
Abstract
Upper and lower truncation limits are commonly applied to quantitative markers used in medical screening tests. We here examine data on 375 trisomy 18 and 522,081 unaffected singleton pregnancies, to determine if the lower truncation limit should be set below the previously specified 0.2 multiples of the median. A lower truncation limit of 0.15 would reduce the underestimation of the risk of having a trisomy 18 pregnancy in about 50% of affected pregnancies and would lead to an estimated 10 percentage point increase in the detection rate, with only a very small increase in the false-positive rate.
Keywords
Upper and lower truncation limits are commonly applied to quantitative markers used in medical screening tests, to avoid extreme values having a large and unwanted impact on an individual’s estimated risk of being affected by the disorder for which screening is being performed.
1
If the screening marker value is higher (or lower) than the specified upper (or lower) truncation limit, the limit is used in risk estimation. The truncation limits are set using data on affected and unaffected pregnancies. There are several ways in which these limits are set: when screening marker values deviate from the Gaussian distributions used in calculating risk (usually determined by inspection of probability plots of the marker values), when in the tails of the distributions there are too few data for a likelihood ratio to be reliably calculated at the value of the marker, or when the likelihood ratio ceases to increase or decrease with more extreme values of the marker.1,2 In antenatal screening for trisomy 18 using the Combined test (nuchal translucency, free β-human chorionic gonadotrophin, and pregnancy-associated plasma protein-A (PAPP-A) with maternal age at 11–13 weeks’ gestation), the lower truncation limit for PAPP-A that we previously specified (0.2 multiples of the median (MoM))
3
may be too high, so that affected pregnancies might be missed. We here examine data on 375 trisomy 18 and 522,081 unaffected singleton pregnancies screened at the Wolfson Institute of Preventive Medicine between January 2000 and August 2016, to determine if the lower truncation limit could be moved below 0.2 MoM. Figure 1 shows the probability plots of the PAPP-A MoM values in affected and unaffected pregnancies. The MoM values in unaffected pregnancies start to deviate from the Gaussian distribution below the previously suggested lower truncation limit of 0.2,
2
but the deviation is not marked until the MoM values drop below about 0.1. About 50% of trisomy 18 pregnancies have a PAPP-A MoM value of 0.2 or less, and about 35% have a MoM value of 0.15 or less. A lower truncation limit of 0.15 would reduce the underestimation of the risk of having a trisomy 18 pregnancy in about 50% of affected pregnancies (the likelihood ratio for PAPP-A increases from 38 at 0.2 MoM to 181 at 0.15 MoM based on previously published means and standard deviations of the log MoM values in trisomy 18 (−0.7959 ± 0.3209) and unaffected (0 ± 0.2495) pregnancies
3
) and would lead to an increase in the detection rate with only a very small increase in the false-positive rate. For example, using previously described modelling methods,
3
at a 1 in 150 term risk cut-off using the Combined test, the detection rate increases from 70% to 80% and the false-positive rate from 0.05% to 0.06%.
Probability plots of pregnancy-associated plasma protein-A multiple of the median (MoM) values in trisomy 18 and unaffected pregnancies.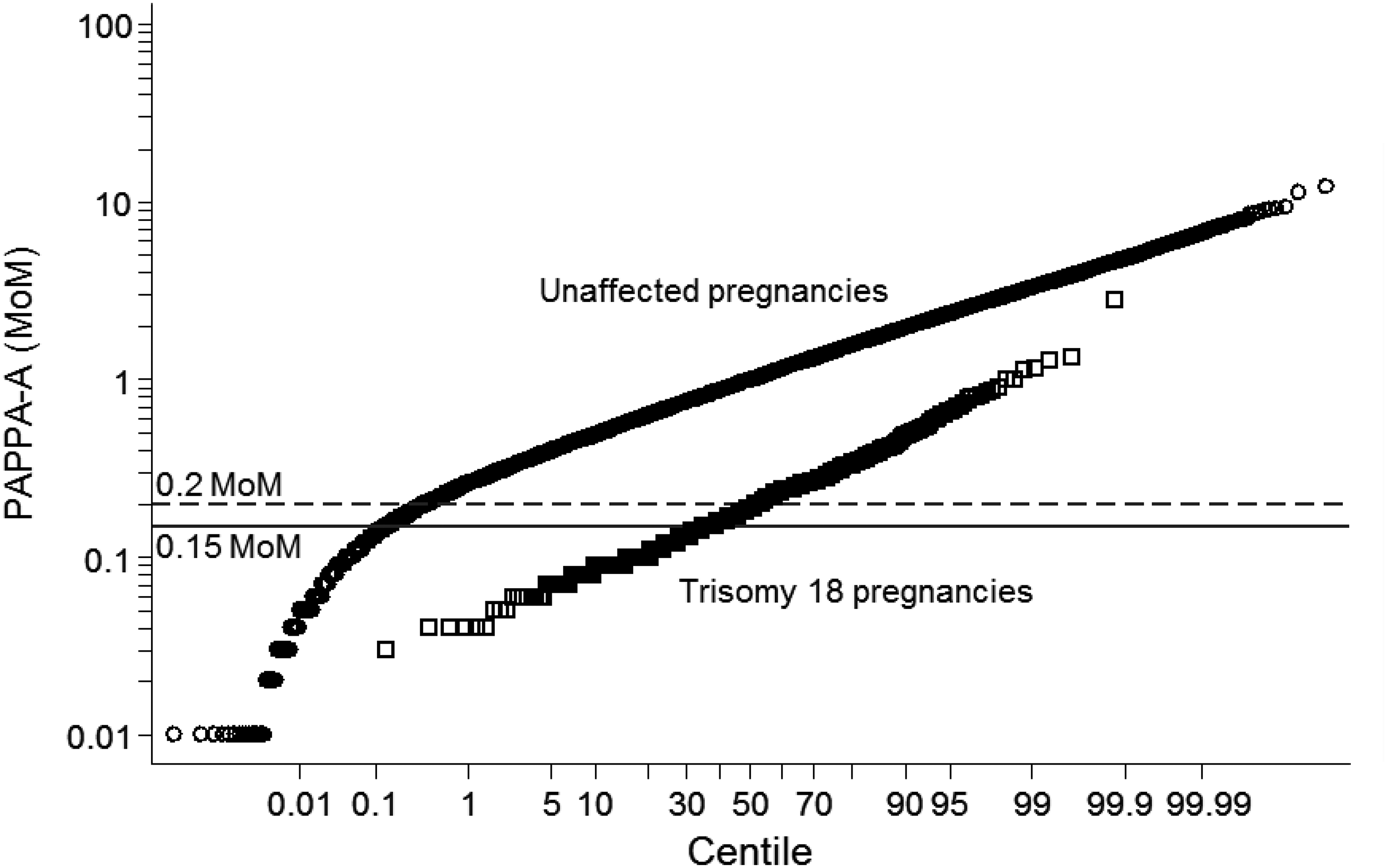
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nicholas Wald is the Director of Logical Medical Systems Ltd, which produces software for the interpretation of Down’s syndrome screening tests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.