
Abstract
Objective
Cervical cancer screening by human papillomavirus (HPV) testing requires the use of additional triage and follow-up analyses. We evaluated women’s compliance with and the performance of this strategy in a routine setting.
Setting
Five cervical service screening programmes in North-East Italy.
Methods
Eligible women aged 25-64 invited for a new screening episode underwent HPV testing for high risk types (hrHPV by Hybrid Capture 2) and cytology triage. Women with positive HPV and cytology results were referred for colposcopy; women with positive HPV but negative cytology results were referred to 1-year repeat hrHPV testing.
Results
Of 46,694 women screened by HPV testing up to December 2011, 3,211 (6.9%) tested hrHPV positive; 45% of these had a positive triage cytology. Those with negative cytology were invited for 1-yr repeat testing. Compliance with invitation was 61.6% at baseline and 85.3% at 1-yr repeat. Rate of persistent hrHPV positivity was 58% (830/1,435). Colposcopy performed in women with a positive hrHPV test at 1-yr repeat accounted for 36% of all colposcopies performed within the screening programmes. Cumulatively, a histological high-grade lesion was detected in 276 women (5.9‰ detection rate), 234 at baseline (85%), and 42 (15%) at 1-yr repeat.
Conclusions
Compliance with hrHPV-based screening programmes was high both at baseline and at 1-yr repeat. Compared with the randomized trials, a higher proportion of triage cytology was read as positive, and only a small number of high-grade lesions were detected among the group of hrHPV positive cytology negative women who repeated testing 1-yr after baseline.
Introduction
A subset of Human Papilloma Virus types, defined as high-risk (hrHPV), cause cervical cancer 1 , and testing for hrHPV (hereafter referred to as HPV testing) has been investigated as a primary screening test in several randomized clinical trials (RCT).2–12 Cross-sectional as well as longitudinal results have consistently demonstrated the superiority of HPV testing, compared with Pap testing, to prevent invasive cervical cancer by detecting high-grade precancerous lesions. 13 However, HPV testing is also associated with a lower specificity, especially in younger women. Therefore, some triage of HPV-positive (hrHPV+) women is required. Different triage options have been compared. 14 The most feasible, and the only one already tested in pragmatic trials under routine conditions, is cytology followed by colposcopy when the result is positive, and by repeat testing when the result is negative.
Many feasibility projects are being performed in Italy within organized service programmes, in order to better define the performance of HPV testing in the routine setting, outside of a research context.15–16
A critical aspect of an HPV-based screening programme with a cytological triage for HPV+ cases is represented by the group of HPV+/cytology negative (cyto-) women; these women are informed of the positive HPV result and are asked to wait 12 months without any further ascertainment, after which time they are invited to repeat the test. What has not been shown is whether these women will comply with the screening algorithm, or seek reassurance by seeking other exams in the interval, outside the screening programme, nor how the repetition of the HPV test will work in routine service screening programmes.
We here present the results of an HPV-based screening strategy in 25–64 year old women attending five organized screening programmes, with particular attention to the performance of the recall after one year of the cases with HPV+/cyto- at baseline.
Methods
Service screening programmes involved in the study.
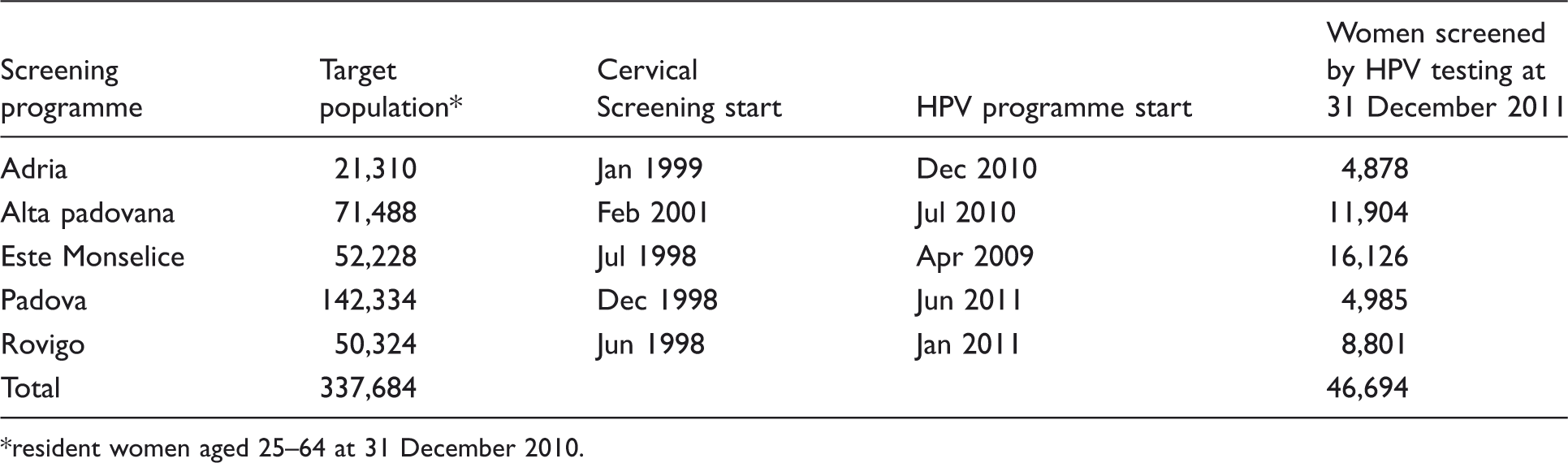
resident women aged 25–64 at 31 December 2010.
As previously described 16 , the screening protocol followed the GISCi (Italian Association of Cervical Screening Programmes) guidelines 19 and the contents of a Health Technology Assessment Report on HPV DNA based primary screening 20 (published in 2012), except for screening interval (three years instead of five) and women’s age (HPV test also in women aged younger than 30). Three years after the previous screening episode, eligible women received a letter of invitation and a leaflet with some information about HPV, the hrHPV test, and the new screening programme. If women did not respond to the invitation, they received a reminder by mail. A double sampling for cytology (conventional or liquid based) and for HPV testing was performed on all participating women. As was previously done with the cytology strategy, virgins (after being advised that they could postpone initiation of screening) underwent Pap smear alone, instead of an HPV test, because of its higher specificity.
Cervical cells were analyzed by Hybrid Capture 2 (HC2, Qiagen) with the High Risk probe set, according to the manufacturer’s instructions, using the Rapid Capture System (RCS, Qiagen) (see reference 16 for details). All samples with a Relative Light Units / Positive Control (RLU/PC) ratio ≥1 were considered positive. The corresponding Pap smears were processed, and read by a cytologist who was aware of the HPV+ result. The results were reported according to the 2001 Bethesda System; 21 a diagnosis of ASC-US+ (atypical squamous cells of undetermined significance - or worse) was considered as positive, and prompted referral to colposcopy. A diagnosis of less than ASC-US was referred to repeat the HPV test one year later. Inadequate Pap smears were repeated.
Women with negative cytology were informed of the result by letter, and 12 months later received a written invitation to repeat the HPV test; women who did not respond were contacted by telephone and asked whether they had already undergone testing (these data were not included in our analyses). Again, two samples were taken (for the HPV test and for cytology) and the HPV test was performed. The women who tested HPV negative returned to screening. Those who remained HPV positive were all referred for colposcopy, their Pap smears were processed, and the diagnoses were made available to the gynaecologists who carried out the colposcopies.
The indicators utilised to evaluate the HPV-based programme were:
– response to invitation (screened women/invited women) – positivity at HPV test (HPV+ tests/HPV tests) – referral rate to colposcopy (screened women referred for colposcopy / screened women) – positive predictive value (PPV) for CIN2+ at colposcopy (colposcopies with histologically confirmed CIN2+/colposcopies) – detection rate (DR) for CIN2+ (women with histologically confirmed CIN2+/screened women)
both at baseline (including post-colposcopy follow-up) and at the one-year repeat in women HPV+/pap- at baseline. The results were stratified by age (25–29, 30–34 and over 35 years).
Statistical analysis
The results of the main indicators of the HPV programme were compared across groups using the χ 2 test or χ2 test for trend or logistic regression, as appropriate. The performance of HPV followed by a cytology triage as the follow up strategy for HPV+/cyto- women was evaluated, by calculating the relative frequencies of the main indicators, and comparing with HPV test alone, with 95% confidence intervals. P-value was fixed at 0.05.
Results
By the end of December 2011, the five programmes together screened, by HPV testing, 46,694 women, as detailed in Figure 1; 31.1% attended their first screening episode, and 68.9% were at a subsequent round, with an overall 61.6% adjusted compliance with invitation.
Flowchart and main data of the HPV-based screening programmes.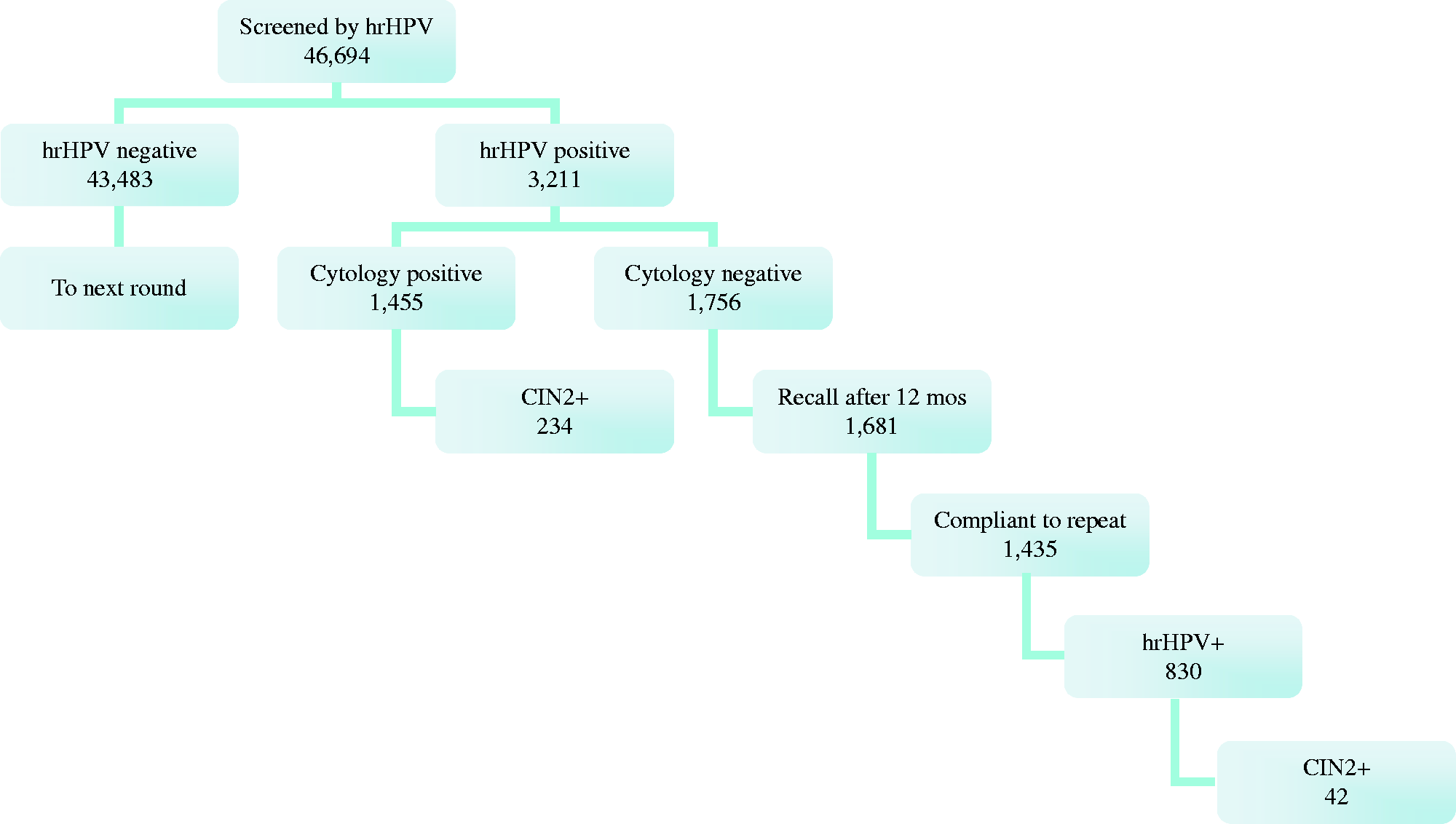
Distribution of Relative Light Units / Positive Controls (RLU/PC) ratios among women with CIN2+ lesions at baseline, by age.

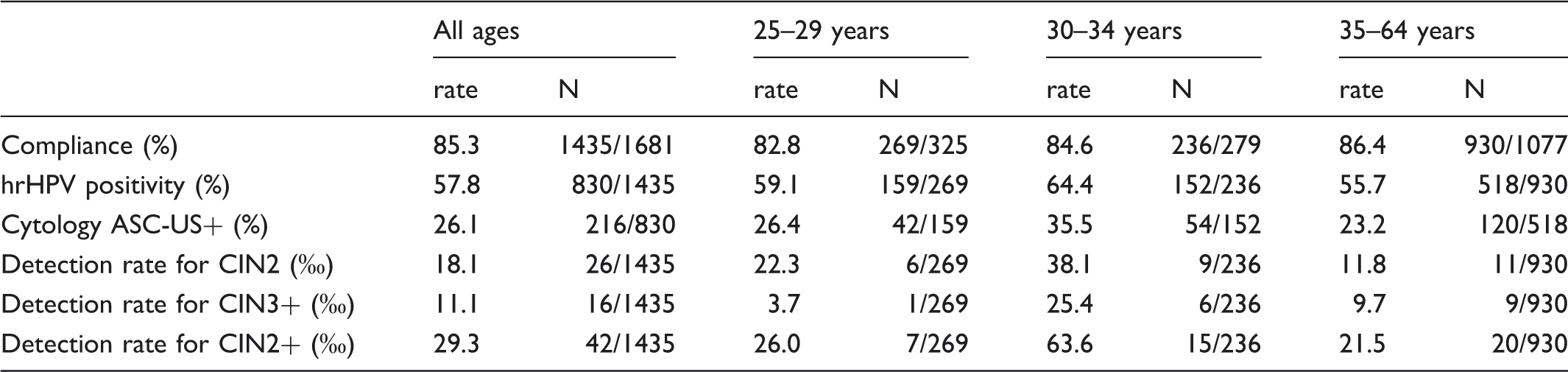
Main outcomes for the group of hrHPV+/cyto- women recalled after one year, by age.
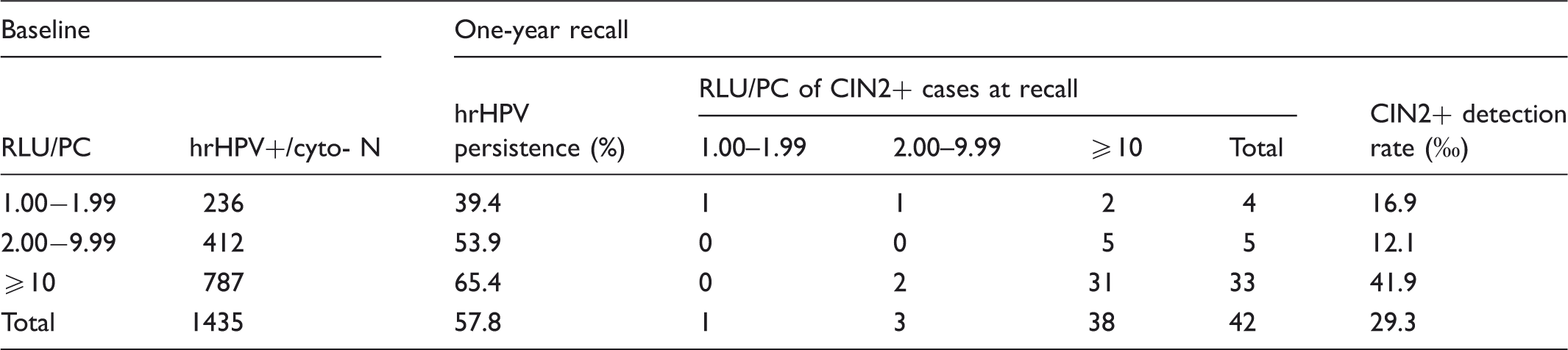
Distribution of CIN2+ detected at one-year recall, by Relative Light Units / Positive Control (RLU/PC) at baseline and at recall, and baseline-RLU/PC-specific detection rate at the recall.
All HPV+ women were referred for colposcopy, irrespective of cytology result, with a compliance of 96.6%. A high-grade lesion was detected in 42 cases (16 CIN3 and 26 CIN2), with a detection rate for CIN2+ of 29.3‰ (11.1‰ for CIN3 and 18.1‰ for CIN2), higher in those aged 25–34 (43.7‰) than in older women (21.5‰) (χ2 test 5.25, p = 0.02).
Among the women diagnosed with CIN2+, the RLU/PC ratio of the samples at 1-yr recall was ≥10 in 38/42 (90.5%). The ratio of the corresponding baseline specimens (Table 4) was 1.00–1.99 in four cases (9.5%), 2.00-9.99 in five (11.9%) and ≥10 in 33 (78.6%). One case of CIN3 had a ratio between 1.00–1.99 in both (baseline and 1-yr recall) specimens; CIN3 was diagnosed in the biopsy and only koilocytosis was detected in the excised tissue. The other three CIN2+ cases with a 1.00–1.99 ratio at baseline showed a higher ratio at recall.
The DR for CIN2+ by the value of RLU/PC ratio at baseline was highest (4.19‰) for the ≥10 group, compared with the 1.00–1.99 (1.69‰) and the 2.00-9.99 (1.21‰) groups, respectively; the difference, however, was not statistically significant across age-adjusted ratio as a continuous variable (p = 0.301 at logistic regression).
The DR for CIN2+ at 1-yr recall relative to the total screened cohort was 0.9‰ (42/46,694); the overall DR for CIN2+ of the HPV programme (baseline + 1-yr recall) was 5.9‰ (276/46,694). The proportion of CIN2+ detected at the 1-yr recall was 15.2% (42/276).
Colposcopies performed at 1-yr recall represented 36% of all the colposcopies of the HPV-based screening strategy, and the PPV for CIN2+ was 5.7%.
Comparison of hrHPV test alone vs hrHPV test + cytological triage as strategy to follow up hrHPV+/cyto- women.

Discussion
This study reports the results on the performance in terms of acceptability, compliance, detection rate, and positive predictive value of a HPV-based screening strategy with cytological triage in 46,694 women aged 25–64, attending five organized screening programmes in North-East Italy.
Overall, in comparison with the previous cytology-based strategy, a roughly 10% higher compliance at baseline was recorded, in line with what was observed in the first implemented programme. 16 The compliance with 1-yr follow-up repeat was also high (85%). This is an important result because compliance with this step of the HPV-based screening protocol is a critical issue. It represents a major difference from the Pap-based strategy, and low rates have previously been observed, in randomized trials as well as in routine settings, and it can affect screening efficacy.11,15,22 While compliance with immediate colposcopy was high (∼90%) in all randomized controlled trials, compliance with repeat testing varied considerably: 55% in the United Kingdom 11 and 94% in Italy. 9 Different contextual factors may potentially affect compliance: the level of fidelity that a screening programme has built with its target population before the introduction of the HPV-based strategy, the method of invitation, and time and type of the repeat test. The first routine HPV-based screening implemented in Italy 15 reported low compliance with invitation, possibly because it was introduced in a district that had not been previously covered by the traditional pap-based programme, and no systematic telephone reminder to non-compliant women was carried out. However, results on primary HPV testing in cervical cancer screening outside a research context are still scarce.4,15,16
The contribution to the overall CIN2+ detection rate of the recall of the group of HPV+/cyto- women was substantial (15.2%), confirming the importance of this step of the protocol. It is, however, lower than expected.
Before the start of the HPV-based strategy, the five programmes used cytology as the screening test. The overall detection rate for CIN2+ in the last three years was 2.7‰. The DR at baseline of the HPV-based programmes was 5.0‰, with a further 0.9‰ obtained by the recall of HPV+/cyto- women. The overall DR was therefore more than doubled with the HPV strategy, but most of the increase occurred at baseline rather than at 1-yr recall, the latter adding only a marginal proportion of lesions. It would not be expected to observe similar differences between the DR of the Pap-programme and the HPV-programme at baseline, because in both strategies only women with a positive cytology are referred to colposcopy and contribute to the DR. 4 In theory, the excess of diagnoses of the HPV-based programme should derive from the follow-up of HPV+/cyto- women.
Our hypothesis is that the reading of a Pap test in a triage situation is very different from that of a primary pap test. The knowledge of a positive HPV test result plausibly induces a different interpretation of some findings. 14 Very low numbers of cells with low-grade abnormalities, that otherwise would be considered as negative, may be reported as positive. This could explain both the higher than expected increase of the DR at baseline, and the low rate of CIN2+ left in the recalled women.
Whether this is correct or not, it is probably unavoidable, given the impossibility, in our setting, to blind the reading of the triage cytology at baseline. We recorded a decrease with time of the HPV+/cyto+ cases, as a result of experience, and courses for specific training have already been carried out in Italy. However, this point should be carefully considered in order to fully understand the performance of the current repeat strategy (1-yr HPV testing) and to identify the best way to improve it.
The use of different RLU/PC ratios as an alternative strategy has been suggested. 23 A higher cut-off might be used either to redefine the HPV-positive category (ie. cut-off at ≥2: women with a ratio <2 go to the next round) or to triage the women (ie. cut-off at ≥2: women with a ratio between 1.00 and 1.99 are referred to 1-yr follow-up, as well as women with higher ratio but negative cytology). Most data published to date derive from randomized controlled trials in which HC2 for high-risk HPV types has been used. Differences in HC2 performance have been observed in relation to the transport medium, and some variation in the reproducibility for equivocal (close to the-cut-off) values has also been described in relation to women’s age, with the suggestion to differentiate the cut-off by age. 24 The use of a higher cut-off (ie. ≥2) would increase the specificity of the HPV test, and decrease the referral rate to colposcopy. In most cross-sectional studies5,6,16,25–28 HPV infections characterized by 1.00–1.99 RLU/PC ratios appeared rarely/never associated with high-grade lesions. Our data suggest that some CIN2+ may be detected at baseline, or develop during follow-up (4/234 and 4/42, respectively, in our experience), in women who test HC2-positive at 1.00–1.99 ratio. At present, the natural history (ie. rates of regression/progression) of lesions associated with lower HPV viral loads is not known.
The protocol utilized to follow up HPV+/cyto- women showed some limitations. We observed a 42% HPV clearance rate, a figure at the lower end of the rates reported in the literature.29,30 This increased the workload of colposcopy and negatively affected the PPV for CIN2+ (5.9%) at 1-yr recall.
A possible alternative to improve the efficacy of the protocol is lengthening the interval for repetition (ie. to 18 months), in order to increase the clearance rate. The acceptability of this to the target population should, however, be evaluated in terms of compliance, and of spontaneous uptake of extra-tests during the interval.
Our results will be compared with those from different protocols, such as the repetition of cytology alone after six months, planned in the Netherlands 31 , although this strategy may raise some concern about acceptability, because it will not be possible to monitor the HPV positivity detected at baseline. Reassuring women about their state of infection would be a further considerable educational challenge, to be added to the complicated issues surrounding HPV infection and the natural history of cervical cancer. 32
Almost 5% (1,455+830/46,694) of women were cumulatively referred to colposcopy, but high-grade lesions were not detected in the majority (88%; 1221+788/2285). Because colposcopies performed at 1-yr repeat accounted for 36% of the total, additional triage at this stage could decrease the amount of unnecessary referrals. Our data did not allow evaluation of the performance of cytology alone at repeat, because it was performed only in HPV+ cases. As we evaluated the performance of HPV followed by a cytological triage also at 1-yr recall, this would reduce the referral rate to less than one third, but lose about 40% CIN2+ lesions.
Other tests are under evaluation as biomarkers for triage of women with HPV infections. Immunocytochemistry for p16INK4a expression (now available as dual stain with ki67) has been demonstrated as a good triage test. 33 Other promising cytological biomarkers are the methylation status of cellular genes (ie. cell adhesion molecule 1 - CADM1, and T-lymphocyte maturation associated protein - MAL), the partial HPV genotyping (HPV16 and HPV18 have higher probability than other hrHPV types of persistence and lesion progression), as well as other viral parameters, but their clinical value has not yet been definitely assessed. 34
Age has been shown to affect the performance of HPV-based screening. Gains in sensitivity and loss in specificity vs cytology are larger among younger women and decrease with increasing age. 20 Overdiagnosis of CIN2+ (and particularly of CIN2) is higher among women aged under 35, 12 leading to the recommendation not to start the HPV-based screening before age 30/35 years. 20 The higher occurrence of lesions that have lower probability to progress and/or persist in younger women may account for these higher rates. The pooled data from four large European randomized controlled trials 13 on HPV-based vs cytology-based screening in preventing invasive cervical cancer suggest a gain in efficacy with HPV testing, starting from age 30. In our study, among the women HPV+/cyto- at baseline and retested at 1-yr follow-up, the group aged 30-34 showed the highest rates of HPV persistence, abnormal cytology, and DR for CIN2+; the lowest HPV-to-cytology rate ratio of invasive cancers in the pooled analysis was observed for this age group. 13
Applying HPV testing to all the target population (ie. women aged 25–64, as in our pilot project), optimal triage of young HPV+ women is of utmost importance. Differences by age in the performance of some triage tests have also been observed 33 , and may reflect the fact that prevalent infections are usually more recent in younger than in older women.
Conclusion
Our feasibility project on the performance of HPV testing with cytology triage in routine screening programmes yielded a high compliance in the target population, both at baseline and at 1-yr repeat for HPV+/cyto- women. Our data highlighted some differences compared with the randomized trials, in particular, a larger than expected proportion of high-grade diagnoses made at the baseline, probably resulting from a higher rate of abnormal cytology.
Footnotes
Acknowledgments
The authors thank Martina Rizzi for her technical assistance, and all the operators of the screening programmes for their contributions to this study.
Funding
This work was supported by Fondazione Cassa di Risparmio di Padova e Rovigo. The funder had no input in the design, conduct, analysis or interpretation of the data, or the preparation, review or approval of the manuscript.