
Abstract
Objective
To test whether a telephone follow-up service for high-needs ethnic groups increases bowel screening participation in non-responders to postal invitations.
Methods
Māori, Pacific, and Asian ethnicity individuals who failed to return a bowel screening test kit within four weeks of it being posted were randomly allocated (1:1) to a telephone active follow-up service or a control group. The active follow-up service made multiple attempts to contact the invitee and provide support. Participation rates at eight weeks’ post-randomisation were compared, and the effect of the intervention on overall participation rates was imputed.
Results
A total of 3828 eligible individuals were allocated to active follow-up and 3773 to the control group. The imputed potential overall increase in participation in the active follow-up group was 2.0% (95% CI = 0.6%–3.4%); however, the impact of follow-up varied significantly by ethnicity and deprivation. The imputed increase in participation was significant for Māori (5.2; CI = 1.8%–8.5%) and Pacific (3.6%; CI = 0.7%–6.4%), but not for Asian ethnicities (0.7%; CI=−1.1%–2.4%). In addition, the imputed increase was significant among high deprivation participants (3.9%; CI = 2.0%–5.9%), but not among low deprivation participants (0.3%; CI=−1.6%–2.2%).
Conclusions
Active follow-up led to higher bowel screening participation in Māori and Pacific but not in Asian ethnicities and was more effective in high deprivation subjects. Active follow-up significantly reduced but did not eliminate ethnic inequalities in bowel screening participation.
Introduction
Cancer screening programmes can widen health inequalities, due to variation in participation among different social groups. 1 In New Zealand (NZ), this is evident from the lower participation in bowel screening by the most deprived ethnic groups: Māori – people of Pacific Island ethnicity (referred henceforth as Pacific) and Asians (a mix of predominantly Chinese, Korean, Filipino, Fijian Indian and Indian ethnicities).
Prior to the staged introduction of national bowel screening in NZ, a Bowel Screening Pilot was conducted over four years from late 2011 in Waitemata district (population around 450,000). Adults aged 50–74 received a postal invitation to participate every two years, using a faecal immunochemical test performed at home and posted to the laboratory for analysis. Following the invitation, a test kit was posted to invitees within two weeks. In the first round, participation within ethnic groups was Māori 46%, Pacific 30%, Asians 54% and people of other (mainly European) ethnicity 60%. 2
Although bowel screening participation has previously been reported to be lower among ethnic minorities,3–6 there are relatively few published studies of specific interventions (e.g. intensive follow-up of non-participants) to reduce these differences. There is strong evidence that reminders improve colorectal cancer screening uptake,5,7 but for bowel screening by posted faecal occult blood test (FOBT) or faecal immunochemical test, randomised controlled trials (RCTs) have not consistently found a positive effect on participation for telephone follow-up. Few trials have tested whether a (live) telephone reminder service in addition to, or instead of, a mailed reminder increases return of posted colorectal screening kits, and no published studies have used a population-based sample. RCTs assessing telephone reminders for mammography have likewise reported mixed results. 8
Among the seven relevant trials identified, two reported significant positive effects on screening participation. Among members of US-based Healthcare Incorporated, there was 9.7% higher participation in those randomised to a telephone reminder in addition to usual care with a mailed reminder (p < 0.005). 9 In a community health centre in the Pacific Northwest USA, there was 8.1% higher participation among the live phone call group than in the group allocated to reminder letters, but the group that received live phone calls in addition to a reminder letter had just 3.7% higher participation, which was not statistically significant. 10 In a factorial design RCT from Washington State, response rates to a telephone call made in addition to a postcard reminder were not significantly higher than to the postcard alone (93.3% vs. 92.7%), and the telephone call alone achieved only a 83.6% response rate (difference not significant). 11 A health centre RCT in Philadelphia reported 4.7% higher participation when a telephone reminder was added to the tailored intervention, but this increase was not statistically significant. 12 An Israeli clinic-based trial found that telephone reminders achieved significantly higher FOBT screening participation than letters (14.7% vs. 9.2%). 13 Telephone reminders did not significantly increase screening rates among individuals sent a faecal immunochemical test kit and written education materials in a trial in rural Iowa (57.2% vs. 56.5%). 14 Among Hispanic subjects in Washington State, telephone reminders and a home visit produced a non-statistically significant 5% higher participation rate in FOBT screening than a postal reminder. 15
It was recognised before the pilot began that bowel screening might exacerbate existing ethnic health inequalities. Initial efforts to reduce disparities focussed on raising community awareness, but when it became apparent that the inequalities persisted, a telephone follow-up service (active follow-up (AF)) was introduced for Māori, Pacific and Asian invitees who failed to return a kit within four weeks. Standard procedure for non-responders had been a reminder letter, but it was hypothesised that direct personal contact by telephone from someone of the same ethnic group in addition to the reminder letter could be more effective than the reminder letter alone, and that this could reduce ethnic differences in participation. This hypothesis was based on the investigators’ direct experience in a breast screening service and is supported by a recent meta-analysis of the value of cultural concordance in patient–physician interactions. 16 A text message follow-up intervention was rejected because of the perceived importance of direct contact, the frequent need to verify contact numbers and because an RCT had shown that automated text messages were significantly inferior to reminder letters, while ‘live’ phone calls were more effective. 10
As the pilot neared completion, the NZ government decided to extend bowel screening to the rest of the country. It was asked whether AF for Māori, Pacific and Asian groups should be incorporated as an integral part of the screening programme, but previous studies did not provide definitive guidance, and so an RCT was conducted to evaluate the impact of the AF service.
Methods
The study was a parallel group RCT with screening invitees as the units of randomisation. Screening invitees of Māori, Pacific or Asian ethnicity who failed to return a test with within four weeks of postage were randomly allocated 1:1 to either the AF or the control group. Group allocation was performed in batches two to three times per week, using a predefined simple random series generated from Excel®, by the principal investigator (who was not involved in the allocation process). Eligibility for bowel screening, Māori, Pacific, or Asian ethnicity, and failure to return a test kit within four weeks were the only criteria for entry into the study. The AF service commenced immediately after randomisation in those assigned to the intervention group. Four weeks following the initial invitation, subjects in both groups were sent a reminder letter, as was standard practice in the pilot.
The primary outcome (bowel screening participation evidenced by a test kit return) was measured at eight weeks from the date of randomisation (i.e. 12 weeks after the original invitation letter for bowel screening had been sent). Outcome assessment was set at eight weeks because in the pilot study approximately 90% of initial non-responders who eventually returned a test kit did so by this time. The outcome was ascertained from the Bowel Screening Register managed independently by the Ministry of Health. The outcome of test kit return was deemed to have been met even if it was a non-readable or incomplete return (e.g. missing specimen date). No allowance was made for postal delays or holiday periods.
With each randomisation batch, subjects were ordered alphabetically by National Health Index (NHI) code, thereby determining their group assignation. Although the randomisation sequence was available to the person in charge of completing the group allocation process, she had limited control over the dates of batch processing and the requirement to apply the randomisation key in order of NHI number meant that there was no possibility of selection bias. There was no stratification or blocking in the randomisation process. The randomisation sequence and group allocation were concealed from those implementing the intervention.
Figure 1 shows the study participant flow. Recruitment and randomisation commenced on 9 November 2016 and ended on 3 April 2017, with follow-up data collected until 29 May 2017 (eight weeks after last subject recruited). Recruitment was stopped once the target sample size had been reached.
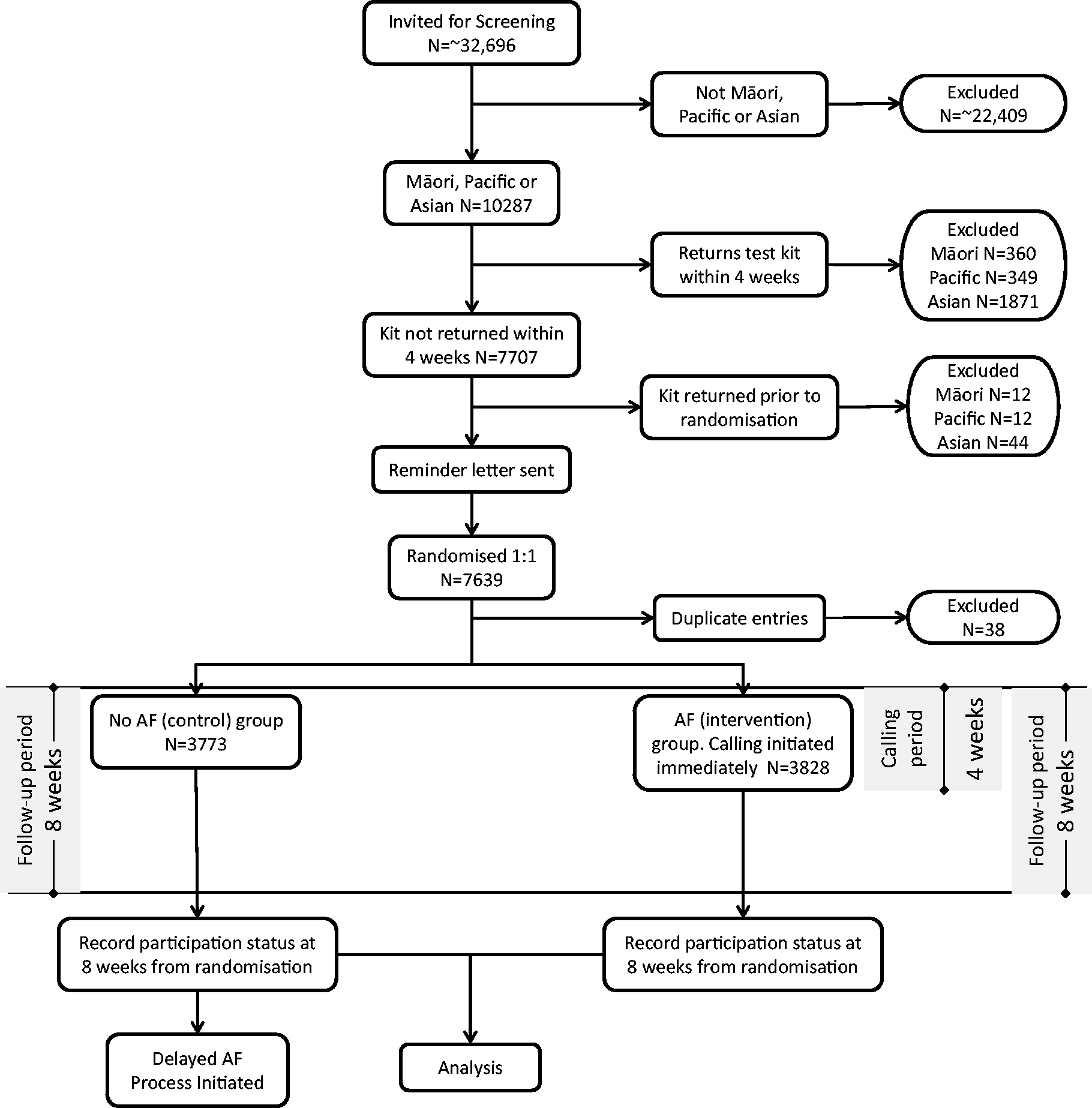
Subject flow diagram.
The ethnicity of study participants was determined by that recorded with their NHI number. Ethnicity in the NHI database, which allocates a unique health sector identifier, is highly accurate, although not perfect, particularly for ethnic subgroups.17–19 Individuals can have multiple ethnicities; however in NZ, it is common to apply a prioritisation to produce a single ethnicity code, where Māori overrides all other ethnicities, Pacific overrides all but Māori and Asian is recorded in priority to European. 20
Data on the individuals assigned to AF were extracted from the pilot study register and added to an Access® database available to Community Coordinator team (some employed directly by the programme, others by contracted third parties), who carried out the AF activities. Community coordinators, typically with a qualification in health promotion and selected for their cultural knowledge and links with the community, used the database to filter the population according to the ethnicity they serve. With some variation over time, there were generally 0.8 full-time equivalent (FTE) Māori Coordinators, 0.6 FTE Samoan/Other Pacific Coordinators and 0.9 FTE of Asian Coordinators (0.4 Chinese, 0.3 Korean and 0.2 Indian) employed.
Coordinators telephoned the individuals on their lists and recorded the call outcome. Asian and Pacific people were called by coordinators fluent in these languages and, where possible, the call was made in the relevant language; Māori were greeted in Māori, but the conversation continued in English. Calls were initiated typically within a day or two of randomisation to the AF group. Key performance indicators required a minimum of three phone calls to be made within a four-week period (from the date of assignment to AF), one of which had to be made after regular working hours. If no direct contact was possible, callers were not to leave a voice mail but should call back at a different time of day. If another person answered the telephone, the purpose of the call was never divulged, but an attempt was made to find a suitable time to call again. The coordinator’s number was withheld, so appeared as ‘Private Number’ on the invitee’s phone. For invalid numbers, other data sources were searched for current contact details. These include the hospital systems, the primary health organisation age/sex registers, the individual’s general practice and contacts the coordinators had within their own communities. Calls were not mere reminders, but sought to identify and remove any barriers that the subject might have to bowel screening participation (e.g. incorrect address or uncertainty over how to perform the test). The callers’ script was reviewed by health literacy experts. Subjects were provided with replacement kits when needed.
The control group received only the reminder letter until eight weeks following randomisation, when the primary outcome was measured. As they received no AF prior to outcome measurement at eight weeks, they are classified in the results section as ‘No AF’. For ethical reasons, and because it partially concealed group allocation to those delivering the intervention, the control group was provided with the AF service on exiting the study after eight weeks.
Study subjects were unaware of group allocation. The laboratory receiving the test kits recorded results onto the bowel screening register automatically and had no information on group allocation. Group allocation was also concealed from those delivering the intervention, although in the first eight weeks of the trial, they could have assumed that all of their referrals for follow-up were from the intervention group.
The study was designed with 90% power to detect a 5% overall and ethnic-specific (Māori, Pacific or Asian) absolute difference in participation at the 0.05 level of significance. The target sample size was 7224. The ethnic-specific differences in participation between the AF and No AF groups were pre-specified secondary study endpoints to be calculated regardless of whether there was evidence of interaction or effect modification.
Data were analysed on an intention-to-treat basis, including participants who left the study zone after randomisation, and those who died during the eight-week follow-up period. Shortly after the study commenced, it emerged that 38 subjects had been randomised more than once, due to a procedural error. These subjects were excluded from the analyses. Exploratory analyses were conducted to assess whether the impact of the intervention varied by gender, age or area deprivation. Area deprivation was derived from a census meshblock look-up table provided by the University of Otago, which was linked to the subject’s address. 21 The statistical significance of this potential effect modification was tested in a log-binomial regression model, controlling for age, sex, ethnicity and area deprivation. 22 The interaction effects were presented on both a multiplicative scale using the relative risk and maximum likelihood confidence limits for the interaction term, and an additive scale using the relative excess risk due to interaction with percentile bootstrap confidence limits (2000 replications per estimate).23,24
CONSORT guidelines were followed. The trial was approved by the NZ Health and Disability Ethics Committee (reference 16/NTA/159), acknowledging that obtaining consent from subjects would not be feasible. Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12616001487404).
Results
After excluding the 38 duplicate entries, data from 7601 subjects (3773 in the control group and 3828 in the AF intervention group) were available for analysis. There were five deaths in the interval between randomisation and follow-up completion, three in the intervention group and two in the control group. These were included in the analysis, consistent with the intention-to-treat approach.
Table 1 summarises the basic characteristics of the AF and No AF groups. No statistically significant differences between them were found. The relatively high proportion of subjects under age 60 reflects both the younger demographic of these ethnicities compared with the majority European ethnic group and the lower rate of participation in younger age groups.
Baseline characteristics of study subjects by group allocation.
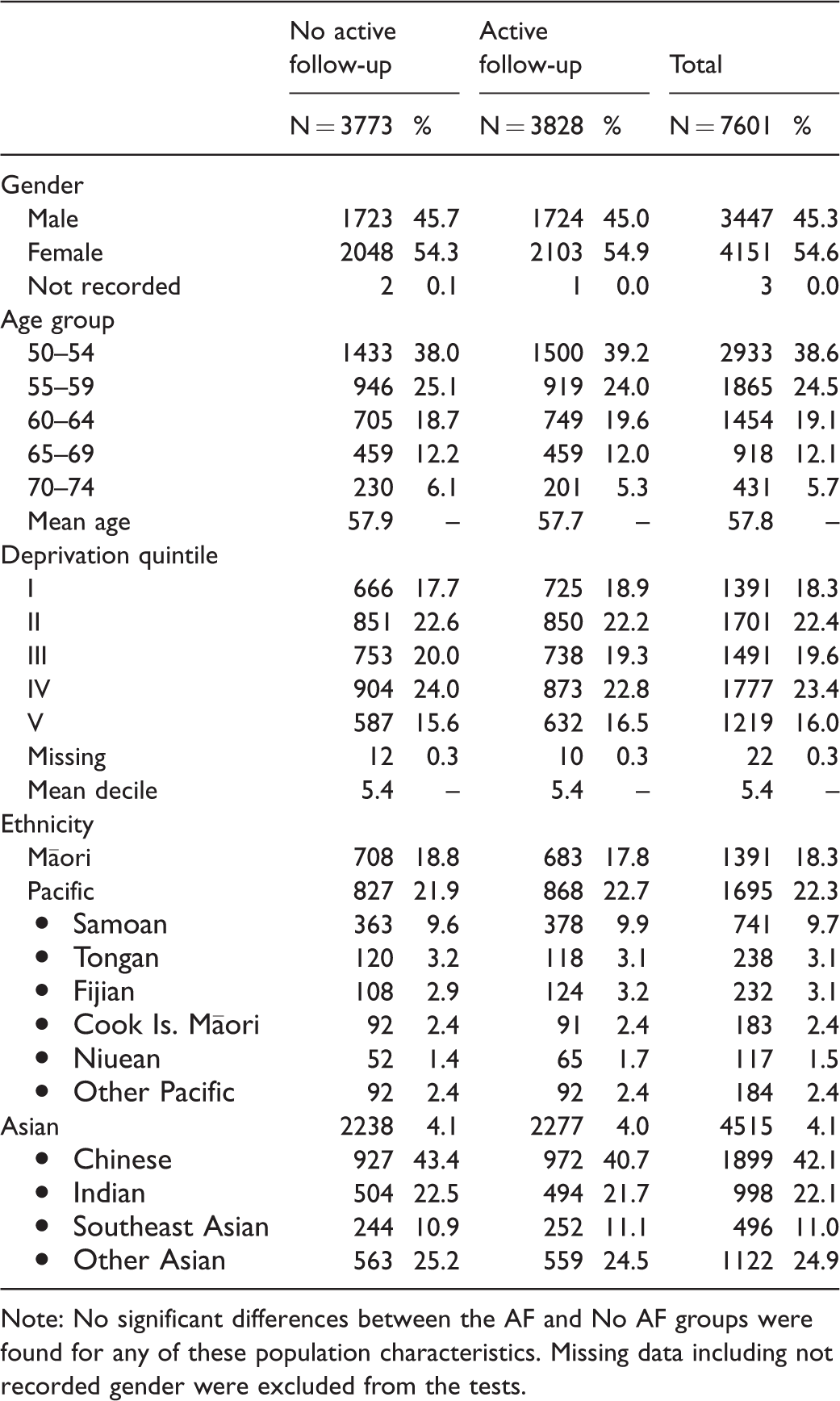
Note: No significant differences between the AF and No AF groups were found for any of these population characteristics. Missing data including not recorded gender were excluded from the tests.
Table 2 presents outcomes by randomisation group overall, by ethnicity and by area deprivation which was the only other subgroup (in addition to ethnicity) found to significantly modify the effect of the intervention, as shown by the log-binomial regression interaction term in Table 3. The impact of the AF intervention varied significantly by ethnicity (likelihood ratio test of two-level interaction term, χ2=8.31, 2 df; p = 0.016). The increase in screening participation attributable to AF was statistically significant for Māori and Pacific, but not for Asian ethnicity participants, where the difference between intervention and the control groups was just 0.95% and not statistically significant (Table 2). Exploratory analyses were performed to look for heterogeneity in the impact of the intervention within the Pacific and Asian ethnic sub-populations, but as the interaction terms in log-binomial regression models were not significant for either Pacific or Asian subgroups, no further analysis was conducted. The final column of Table 2 imputes the expected impact of the AF intervention on overall screening participation rates (assuming it were implemented in all eligible subjects), taking into account the proportions in each stratum who return kits by four weeks.
Participation by ethnicity and deprivation: before and during trial with imputed gains in overall participation attributable to AF.
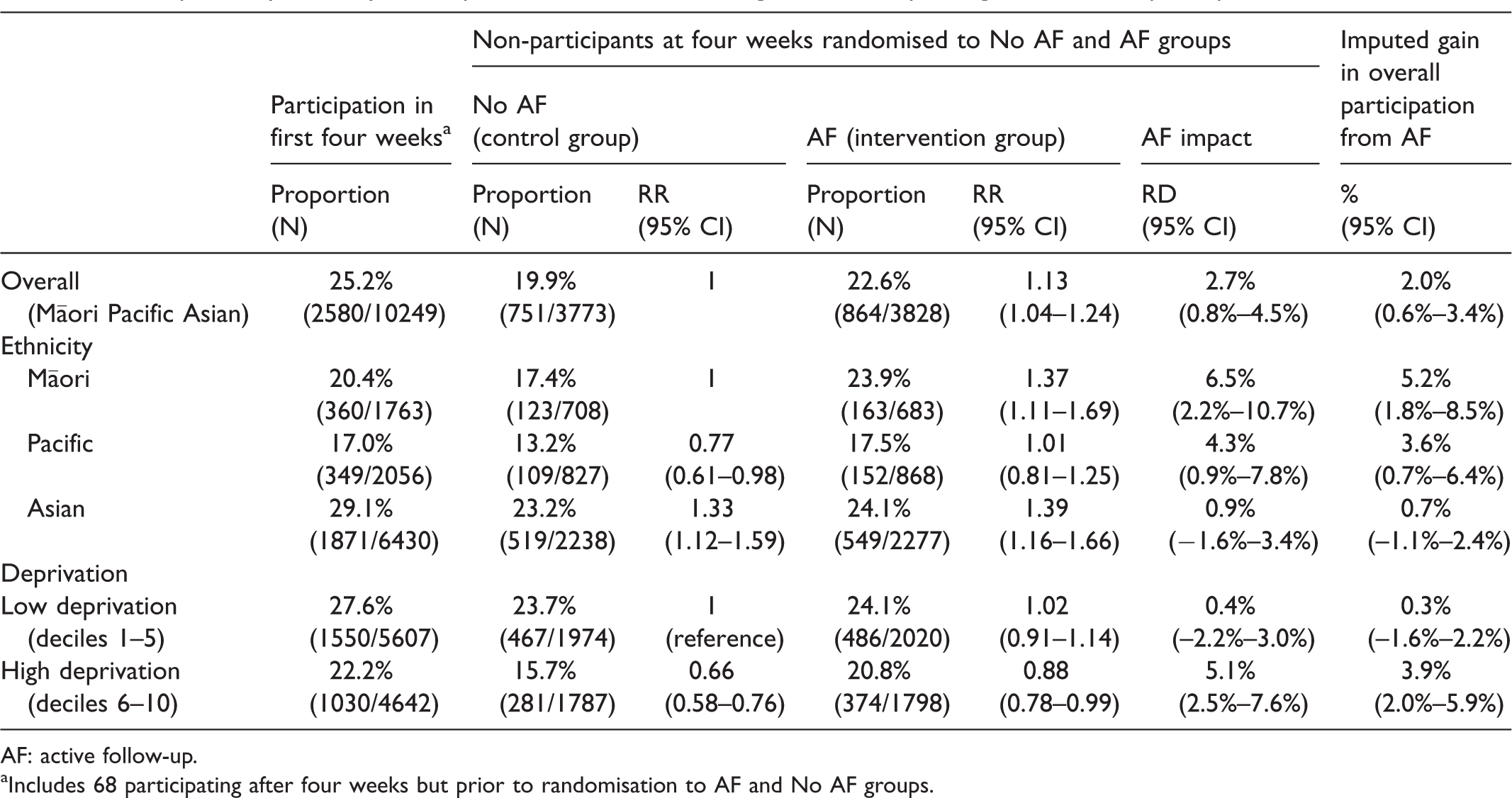
AF: active follow-up.
aIncludes 68 participating after four weeks but prior to randomisation to AF and No AF groups.
Potential effect modifications on the impact of active follow-up, tested by log-binomial regression.
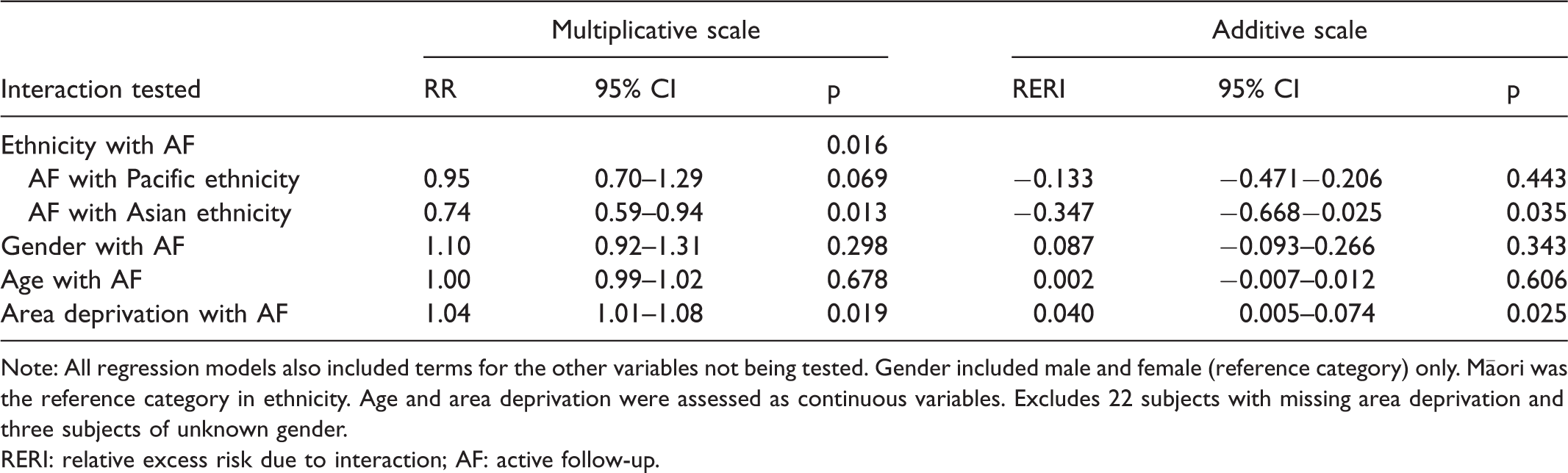
Note: All regression models also included terms for the other variables not being tested. Gender included male and female (reference category) only. Māori was the reference category in ethnicity. Age and area deprivation were assessed as continuous variables. Excludes 22 subjects with missing area deprivation and three subjects of unknown gender.
RERI: relative excess risk due to interaction; AF: active follow-up.
Area deprivation was a significant modifier of the effectiveness of AF, its effect on the impact of AF being confirmed by the significant interaction term when assessed separately on both multiplicative and additive scales (Table 3). The AF intervention was significantly more effective in those of higher deprivation. In Table 2, where deprivation has been dichotomised into low deprivation (deciles 1 to 5) and high deprivation (deciles 6 to 10), AF led to a negligible increase in screening participation in low deprivation subjects (0.4%), but had a strongly positive effect in high deprivation subjects (5.1%).
Area deprivation varies considerably by ethnicity, with lower mean deprivation among those of Asian ethnicity (4.7) than Māori (5.8) or Pacific (6.9). However, the multiple log-binomial regression model demonstrated that even when deprivation is controlled for, ethnicity remains a significant effect modifier and, conversely, deprivation remains a significant effect modifier when ethnicity is controlled for. The three-way interaction term for ethnicity, deprivation and AF was not significant. However, the interaction effect of both deprivation and ethnicity lost statistical significance when both were included in the log-binomial model, suggesting that there may be some overlap in the way that these factors affect the impact of AF.
In 95% of those in the AF group who failed to return a test kit, it was possible to assess whether the service had succeeded in contacting the subject or his/her household. Among these, in 43.2%, there was no record of any contact having been made. That proportion was significantly higher among Asians (62.6%), than among those of Pacific (20.5%) or Māori (7.9%; p < 0.00001) ethnicity. Rates of no contact also varied significantly within ethnic groups: 42.4% among Chinese Asians compared with 77.5% in the non-Chinese Asians (p < 0.0000001), and 13.0% among Samoan compared with 29.0% among non-Samoan (p < 0.00001).
Discussion
Although this is not the first study to report the impact of telephone reminders on bowel screening participation in Asians, it is the first to report it in Māori and Pacific ethnic groups. It is one of only three studies (out of eight) that has demonstrated a positive impact of telephone follow-up on screening participation in non-responders to postal bowel screening invitation.9–15 It therefore contributes to the evidence that telephone follow-up can lead to higher bowel screening participation; however, the results show that this may depend on the group being targeted, which was noted with another intervention introduced to raise participation rates in this programme. 25
The impact on faecal immunochemical test completion rates was statistically significant overall, and among deprived Māori, Pacific and high deprivation subgroups. It was effective in males and females, and across the full age range, but it was not effective among Asians nor among those living in areas of low deprivation. The differential efficacy according to area deprivation could be seen as a positive outcome from an equity perspective, and something that has not been explicitly studied previously (although the review by Duffy et al. noted that personalised reminders for screening programmes are effective in low socioeconomic status groups 26 ).
The ethnic heterogeneity is not necessarily due to cultural differences between the three groups. The number of Asian subjects was almost 50% higher than the combined total of Māori and Pacific subjects, but the staffing was not proportionately higher, making it difficult to provide the same level of service for each. This difference is reflected in the higher rates of no contact that were observed with Asians than Māori or Pacific.
Although area deprivation was also associated with greater AF impact, the relatively lower deprivation of Asian subjects may have partly explained the lack of AF impact in that group. The possibly higher impact of AF on those of high deprivation, if a true effect, would imply a positive impact for the intervention on health inequalities, which was the key driver for this intervention in NZ.
Despite the significant impact of AF on Māori and Pacific participation rates, the imputed gains would not have been sufficient to completely eliminate the gap with the European and Other group, which had a four-week participation rate of 31.4%. It would therefore need to be combined with other effective pro-equity strategies.
Key strengths of this trial were its large sample size, simple design, unequivocal outcome measure, broad eligibility criteria, low loss to follow-up and generally high-quality ethnicity data. The use of a randomised controlled design supports a causal interpretation for the main finding. The study tested a well-defined intervention applied in a real-world setting, facilitating replication elsewhere, but especially in NZ, where it has already made a tangible contribution to bowel screening policy.
One limitation of this RCT was that the data recorded by the coordinators were not of sufficient detail and quality to assess the extent to which the kit return could be attributed to success in establishing contact with the subjects and related to the timing of those contacts. There was considerable variation by ethnicity in the proportion of subjects for whom there was no record of contact being established, but there are several possible explanations for this, including inaccuracies in telephone records, lower staffing levels for the Asian coordinators, ethnic differences in the frequency of change of abode and possibly a tendency for coordinators to have greater success at contacting those of their own ethnic subgroup. Better information systems might provide greater insight into reasons for the heterogeneity of AF impact, including quantitative data on the nature of the barriers faced by non-participants. Better information systems could also provide useful feedback to coordinators, to help them to improve the efficacy of their contacts.
Sample size, though large, was not sufficient to power tests of effect modification within ethnic subgroups. In particular, Asians are a highly diverse group with major cultural and linguistic differences among the three main subgroups, Chinese, Indians and Southeast Asians.
Previous studies have not provided confidence that telephone follow-up of postal colorectal screening invitation is always effective. Our study found that, although overall the intervention was efficacious, there was significant variation by ethnicity and area deprivation. This suggests that contextual factors such as staffing levels, training, access to accurate and up to date telephone records and the ethnicity of the person responsible for follow-up are significant determinants of impact. Further research is warranted to determine the relative importance of these factors.
In contrast to other reported interventions, the AF programme was implemented specifically to reduce health inequalities. AF provided more than just a reminder. It also assisted with logistic barriers (such as incorrect addresses) and confusion over how to perform the test, and provided subjects with an opportunity to be reassured about the benefits of the test. The telephone calls also helped to formally 'opt out' those subjects for whom a CRC screening test would be inappropriate, and those who had made an informed decision not to undertake the test.
Telephone reminders cost approximately 10 times more than postal reminders, 4 and so may not be feasible or cost-effective to apply to all non-respondents. Our findings show that even if unaffordable for all non-respondents, telephone follow-up may help to achieve equity goals, especially given its higher impact among those in areas of greater deprivation. Future applications might consider targeting those living in areas of high deprivation.
A significant proportion of non-respondents four weeks after being invited to undergo screening subsequently return a test kit, even without telephone follow-up. Delaying the instigation of AF by a few weeks might make telephone follow-up more efficient, by not intervening with many of those who will return a kit anyway.
Conclusions
The AF service had a statistically significant and meaningful impact on Māori and Pacific but not Asian participation in bowel screening. The failure in the Asian group may be partly due to lower rates of patient contact. Effectiveness of the AF intervention correlated with the level of area deprivation of the subject’s residence. AF can therefore make a valuable contribution to reducing ethnic and socioeconomic inequalities in bowel screening participation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.