calculate rates, and for the benign biopsy rate, which does not have a corresponding European standard. Therefore, the expected cancer detection rates and benign biopsy rates were specific to the BreastCheck guidelines. The eligible women uptake rate includes all women of screening age known to the programme, except those excluded or suspended by the programme for reasons including opting out from interaction with the programme, women with a prior recent mammogram, or in follow-up care for breast cancer. Performance measures presented include number of women screened, uptake rates, recall rates, cancer detection rates (type and size), proportion of ductal carcinoma in situ (DCIS) and benign open biopsy rates. Positive predictive values (PPVs) and standardized detection ratios (SDRs) are also included as overall indicators of programme performance. Uptake of screening is essential for programmes to achieved desired mortality reductions. The aim of screening is to detect small cancers <15 mm with the best prognosis. The SDR is a composite measure used to reflect overall programme performance and is useful for comparative purposes with other national programmes. Data are presented for women attending for first screening and subsequent screening. Subsequent screening refers to a woman’s second or later screening event with BreastCheck.
Results
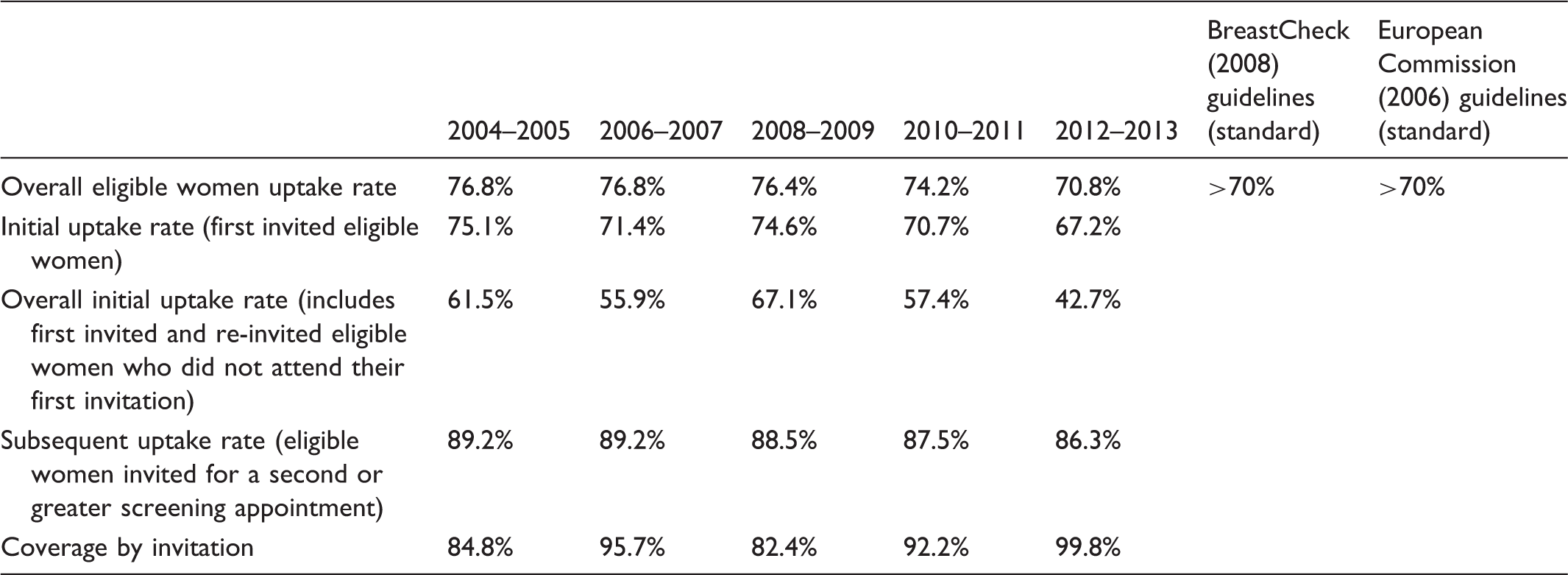
Uptake and coverage rates for BreastCheck (two-year period analysis).
Performance indicators and characteristics of cancers in first screened women (two-year period analysis).
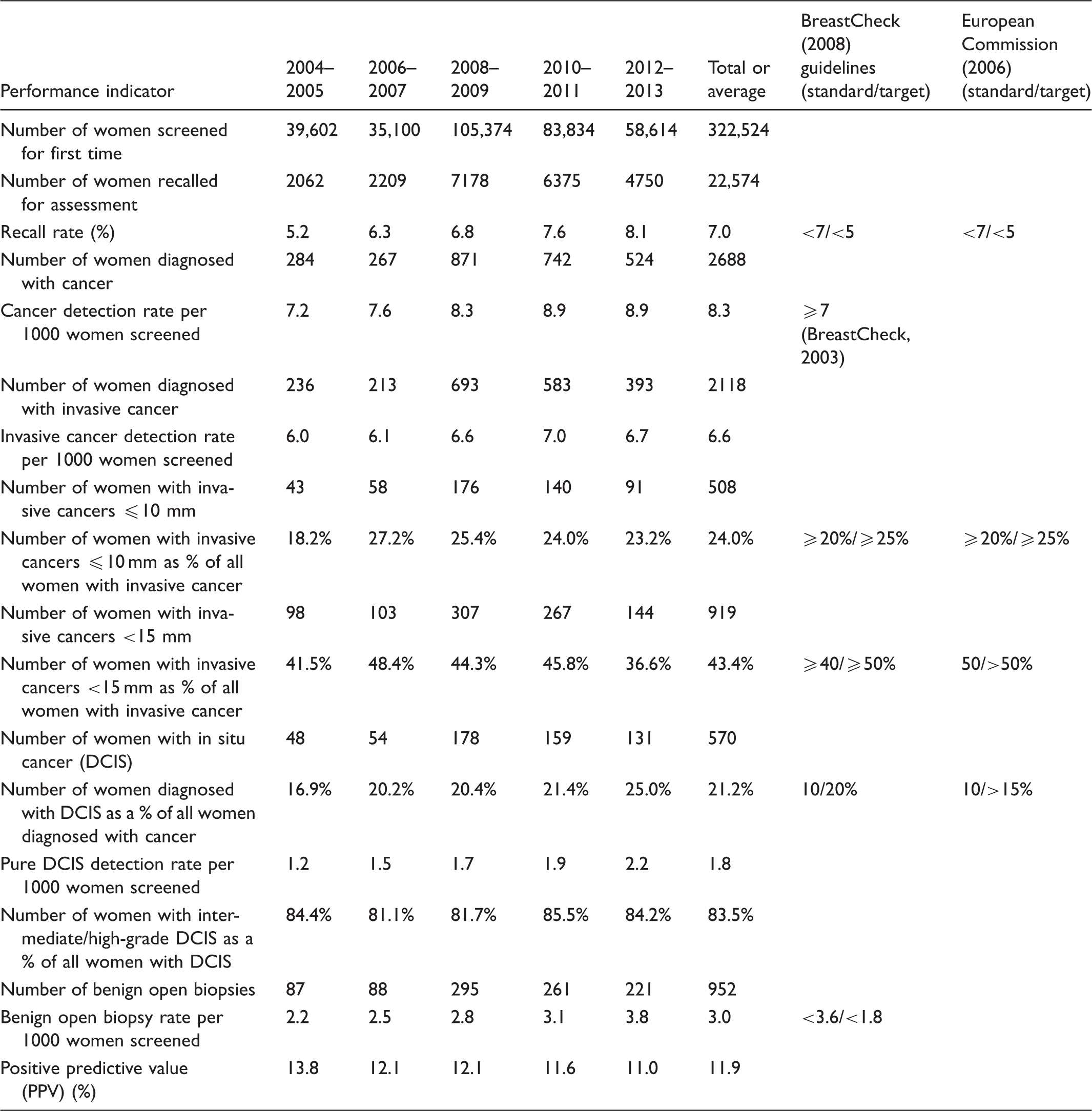
DCIS: ductal carcinoma in situ.
Performance indicators and characteristics of cancers in subsequent screened women (two-year period analysis).
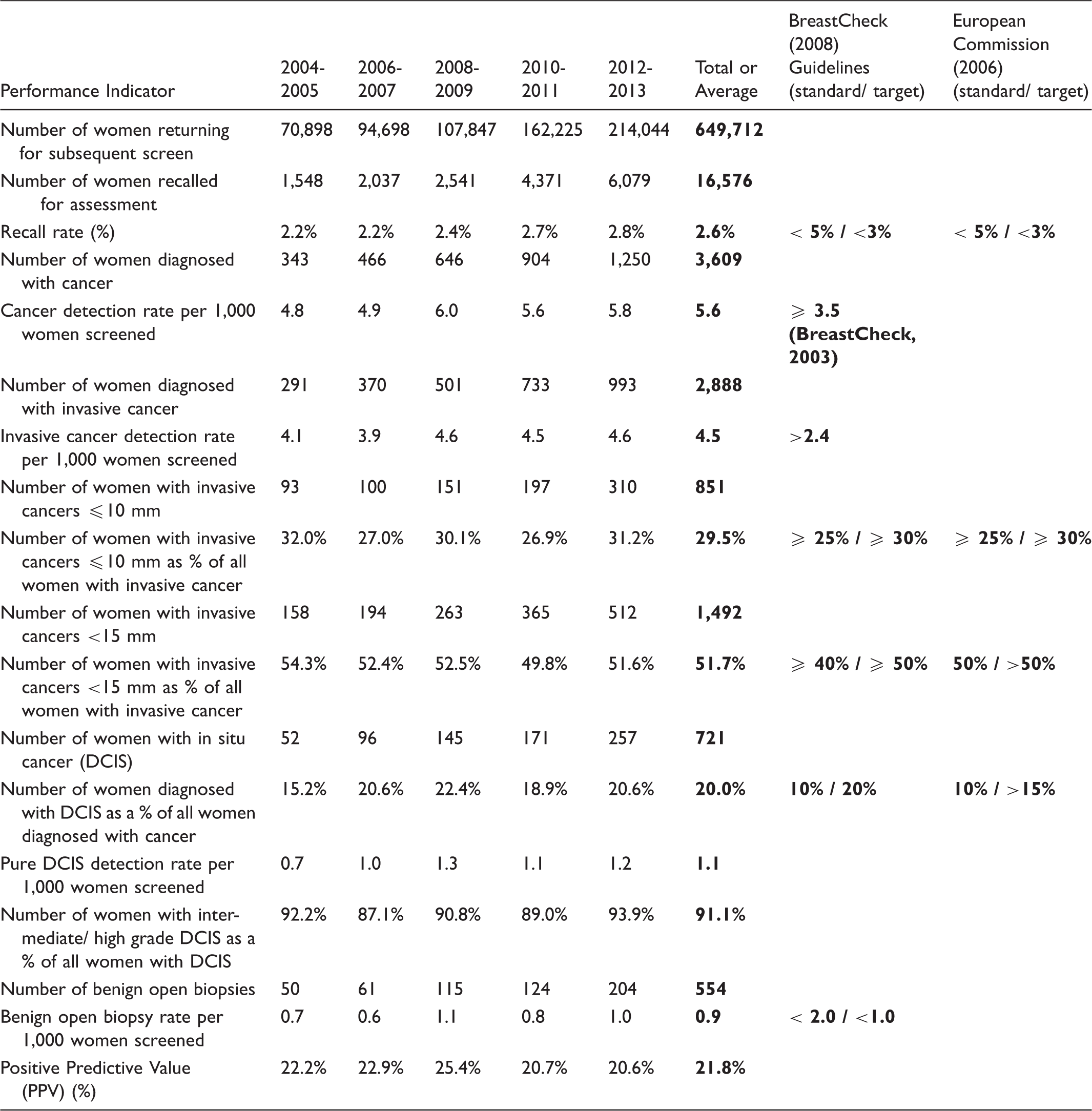
Initial recall rates rose following the introduction of digital mammography, from 5.2% in 2004–2005 to 8.1% in 2012–2013. Recall rates for first screened women remained outside the BreastCheck and European target of <5% across the 10-year period and outside the standard of <7% in 2010–2011 and 2012–2013 (Table 2). Conversely, subsequent recall rates met the BreastCheck and European target (<3%) and ranged from 2.2% in 2004–2005 to 2.8% in 2012–2013 (Table 3).
There were 2688 initial and 3609 subsequent women diagnosed with breast cancer over the decade. For first screened, the cancer detection rate has risen steadily from 7.2 cancers per 1000 in 2004–2005 to 8.9/1000 in 2012–2013 (Table 2). The overall detection rate was 8.3/1000 first screened women, which exceeds the programme standard of ≥7 (Table 2). An overall increasing detection rate is also apparent for subsequent women, rising from 4.8/1000 in 2004–2005 to 5.8/1000 in 2012–2013 (Table 3), above the programme standard of ≥3.5.
At initial screening, 2118 women were diagnosed with invasive cancer over the period, corresponding to an average invasive cancer detection rate of 6.6/1000 women (Table 2). This rose from 6.0/1000 in 2004–2005 to 6.7/1000 in 2012–2013. For subsequent women, 2888 were diagnosed with invasive cancer, equating to an average detection rate of 4.5/1000 which is above the programme standard of >2.4 (Table 3). This increased from 4.1/1000 in 2004–2005 to 4.6/1000 in 2012–2013.
For initial women, on average 24.0 and 43.4% of screen-detected invasive cancers were ≤10 and <15 mm, respectively (Table 2). The average for ≤10 mm cancers meets the European standard of ≥20%, but falls slightly short of the target of ≥25%. The average for <15 mm cancers meets the BreastCheck standard of ≥40%, but does not meet the European target of >50%. This standard was met in every time period except 2012–2013. For subsequently screened women, on average 29.5% screen-detected invasive cancers were ≤10 mm and 51.7% were <15 mm (Table 3). The average for ≤10 mm cancers meets the European standard of ≥25%, but fails to meet the target of ≥30%, while the European target for <15 mm cancers (>50%) was achieved in every period excluding 2010–2011.
DCIS as a proportion of all cancers averaged 21.2% for first screened and 20.0% for subsequently screened women and is therefore in keeping with the European target of >15%, but overall the DCIS proportion was outside the programme target of 10–20%. The DCIS detection rate for initial women increased steadily over the 10 years, from 1.2/1000 women in 2004–2005 to 2.2/1000 in 2012–2013, with a marked rise post introduction of digital mammography (Table 2). Conversely, the DCIS detection rate for subsequent women has varied from 0.7/1000 in 2004–2005 to 1.2/1000 in 2012–2013 and peaked at 1.3/1000 in 2008–2009 (Table 3). For first screened women, on average 83.5% of DCIS detected was of intermediate or high grade, with this percentage remaining above 80% across the time period (Table 2). For subsequent women, 91.1% of DCIS detected was of intermediate or high grade overall, ranging from 87.1% in 2006–2007 to 93.9% in 2012–2013 (Table 3).
For women undergoing initial screening, benign open biopsy rates met the programme standard (<3.6/1000) in every period except 2012–2013 and averaged 3.0/1000 (Table 2). For those subsequently screened, benign open biopsy rates averaged 0.9/1000 and remained within the programme standard (<2.0/1000) and target (<1.0/1000) in every time period except 2008–2009 (Table 3).
The PPV averaged 11.9% for initial women, declining from a peak of 13.8% in 2004–2005 to 11.0% in 2012–2013 and reflecting the higher recall rate particularly post introduction of digital mammography (Table 2). The PPV for subsequent women averaged 21.8%, remaining above 20% across the decade and peaking at 25.4% in 2008–2009 (Table 3).
The programme standardized detection ratio increased from 1.03 in 2004–2005 to 1.25 in 2012–2013 and met the programme standard (>0.75) and target (≥1.0) in every period.
Discussion
Adoption of a longitudinal perspective on screening programmes and examination of their performance indicators over a sustained period is worthwhile.1,2,12 A key challenge faced by population screening programmes internationally is achieving and maintaining high levels of screening over time. While BreastCheck uptake of screening remained above the acceptable standard of 70% throughout the period, it has been falling since 2010. This trend can be attributed to the uptake rates of initial women. More recently, a new national television advertising campaign introduced in 2014, in addition to a text reminder programme for subsequent women and population register clean-up project have resulted in an overall uptake of 76.5% in 2014/2015. 13 Reviewing comparable programmes across Europe, Giordano et al. found that 13 of 26 breast screening programmes included achieved the European Union benchmark of acceptable uptake (>70%), while nine reached the EU desirable level (>75%). 14 It will be essential to ensure sustained levels of uptake in the programme across the extended age group.
Overall recall rates of 7.0% and 2.6% for women undergoing initial and subsequent screening were found. These rates increased following the introduction of digital mammography, which took place on a phased basis during 2007 and early 2008. European comparisons prior to the introduction of full field digital mammography (FFDM) in most countries have shown Ireland to be midway in the ranking of initial recall rates and amongst the lowest in the ranking of subsequent recall rates. 15
Previous studies that explored breast cancer screening programme performance for screen-film mammography (SFM) versus FFDM have been somewhat inconsistent. Several studies have shown higher recall rates post introduction of digital mammography.16–19 Previously published work from this programme by Hambly et al. compared 35,204 BreastCheck mammograms using FFDM with 153,619 mammograms using SFM, from January 2005 to December 2007. 20 At the time of introduction of FFDM into the BreastCheck programme, they found the cancer detection rate to be significantly higher for FFDM (6.3/1000) than SFM (5.2/1000), and this effect was seen at the time for initial and subsequent screening, invasive cancer and DCIS and also across age groups. They also showed higher recall rates with FFDM.
The current study shows that this trend has continued, with increased cancer detection rates following the introduction of FFDM, reflecting the pattern in most studies for FFDM.16,21 However, Chiarelli et al. found a similar detection rate for digital direct radiography and SFM, 19 while Vinnicombe et al. found no evidence of significant differences between FFDM and SFM cancer detection rates after adjusting for age, ethnicity, area of residence and type of referral. 17 Within the current study, while invasive cancer detection rates rose following the introduction of digital mammography, the increase was more evident in DCIS detection. International European comparisons show Ireland to be high in the ranking of DCIS detection. 22 In line with the findings of other studies,23,24 in our study, the majority of DCIS detected (83.5% for initial and 91.1% for subsequent women) was of intermediate or high grade.
Data from the Danish screening programme show that increased cancer detection rates can be associated with increased rates of benign open biopsies. 25 The move to FFDM may have contributed to the increase in benign open biopsy rates seen in initial women, but despite this increase, overall benign open biopsy rates have remained within the BreastCheck programme target for subsequently screened women and within the standard for women undergoing initial screening.
The overall PPV of recall to assessment was 11.9% for initial and 21.8% for subsequent women, with some variability across the decade and a declining trend emerging for initial women. European comparisons of screening programmes show the PPV in Ireland for both initial and subsequent screening to be midway in rankings. 15 Del Turco et al., Hambly et al. and Vinnicombe et al. found no significant difference in PPVs for FFDM versus SFM, despite higher recall rates shown post FFDM.16,17,20
Among the strengths of this study is complete national data from a population screening programme. Data accuracy is a focus of the programme. Detailed clinical and administrative data are available on all patients, with excellent completeness of collected data, which are used for audit routinely. A limitation of using national average is that local differences are not reflected, however, the organization of this national screening programme is divided into four static units, and these units are routinely compared against the standards, with limited differences found.
This paper has presented an overview of the performance of BreastCheck, against European and programme standards, during a time when the programme underwent national expansion, introduced FFDM and was subsequently awarded full EUREF accreditation. Quality indicators for DCIS and recall rates were established in the analogue era of mammography, and we anticipate revised quality indicators in the forthcoming breast cancer screening guidelines to be published over the coming year.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The National Screening Service is part of the Health and Wellbeing Division of the Health Service Executive. It encompasses BreastCheck – The National Breast Screening Programme, CervicalCheck – The National Cervical Screening Programme, BowelScreen – The National Bowel Screening Programme and Diabetic RetinaScreen – The National Diabetic Retinal Screening Programme.