
Abstract
Objective
Colorectal cancer screening programs frequently report problems ensuring adequate follow-up of positive fecal immunochemical tests (FITs). We investigated strategies implemented by ongoing screening programs to improve follow-up for FIT-positive participants, and explored associations between interventions and reported rates of follow-up.
Methods
We submitted an electronic survey to 58 colorectal cancer screening programs or affiliated researchers. Primary outcomes were the proportion of program participants with a positive FIT completing diagnostic colonoscopy, and patient, provider, and system-level interventions used to improve follow-up. We compare mean colonoscopy completion at six months in programs with and without interventions.
Results
Thirty-five programs completed the survey (60% response). The mean proportion of participants with a positive FIT who completed colonoscopy was 79% (standard deviation 16%). Programs used a mean of five interventions to improve follow-up. Programs using patient navigators had an 11% higher rate of colonoscopy completion at six months (p = 0.05). Programs sending reminders to primary care providers when no colonoscopy has been completed had a 12% higher rate of colonoscopy completion (p = 0.03). Other interventions were not associated with significant differences.
Conclusions
Almost all programs employ multiple interventions to ensure timely follow-up of positive FIT. The use of patient navigators and provider reminders is associated with higher rates of colonoscopy completion.
Introduction
Fecal testing for occult blood to screen for colorectal cancer (CRC) has been shown to reduce CRC incidence and mortality and is widely recommended beginning at age 50.1,2 The fecal immunochemical test (FIT) has largely replaced guaiac tests because it has higher sensitivity for CRC and improves participation. 3 CRC screening with FIT is a two-step process. Individuals with a positive or abnormal test (fecal hemoglobin level exceeding the stipulated positivity cut-off) are at higher risk for cancer, and should undergo a diagnostic colonoscopy. A systematic review found that the compliance with any second procedure was 81% in real-world screening programs using FIT, 4 probably due to multiple barriers at the patient-, provider- and system-levels. A recent European Union screening report showed wide variability across countries in compliance with colonoscopy referral. 5 Delays in colonoscopy greater than nine months are associated with an increased risk of CRC, particularly advanced-stage disease. 6 Inadequate follow-up of positive FIT may undermine the effectiveness of screening programs to reduce CRC morbidity and mortality. We aimed to collect data about strategies implemented by ongoing screening programs to improve follow-up for FIT-positive participants, and to explore associations between interventions and reported rates of follow-up.
Methods
We conducted a cross-sectional electronic survey of CRC screening programs or affiliated researchers worldwide between April and August 2019. We compiled a list of contacts from a recent publication on existing screening programs, 7 participants from a European Union consortium, 5 and the web. Ethics approval was not required, as we collected aggregate, system-level information. The survey was approved by the World Endoscopy Organization CRC Screening Committee. We emailed program contacts, and sent up to two reminders two weeks and two months after the first email. Given inconsistencies, we contacted all respondents a second time to ensure proper interpretation of reported information.
The electronic survey instrument consisted of 20 questions, including goals for the follow-up of positive tests, rates of referral and colonoscopy completion within six months, interventions in place to increase follow-up (divided into patient, provider and system-level interventions), and rates of colonoscopy completion stratified by participant race, education level, and socio-economic status (see supplementary materials).
We used descriptive statistics for program characteristics and interventions used to increase follow-up; means for the proportion completing colonoscopy at six months (or the nearest available time point); the Student’s t-test to compare the mean colonoscopy completion of programs that did or did not implement individual interventions to improve colonoscopy follow-up; and univariate linear regression analysis for the association between the number of interventions implemented and the reported proportion of colonoscopy completion. All results are presented without giving program names, but detailed results are available in the supplementary materials. Associations with a p-value ≤0.05 were considered statistically significant. All analyses were performed using STATA version 14.2 (Statacorp, College Station, USA).
Results
Thirty-five of 58 programs contacted completed the survey; four did not currently provide FIT screening (60% response). Eighty percent were national- or regional-level screening programs (n = 28), and 74% offered FIT only (n = 26), with a median of 90,000 participants screened annually (interquartile range 13,000 to 510,000). Most programs (74%, n = 27) set targets of three months or less between the time of a positive FIT report and colonoscopy completion. Five programs (9%) reported targets greater than six months or did not have a specific target.
The proportion of participants with a positive FIT who completed a colonoscopy within six months varied widely, from 39% to two programs that reported 100% colonoscopy completion. The mean among 32 programs providing results was 79% (standard deviation 16%). Mean colonoscopy completion was higher in 31 organized programs than three opportunistic programs (81% vs. 57%, p = 0.01), with one program not answering. Few programs collected data on colonoscopy completion stratified by race, education level, and socioeconomic status.
Reported interventions to improve colonoscopy follow-up are listed in Table 1. The mean number of interventions used was five, and only two programs used none. Interventions employed by more than half of the programs included notifying primary care providers of results (25 programs), providing the diagnostic colonoscopy free of charge (24), maintaining a registry to track FIT-positive patients (22), and using patient navigators (20). Overall, each additional intervention was associated with a 3% higher colonoscopy completion rate (p = 0.02). Individual interventions associated with higher mean colonoscopy completion rates were using patient navigators (difference in means 11%, p = 0.05), and sending reminders to primary care providers when no colonoscopy has been completed (difference 12%, p = 0.03).
Interventions to improve the follow-up of positive tests and frequency of use (n = 35).
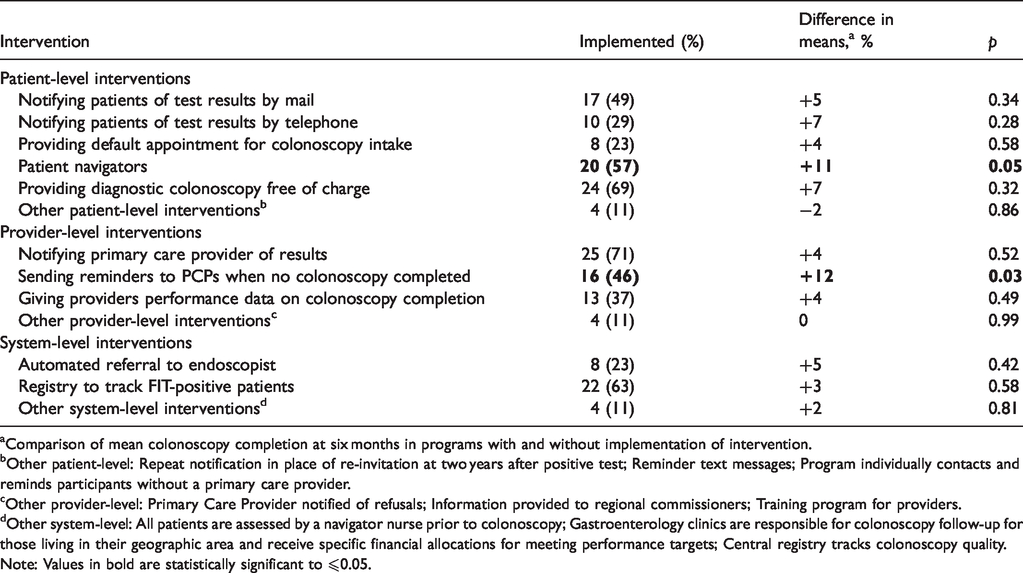
aComparison of mean colonoscopy completion at six months in programs with and without implementation of intervention.
bOther patient-level: Repeat notification in place of re-invitation at two years after positive test; Reminder text messages; Program individually contacts and reminds participants without a primary care provider.
cOther provider-level: Primary Care Provider notified of refusals; Information provided to regional commissioners; Training program for providers.
dOther system-level: All patients are assessed by a navigator nurse prior to colonoscopy; Gastroenterology clinics are responsible for colonoscopy follow-up for those living in their geographic area and receive specific financial allocations for meeting performance targets; Central registry tracks colonoscopy quality.Note: Values in bold are statistically significant to ⩽0.05.
Discussion
In an international survey of CRC screening programs, mean colonoscopy completion at six months after positive FIT was 79%. Factors associated with higher compliance were the use of primary care provider reminders, patient navigators, and a greater number of interventions. Three-quarters of programs have targets for colonoscopy completion within 90 days of a positive FIT.
These findings expand on previous research to provide worldwide data regarding current practices. Our mean colonoscopy completion rates were similar to a recent European Union report 5 and a meta-analysis of published reports.4 European and Canadian guidelines recommend follow-up with 30 and 60 days respectively, but little guidance is provided about how to achieve these targets.8,9 Current US guidelines do not specify a follow-up interval or preferred follow-up strategies. 3 Even so, nearly all programs we surveyed have implemented multiple interventions to ensure timely follow-up, and a greater number of interventions was associated with improved rates of colonoscopy completion. Specifically, programs using patient navigators and provider reminders reported higher rates of colonoscopy completion, supporting the results of a systematic review that found moderate evidence to support those interventions. 10
Our primary limitation is that a cross-sectional study cannot prove temporality or causation. However, several findings are consistent with previous interventional studies (i.e. range of follow-up rates, and use of provider reminders and navigators). Our sample may not be representative of all settings in which FIT is performed and followed up, and all data are based on self-report. We considered programs equally, regardless of their size, such that our results are strongly influenced by smaller screening programs. Nonetheless, our findings further reinforce the need for specific interventions to increase colonoscopy completion after positive FIT.
Supplemental Material
MSC904977 Supplemental Material1 - Supplemental material for Interventions to ensure follow-up of positive fecal immunochemical tests: An international survey of screening programs
Supplemental material, MSC904977 Supplemental Material1 for Interventions to ensure follow-up of positive fecal immunochemical tests: An international survey of screening programs by Kevin Selby, Carlo Senore, Martin Wong, Folasade P May, Samir Gupta and Peter S Liang in Journal of Medical Screening
Supplemental Material
MSC904977 Supplemental Material2 - Supplemental material for Interventions to ensure follow-up of positive fecal immunochemical tests: An international survey of screening programs
Supplemental material, MSC904977 Supplemental Material2 for Interventions to ensure follow-up of positive fecal immunochemical tests: An international survey of screening programs by Kevin Selby, Carlo Senore, Martin Wong, Folasade P May, Samir Gupta and Peter S Liang in Journal of Medical Screening
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PSL is supported by grant K08CA230162 from the National Cancer Institute. FPM is supported by grant R03CA230947 from the National Cancer Institute.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.