
Abstract
Objective
England has universal screening for sickle cell disease in newborns, with a policy of reporting beta thalassaemia major where it is detected. We report a case with a high gamma/beta ratio (20.167), but all other tandem mass spectrometry results within expected normal limits. The second test did not support the presumed diagnosis of beta thalassaemia major. As the two results were discrepant, further investigations were carried out.
Methods and results
Sanger sequencing identified a novel mutation HBB:c.40 G > A (Hb Tower Hamlets) with concomitant beta plus (severe) thalassaemia due to the HBB:c.92 + 5 G > C mutation.
Conclusions
This case highlights considerations for policy makers and implementers of new methods in screening programmes. For the English screening programme, the importance of adherence to the two-part testing strategy for newborn haemoglobinopathy screening is demonstrated. When discrepancies occur in results between the two tests, a thorough investigation is indicated. Communication, training, incident review and oversight are vital aspects of any screening programme. Protocols, risk assessments and guidance require constant monitoring and review to ensure that they remain fit for purpose. When new methods are introduced, stringent application of these principles is recommended.
Introduction
In the English programme of universal screening for sickle cell disease in newborns, the policy is to report beta thalassaemia major where it is detected. Following a 2012–2013 pilot study, tandem mass spectrometry (MSMS) was approved for use as a screening technique, and now comprises the initial screen for almost 50% of the 680,000 births tested annually. In brief, globin peptide fragments are generated by digestion with trypsin; these are subsequently analysed by targeted MSMS experiments for specific haemoglobins. 1 Using this technique, results are reported as a ratio of peptide under investigation against corresponding wild-type beta peptide signal. A high gamma/beta ratio in a full-term infant suggests beta thalassaemia major.
Methods and results
We report a case where a high gamma/beta ratio (20.167) was obtained on the initial screen of a female infant, gestation 39 + 6 weight 3540 g. All other MSMS results were within expected normal limits (see Table 1). In accordance with the screening policy, a second test with a different principle was performed. This showed a normal pattern of Hb F and Hb A (on iso-electric focussing (IEF)) which did not support the presumed diagnosis from the initial screen of beta thalassaemia major. As the two results were discrepant, further investigations were carried out, initially high-performance liquid chromatography (HPLC), which also gave a normal pattern with Hb A 11.9%, the remainder being Hb F.
Results for MSMS experiments with recommended action values.
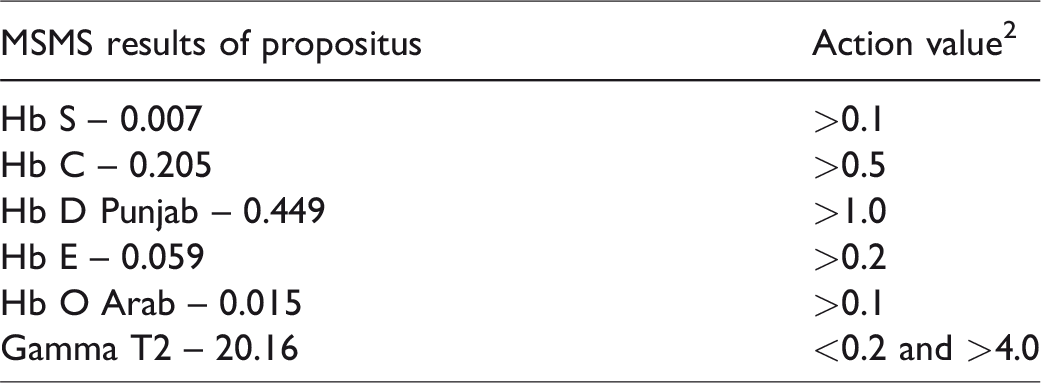
As part of the on-going assessment of discrepant cases, Sanger sequencing was carried out, and a novel mutation HBB:c.40 G > A (Hb Tower Hamlets) with concomitant beta plus (severe) thalassaemia due to the HBB:c.92 + 5 G > C mutation was identified. This novel variant results in an alanine to threonine substitution at position 13 of the beta globin chain located in the beta T2 peptide. The Ala>Thr substitution creates an alternate beta T2 peptide with a +30 Dalton mass difference from wild type, thus reducing the observed beta T2 signal for the experiment. The HBB:c.92 + 5 G > C mutation further reduces the wild-type signal due to the significantly reduced synthesis of the beta globin chain from this allele. The two events combine to generate an observed gamma T2/beta T2 ratio above the action value for beta thalassaemia major.
Discussion
MSMS has recently been included as an acceptable technique in English laboratories performing newborn screening for sickle cell disease. Policy states that positive samples identified in the first test (here MSMS) must have a second confirmatory test using a different principle (IEF, HPLC or capillary electrophoresis (CE)), and that discrepancies should be appropriately investigated. 3 For IEF and HPLC, which have been in use for over 30 years, there is a significant body of evidence and expertise available. However, this level of expertise in MSMS has not yet been reached, and during implementation, there has been a tendency for the results from familiar techniques to be favoured above MSMS. A thorough review of discrepant cases will add to the body of knowledge available.
Communication, training, incident review and oversight are vital aspects of any screening programme. Protocols, risk assessments and guidance require constant monitoring and review to ensure that they remain fit for purpose. The NHS Sickle Cell & Thalassaemia Screening Programme is working closely with laboratories implementing MSMS to ensure that the guidance, action values, training and knowledge base are appropriate. In the six years following the initial pilot study, action values for the common conditions have been refined but remain under review. 2 Current work streams focus on rarer cases and include review of the ratios obtained when there is co-inheritance of haemoglobin variants with beta thalassaemia. The reported case was potentially a false positive for beta thalassaemia major. The reporting laboratory recognized and followed up the anomaly between MSMS and the second tests, but relied on the more familiar techniques of IEF and HPLC for the initial report. Molecular diagnosis was carried out as part of the ongoing evaluation of the action values and review of discrepancies. Our ongoing review has also identified a case where reliance on a familiar technique, IEF, resulted in a clinically significant compound heterozygous S/beta plus thalassaemia being reported as a sickle carrier. These cases demonstrate the importance of the two-part testing strategy in England and the complexities of screening for these disorders. The cases also highlight the value of molecular testing to resolve discrepancies identified in the two-part test. When used as recommended, the two-test strategy improves specificity of the screening test, which in turn limits unnecessary referral into clinical pathways, and reduces clinically anomalous cases and the potential anxiety faced by families.
Conclusion
This case of Hb Tower Hamlets co-inherited with beta thalassaemia highlights important principles to be considered by policy makers when implementing new screening strategies, and good practice for existing screening programmes.
Footnotes
Acknowledgements
We thank Deborah Mantio and Laura Fraser The Doctors Laboratory, Central Middlesex Hospital, Tejswurree Ramgoolam Newborn Screening Laboratory, Great Ormond Street Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.