
Abstract
Objectives
To estimate the impact of increased participation in screening, and of the proposed change from Pap to human papillomavirus screening on the incidence of cervical cancer in British Columbia.
Methods
For invasive cervical cancer cases diagnosed in British Columbia between 2002 and 2011, data were extracted on age and cancer morphology from the British Columbia Cancer Registry, and Pap screening history was obtained from the British Columbia Cervical Cancer Screening Program database. Only screening performed two to seven years prior to diagnosis was assumed to reduce subsequent risk of cancer. Results from randomized trials of human papillomavirus versus cytology screening and population based estimates of cytology screening were used to estimate the effect of a change in screening test and increases in participation.
Results
Between 2002 and 2011, there were 1663 cases of cervical cancer reported; 660 (367 squamous and 293 non-squamous) were eligible and screened two to seven years prior to diagnosis. The predicted reduction by changing to human papillomavirus screening was 363 (95% confidence interval = 124–496) representing 22% of all cases. If 50% of subjects not screened two to seven years prior had undergone Pap screening, it is projected that a further 268 cases (16%) could have been prevented; if they had undergone human papillomavirus screening, a further 365 cases (22%) could have been prevented.
Conclusions
For many women who develop cervical cancer, primary human papillomavirus testing could have substantially reduced their cancer risk. Human papillomavirus rather than Pap testing would further increase the gains from any increases in population screening participation.
Introduction
The most common method used to prevent cervical cancer has been the Pap test, but the test has well recognized limitations. The sensitivity of a single Pap test for the detection of cervical intraepithelial neoplasia (CIN) grade 2 or worse (CIN2+), which is widely viewed as a precursor to most squamous cervical cancer development, averages around 55%.1,2 Several studies have demonstrated that cytology is marginally effective for the prevention of adenocarcinomas,3–6 and as cytologic interpretation involves subjective assessment, performance varies substantially. 7
It is now understood that human papillomavirus (HPV) infection is a necessary precursor to the development of the vast majority of cervical cancers.8,9 This has resulted in the development and adoption of vaccines against the two principal HPV types 10 and, in some jurisdictions, the adoption of HPV testing as a screening tool.11,12 Published mathematical models permit the prediction of the effects of different strategies for vaccination and screening on the future burden of cervical cancer.13–16 Population-based reviews of the histories of cervical cancer cases provide a valuable tool for understanding the influence of various factors17–20 on the burden of disease. Information obtained from such audits facilitates the prediction of the effect of changes in environmental conditions, including a change in screening practice. 21
We present the results of an audit of the screening histories of cervical cancer cases in the Canadian Province of British Columbia (BC), and combine these with summary findings on the effects of primary HPV screening from randomized controlled trials 22 to predict the impact of the adoption of HPV screening, and of increases in screening uptake, on the number of new cervical cancer cases in BC.
Methods
Risk reduction with adoption of HPV testing
The effect of a change of primary screen from Pap smears to HPV testing is estimated using results from a combined analysis of four randomized trials comparing the impact on invasive cancer diagnosis of these two methods. 22 Data from these trials (Swedescreen, 23 POBASCAM, 24 ARTISTIC 25 and NTCC 26 ) were analyzed using a common approach, and results were compiled by study, age at screening (<30, 30–34, 35–49, and ≥50), years since enrolment (≤2.5, > 2.5), and cancer morphology (squamous and adenocarcinoma). Overall incidence of invasive cancer was reduced in the HPV arms (odds ratio (OR) = 0.60, 95% confidence interval (CI) = 0.40, 0.89). This reduction was significant for 2.5 years or more post-enrolment (OR = 0.45, 95% CI = 0.25, 0.81), but not prior (OR = 0.79, 95% CI = 0.46, 1.36). The reduction was significant for adenocarcinomas (OR = 0.31, 95% CI = 0.14, 0.69), but not for squamous cell carcinomas (OR = 0.78, 95% CI = 0.49, 1.25). No significant variation in results was found between studies, or by subject age at enrolment. 22
Risk reduction with increased participation in pap screening
We used the findings from an International Agency for Research on Cancer (IARC) report, of a risk reduction of 84% for invasive squamous cervical cancer among women aged 35–64 undergoing Pap screening every five years, 27 to estimate the effect of improved participation in Pap screening. Screening every three years is currently recommended in Canada. 28
Specification of participation
We used methods for the specification of participation29,30 for use in case-control studies of cancer preventive screening tests to identify cases that could be affected by screening. The lengths of two intervals prior to diagnosis were specified. The first, the occult invasive phase (OIP), is an interval during which invasive cancer is present but has not been diagnosed. Although screening during the OIP could benefit the patient through the detection of invasive disease at an earlier stage, it would not result in the prevention of cervical cancer. The second phase, which precedes the OIP, is the pre-invasive detectable phase (PIDP), where pre-cancerous lesions are present but have not yet developed into invasive cancer. Screening during the PIDP can lead to the prevention of cancer through the identification and successful treatment of a precursor lesion. The OIP and PIDP are assumed to vary between individual cases.
Analyses of time between a negative cytology and development of invasive squamous cervical cancer from service screening indicate protection up to five to seven years.5,27 A joint analysis of seven European cohort studies involving more than 24,000 women indicated that the risk of CIN3 + at three years following a negative cytology exceeded that at five years following a negative HPV test. 31 The time from negative screening test until invasive cancer diagnosis will overestimate the average PIDP, as this interval will also include the period when invasive cancer was present, but occult. 23 Direct estimation of the average OIP in individual cases is not possible, and model estimates have mean values typically around two to three years. 32 The summary of four European randomized trials 22 found reductions in cervical cancers, but little difference between HPV and cytology arms in the first two years, indicating that it is primarily pre-existing cancer which is being diagnosed in this period. Consequently, the OIP will be chosen to be two years. Rescreening intervals for HPV tests are commonly set at five years or longer.33,34 This period will be smaller than the average PIDP so that a high proportion of cancers can be prevented if the recommendation is followed, 31 so a value of five years for the average PIDP represents a conservative choice. The net result of these considerations is that screening utilization within the three-year period, two to seven years prior to the diagnosis of invasive cancer, is an appropriate choice for the PIDP. The results from the joint analysis of the four trials for >2.5 years after entry are used as the estimate of the relative effect of HPV versus cytology screening within the PIDP.
Age limits for screening
There is uncertainty regarding the efficacy of screening women between the ages of 21 and 29,19,35 and Canadian recommendations indicate that Pap screening should start at age 25. 28 It is generally considered that HPV is not a suitable screening test in younger women because of the high prevalence rate of HPV infection of limited clinical significance, 36 resulting in recommendations to begin screening with HPV at age 30 or 35. We selected age 30 as the lower cut-off for use of HPV as a screening test, with any screening under age 30 assumed to continue as before (i.e. using cytology). Current Canadian recommendations specify that screening can end at age 69, if the last three screens performed prior to this age were negative and were performed within a 10-year period. 28 Women with a history of significant pathologically proven abnormality (CIN2+) are recommended to continue screening. We used this specification to classify cases after age 69.
Study data
Cases of invasive cervical cancer occurring in BC between 1 January 2002 and 31 December 2011 were identified from the population-based BC Cancer Registry (BCCR), and disease and identifying data extracted. Screening is provided through a centralized screening laboratory affiliated to the BC Cancer Agency, which houses the BCCR. The screening program estimates that 70.2% of eligible women aged 20–69 have been screened in the previous three years. 37 Screening histories were identified from the BC cervical cancer screening program (CCSP) database. The CCSP database contains records of all screens after 1986 interpreted at the cervical cytology laboratory, which is the sole provider of gynecologic cytology interpretation within the BC public medical plan. Information extracted included dates and results of examinations performed prior to the date of diagnosis. Cancer cases were classified by their age at diagnosis, cancer morphology, and history of cytologic screening.
Statistical considerations
To predict the impact of use of HPV rather than Pap testing, we applied the risk reductions found in the published analysis 22 to the appropriate subgroups, as identified within the audit of cancer cases. Grouping was based on the published breakdowns. 22 CIs for projections were based on the published CIs for risk reduction 22 and the sampling variation of the study population.
In predicting the effect of increases in participation, we assumed that the number of cases in women with eligible cancers arising outside the PIDP was reduced proportionately, and these women would now be screened within the PIDP. For increased participation in Pap screening, only squamous cancers were eligible, and the risk ratio from the IARC report 27 was applied (13%) to the number of cancers that would still occur after increased participation. For increased participation in HPV screening, the same approach was used, and both squamous and non-squamous cancers were included. For squamous cancers, the rate-ratio was that for Pap 27 multiplied by the corresponding estimated relative reduction for HPV versus Pap. 22 For non-squamous cancers, the HPV versus Pap ratio alone was used. 22 Canada has no official target for cervical screening participation, so for the purposes of illustration we assumed a large effect: that the rate of inadequate compliance (not screened in the PIDP) would be halved. Participation is currently measured in the population using a three-year window, and this does not easily translate into the PIDP as defined in this paper. However, if the ratio were the same, this would correspond to an increase from 70.4% to 85.2% population participation every three years among eligible BC women.
This research was approved by Research Ethics Board of the University of British Columbia, certificate number H06-04032.
Results
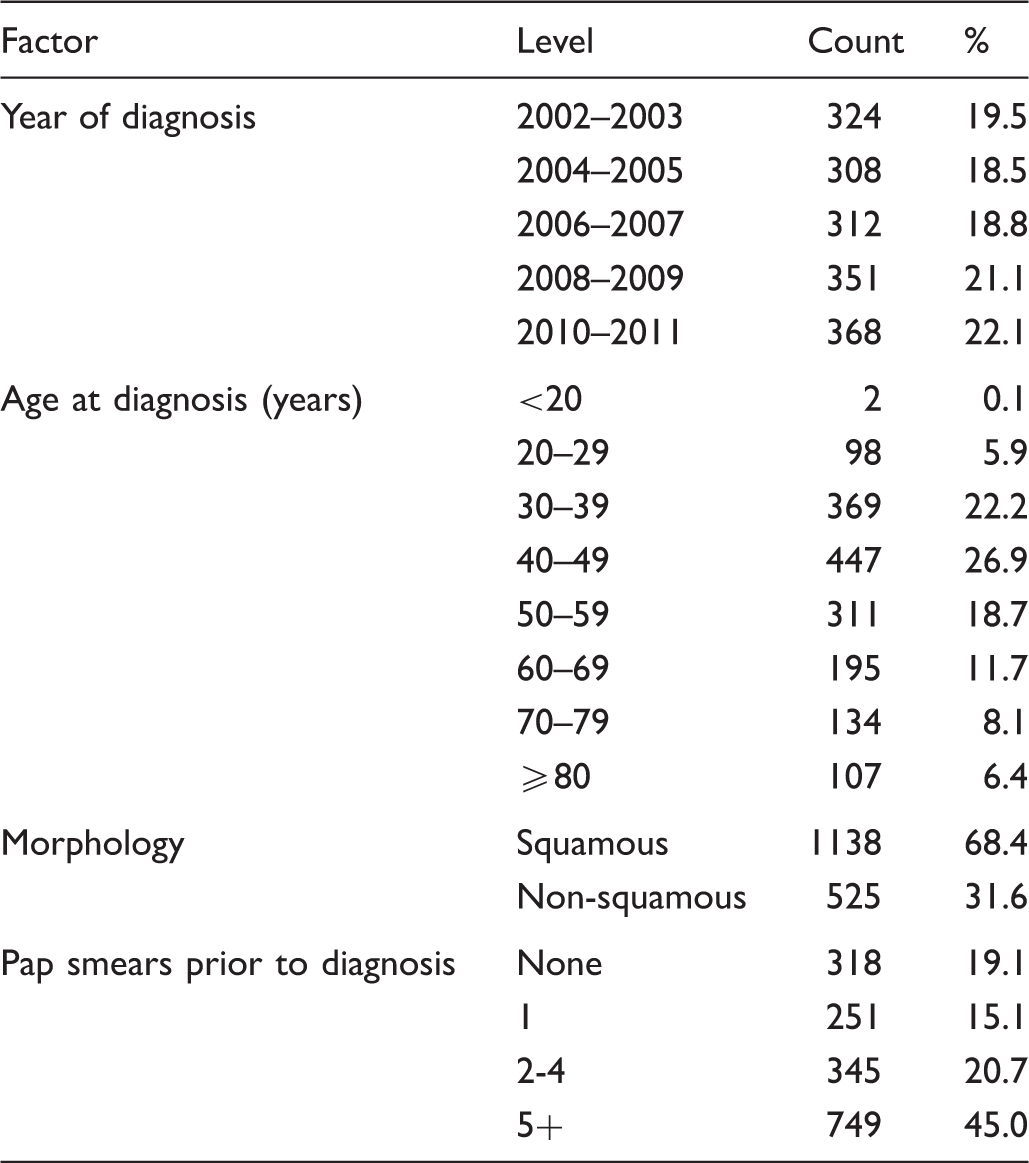
Distribution of invasive cervical cancers diagnosed in British Columbia in 2002–2011 by year of diagnosis, age, morphology, and number of pap smears prior to diagnosis.
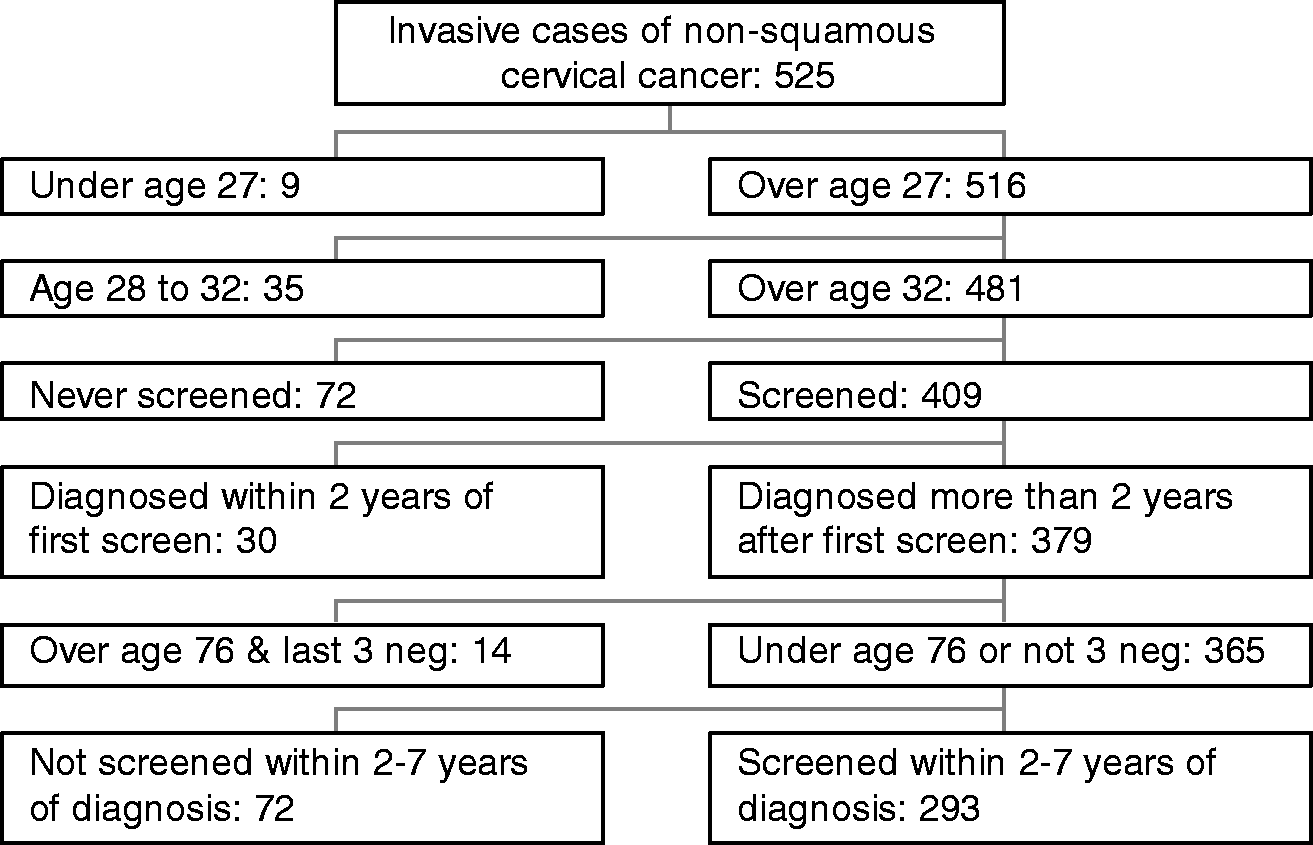
The classification of cervical cancer cases seen in the study population is given separately for squamous (Figure 1) and non-squamous (Figure 2). There were 811 cases, 637 squamous and 174 non-squamous, over age 32 and eligible for screening, in women who had not participated in screening in the PIDP (two to seven years prior to diagnosis).
Schema of invasive squamous cervical cancer cases diagnosed 2002–2011 in British Columbia by age and screening history. Schema of invasive non-squamous cervical cancer cases diagnosed 2002–2011 in British Columbia by age and screening history.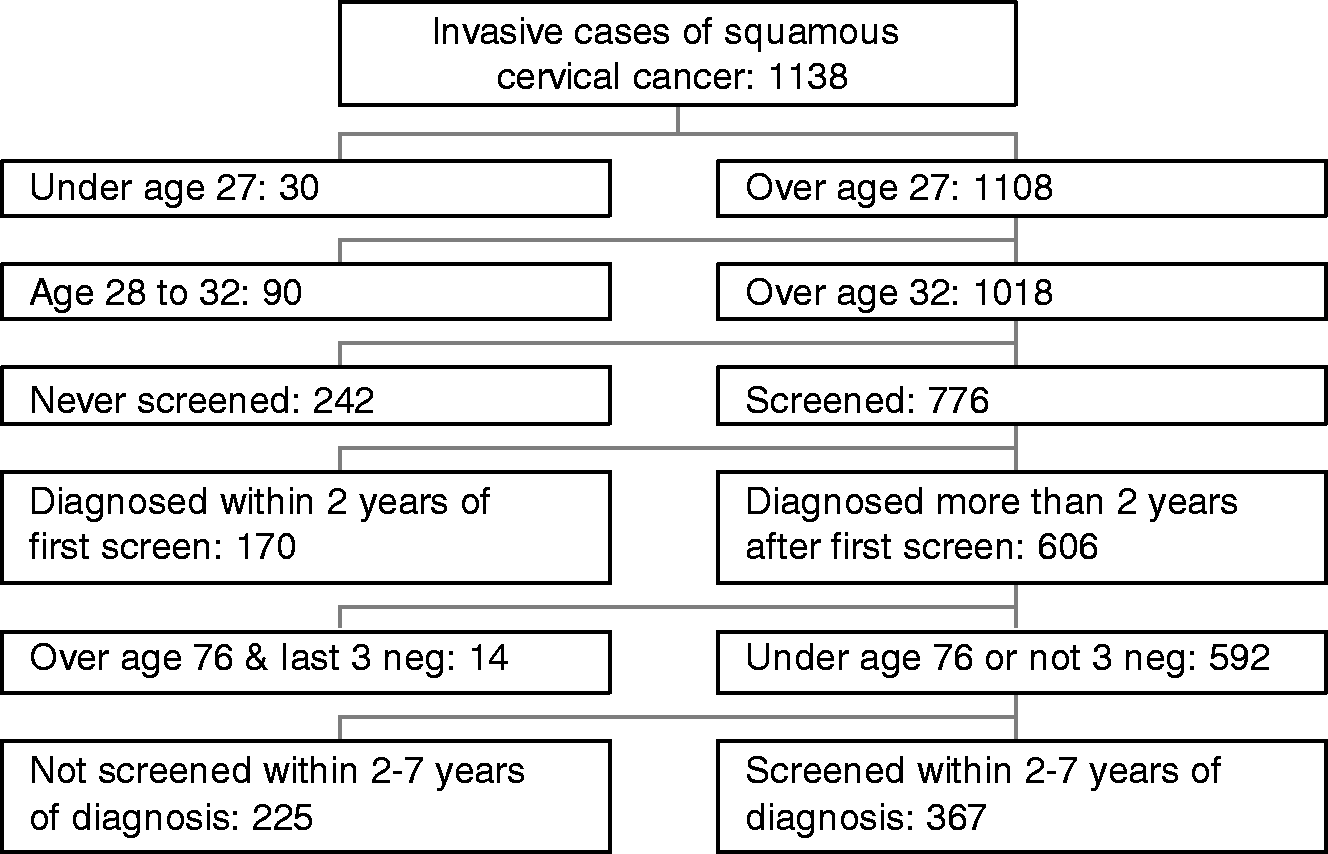
Number of cases eligible, odds ratios and estimated potential reductions in cervical cancer burden for the study data.
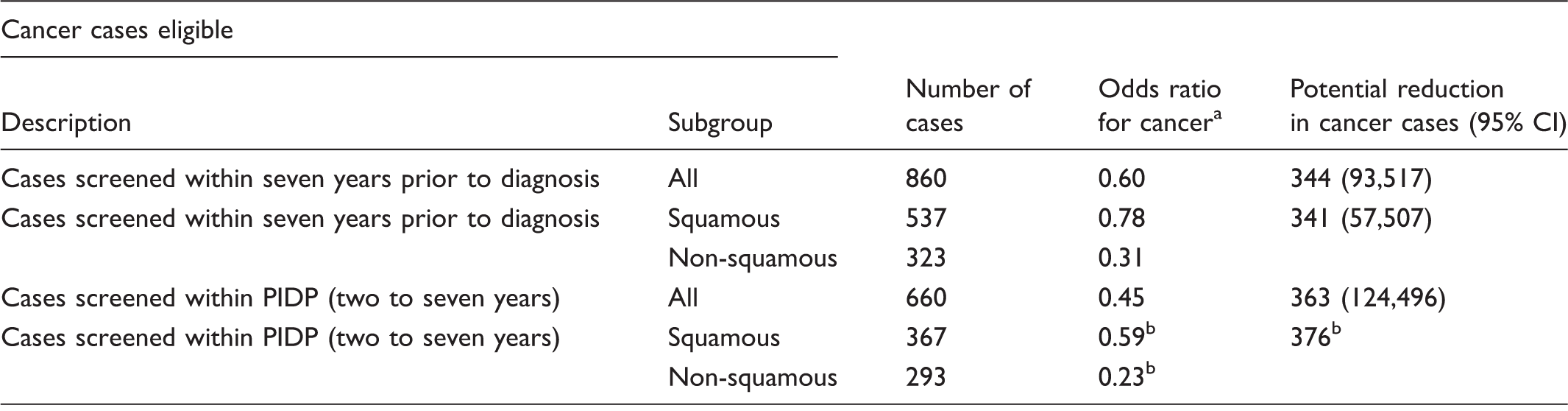
Ronco et al. 22
Ronco et al. 22 and assuming independence in effect between effect of time since screening and tumor morphology. Confidence interval was not available.
Increased participation in Pap screening, which reduced the number of eligible women not being screened within the PIDP, would potentially influence 637 (242 + 170 + 225) squamous cancers (Figure 1). If half of these women had been screened within the PIDP, we would estimate that 268 (637 × 0.5×.84) of these cases would have been potentially prevented, which represents 16% of all cases. A similar level of increased participation with HPV screening would result in a projected reduction of 298 squamous (637 × 0.5 × [1 − (1 − .84) × (1 − 0.59)]) (Figure 1 and Table 2) and 67 non-squamous (174 × 0.5 × [1 − 0.23]) (Figure 2 and Table 2) cases, a total of 365, which represents 22% of all cases.
It has been projected that in 2015 1500 cases of cervical cancer will exist in Canada. 38 If the same proportional reductions associated with use of HPV and no change in participation estimated for BC could also be realized in Canada, this would correspond to predicted annual reductions between 287 and 339 cases. For increased Pap participation, the corresponding estimate is 240 cases (16%), and for increased HPV participation, it is 330 cases (22%).
Discussion
The audit of invasive cervical cancer cases diagnosed in BC between 2002 and 2011 revealed that 660 cases (39.7%) had been screened at a time when screening with HPV could have reduced the women's risk of developing cervical cancer (PIDP). It was estimated that use of the HPV test in place of the conventional Pap smear, with no change in participation, would have resulted in a reduction of 363 cervical cancers (22%) (95% CI 124–496) over the study period, with over 60% of these cases being of non-squamous morphology. Changing the criteria of those potentially affected resulted in slightly different estimates, and the percentage potentially prevented is between 21% and 23% of all cases. It was estimated that increasing Pap screening participation so that the rate of non-participation was halved, with no change in screening test, would result in a reduction of 268 cases (16%). The same increased participation with HPV testing would result in an estimated reduction of 365 cases (22%).
A study from England 21 projected that a switch to HPV testing could result in a maximum 32.6% reduction in cases currently being screened. The basis of this calculation is somewhat different from the one presented here, in that it draws on a case-control study of screening and the observed increased sensitivity of HPV testing for the identification of CIN2+. The study assumes a best-case scenario, where precursor identification in cancer cases would have resulted in prevention of invasive cancer. Also, higher screening participation rates in England 39 imply that the result of improvements in the screening test will be proportionately higher.
A limitation of this study is that it relies on evidence from randomized trials conducted in other jurisdictions to project reductions in cancer development associated with a change in screening test in Canada. Subject compliance with recommended follow-up may differ between randomized trials and routine practice. Although HPV testing has been demonstrated to display consistent sensitivity for CIN2+, 1 cytology has not, 7 so that cancer reductions brought about by a change to HPV testing may vary depending on actual cytology performance. The sensitivity of cytology in BC has been estimated to be around 75%, 40 which is similar to that reported for England, 1 the location of one of the participating trials. Trials compared cytology with HPV screening, using the same frequency of testing. If the frequency of testing is reduced when HPV is used (every five years), compared with that used for Pap, it can be anticipated to diminish its relative effectiveness to that when used at the same frequency, although it should still be expected to be superior to cytology based on its better negative predictive value. 30 The impact of HPV screening beyond seven years after initiation was not available from the trials, but as its superiority results from the increased ability to identify precursor lesions, there is no reason to think that it would not continue to be more effective. Increasing participation in screening has proven challenging in BC, and in Canada generally, with current rates approximately 70% little changed over the last five years 37 despite efforts to increase them. A 50% reduction in effective non-participation would require a major change in population behavior.
Monte-Carlo simulation studies have been conducted on the effect of potential misspecification of the length of the pre-clinical detectable phase in case-control studies where mortality, not incidence, of cancer is the outcome. These studies have concluded that under-specification of the interval length results in greater bias than over-specification, 41 and that bias generally results in the underestimation of screening efficacy.
The success of gynecologic cytology in controlling cervical cancer has resulted in an understandable caution when considering its replacement. Current evidence suggests that there are substantial benefits in switching to HPV testing. Used appropriately, with triage of HPV cases with cytology, or other approaches, HPV testing results in no sustained increase in referral to colposcopy in women aged over 30. 42 HPV testing also offers the potential to increase effective participation in screening, both through the extension of the screening interval, and the potential use of self-collection in those not currently participating in screening. 43 Ongoing deployment of HPV vaccines can be expected to bring about further reductions in cervical cancer; however, there will be a continuing need for screening, as women already infected will continue to be part of the population for many years. In this environment, cytology screening will be less appropriate and more technically challenging, 44 and there seems a substantial case for the replacement of the Pap test with one based on HPV.
Footnotes
Acknowledgements
The authors thank Norm Phillips who conducted the statistical analysis contained in this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research materials
Research data contained in this report can be obtained from the corresponding author.