
Abstract
Objective
To estimate the performance of antenatal sequential Integrated screening for Down’s syndrome (DS), trisomy 18 (T18) and trisomy 13 (T13), in which women have first trimester testing for each disorder; those above specified risk cut-offs are screen-positive, and the remainder continue to Integrated testing, using first and second trimester screening markers together.
Methods
Published screening marker parameters and Monte Carlo simulation were used to calculate detection rates (DR’s) and risk cut-off levels for specified false-positive rates (FPR’s), and DR’s and FPR’s for specified risk cut-offs. We compared this screening performance with that based on all women having Integrated tests.
Results
Sequential Integrated DS screening detects 71% of DS pregnancies at the first trimester stage at a 0.5% FPR. For an overall 2% FPR, the DS DR is 92%, the same screening performance as the Integrated test performed on all women. Sequential Integrated T18 and T13 screening detects 70% of T18 and 53% of T13 pregnancies at the first trimester stage at a 0.05% FPR for each. The overall T18 and T13 DR’s are 96% and 72% respectively at 0.2% FPR, the same screening performance as with Integrated tests performed on all women. Increasing the overall FPR’s does not materially increase the DR’s for any of the three disorders.
Conclusion
The performance of sequential Integrated screening is similar to the performance if all women have an Integrated test, but has the advantage of identifying most DS, T18, and T13 pregnancies a few weeks earlier.
Keywords
Introduction
Down’s syndrome, trisomy 18, and trisomy 13 are the most common viable autosomal trisomies, with birth prevalences of 19.4, 2.3, and 1.4 per 10,000 respectively in the absence of screening and selective abortion. 1 In 2006 we estimated the screening performance of sequential Integrated screening for Down’s syndrome. 2 We here provide updated screening performance estimates based on the Serum, Urine and Ultrasound Screening Study (SURUSS) screening marker parameters, 3 revised in light of new data, 4 and include screening performance estimates of sequential Integrated screening for trisomy 18 and trisomy 13.
In sequential Integrated screening, women with a positive first trimester (11–13 weeks’ gestation) screening test result are offered a diagnostic test (amniocentesis or chorionic villus sampling), and the remaining women continue to a second trimester (14–22 weeks’ gestation) Integrated test, which reuses the first trimester screening markers together with second trimester markers. Women with positive Integrated test results are offered a diagnostic test. Provided the first trimester test false-positive rate is low (for example 0.5% or lower) and, hence, the risk cut-off high (for example 1 in 50 or higher), sequential Integrated screening for Down’s syndrome can achieve the same detection rate for only a marginally higher false-positive rate than that achieved if all women have an Integrated test. For sequential Integrated screening for Down’s syndrome, we previously estimated that at a 90% detection rate the false-positive rate was 2.25% compared with 2.10% if all women have an Integrated test. 2
Methods
Monte Carlo simulation was used to draw samples of 1,000,000 pregnancies with Down’s syndrome, 1,000,000 with trisomy 18, 1,000,000 with trisomy 13, and 1,000,000 unaffected pregnancies from the multivariate Gaussian distributions of the log10 transformed multiple of the median values for three first-trimester markers (nuchal translucency [NT], free β-human chorionic gonadotrophin [hCG] and pregnancy associated plasma protein-A [PAPP-A]), and four second-trimester markers (alphafetoprotein [AFP], unconjugated estriol [uE3], free β-hCG, and inhibin-A). The multivariate distribution of the markers in Down’s syndrome and unaffected pregnancies was estimated using the parameters (means, standard deviations, correlation coefficients, and truncation limits) from the Serum Urine and Ultrasound Screening Study (SURUSS) 3 (with update 4 ), and in trisomy 18 and trisomy 13 from published data from the Wolfson Institute of Preventive Medicine Antenatal Screening Service. 5 In screening for trisomy 18 and trisomy 13, for unaffected pregnancies the 11 week estimate of the standard deviation of NT was used. 4 Each simulated pregnancy was assigned a maternal age based on the distribution of maternities in England and Wales 2006–2008 6 and the maternal age-specific odds of a livebirth affected with Down’s syndrome, 7 trisomy 18, or trisomy 13. 1 For each simulated pregnancy, and for each disorder, an early second trimester maternal age risk was calculated by multiplying the maternal age specific odds of having an affected live birth by 1/0.77 for Down’s syndrome, 8 1/0.35 for trisomy 18, and 1/0.58 for trisomy 13 9 to allow for the general fetal loss in affected pregnancies from this time in pregnancy until term. The predicted risks of Down’s syndrome, trisomy 18, and trisomy 13 were calculated by multiplying the age specific odds by the likelihood ratios obtained from the overlapping multivariate Gaussian distributions of marker levels (second trimester inhibin-A not used to estimate trisomy 18 pregnancy risk, and second trimester AFP, uE3, and hCG not used to estimate trisomy 13 pregnancy risk) in affected and unaffected pregnancies (calculated using total or free β-hCG in either the first or second trimester).
Detection rates for sequential Integrated screening were determined by setting the first trimester test Down’s syndrome false-positive rate at 0.25, 0.5, 0.75, or 1%, and the overall Down’s syndrome false-positive rate at 1, 2, 3, 4, and 5%, and setting the first trimester trisomy 18 and trisomy 13 false-positive rates at 0.025, 0.05, 0.075, or 0.1%, and the overall trisomy 18 and trisomy 13 false-positive rates at 0.1, 0.2, 0.3, 0.4, or 0.5%, and these were compared with the detection rates for all women having an Integrated test for each disorder (free β-hCG used in the second but not the first trimester for Down’s syndrome screening because free β-hCG discriminates better between Down’s syndrome and unaffected pregnancies in the second trimester, 3 vice versa for trisomy 18 and trisomy 13 screening 5 ), for the same overall false-positive rates. Similarly, detection and false-positive rates were calculated by setting risk cut-offs (this was done for early second trimester risks of an affected pregnancy, and for term risks of an affected pregnancy). We also estimated screening performance with the use of total hCG instead of free β-hCG, with distribution parameters for total hCG in trisomy 18 and trisomy 13 pregnancies taken from other sources: first trimester trisomy 18 mean, standard deviation, truncation limits, and correlation with PAPP-A from Palomaki et al. (2004), 10 second trimester trisomy 18 mean, standard deviation, and correlation with uE3 from Hackshaw et al. (1995), 11 truncation limits from Palomaki et al. (1995) 12 and correlation with AFP from Hackshaw et al. (2000); 13 first trimester trisomy 13 mean and standard deviation from Spencer et al. (2000), 14 and truncation limits based on inspection of a probability plot constructed from data extracted from Figure 2 of Spencer et al. (2000) 14 and the point of risk reversal 15 (limits 0.30 to 1.42). In both trisomy 18 and trisomy 13 pregnancies the correlation between NT and first trimester total hCG was taken to be the same as the correlation between NT and free β-hCG, and in trisomy 13 pregnancies the correlation between first trimester total hCG and PAPP-A was taken to be the same as the correlation between free β-hCG and PAPP-A.
Results
Performance of Integrated and sequential Integrated screening for Down’s syndrome according to false-positive rates and whether free β-hCG is used in the first, second, or both trimesters. Table based on early second trimester Down’s syndrome risks.
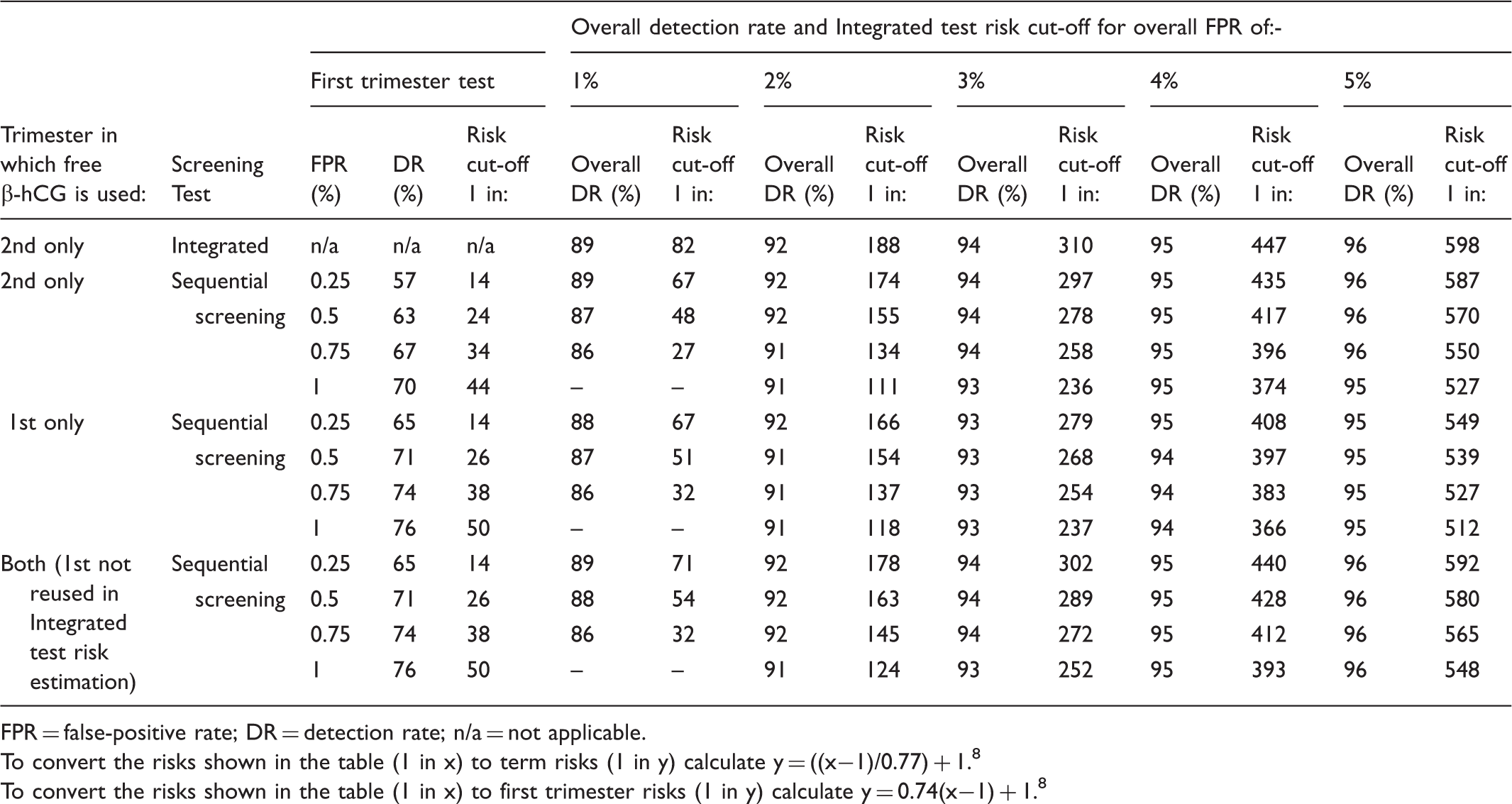
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.77) + 1. 8
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.74(x−1) + 1. 8
With free β-hCG used in the first (but not the second) trimester, at the same first trimester and overall false-positive rates, sequential Integrated screening detects 71% of Down’s syndrome pregnancies in the first trimester, and 91% overall. With free β-hCG used in both the first and second trimesters (but the first measurement not reused in estimating an Integrated test risk), at the same first trimester and overall false-positive rates, sequential Integrated screening detects 71% of Down’s syndrome pregnancies in the first trimester, and 92% overall. The Table shows that there is no material increase in the detection rate from increasing the overall false-positive rate beyond 2%. For example, in sequential Integrated screening, with a first trimester test false-positive rate of 0.5%, doubling the overall false-positive rate from 2% to 4% adds only three percentage points to the overall Down’s syndrome detection rate.
Performance of Integrated and sequential Integrated screening for Down’s syndrome according to risk cut-off levels and whether free β-hCG is used in the first, second, or both trimesters. Table based on early second trimester Down’s syndrome risks.
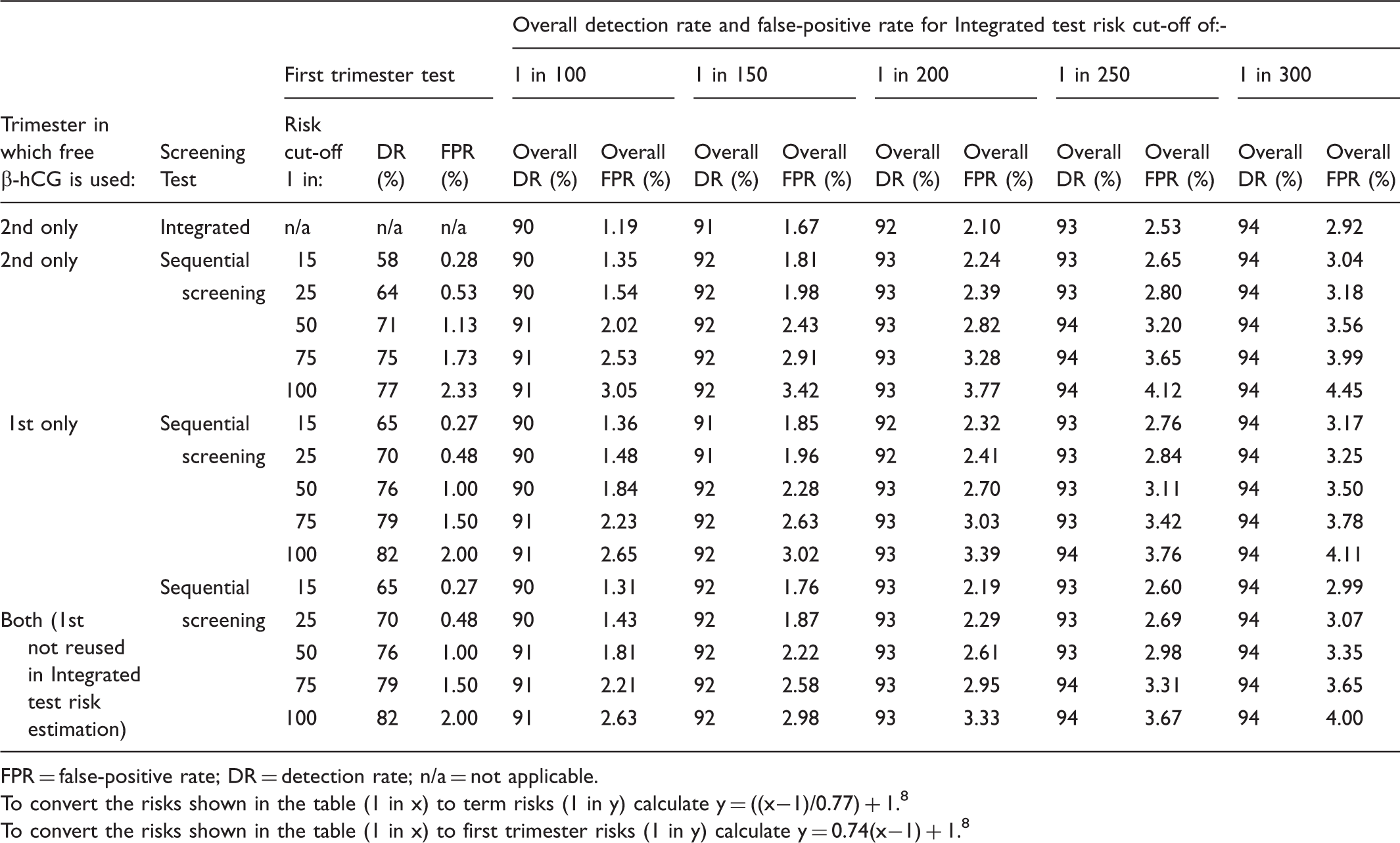
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.77) + 1. 8
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.74(x−1) + 1. 8
Performance of Integrated and sequential Integrated screening for trisomy 18 according to false-positive rates and whether free β-hCG is used in the first or second trimester. Table based on early second trimester trisomy 18 risks.
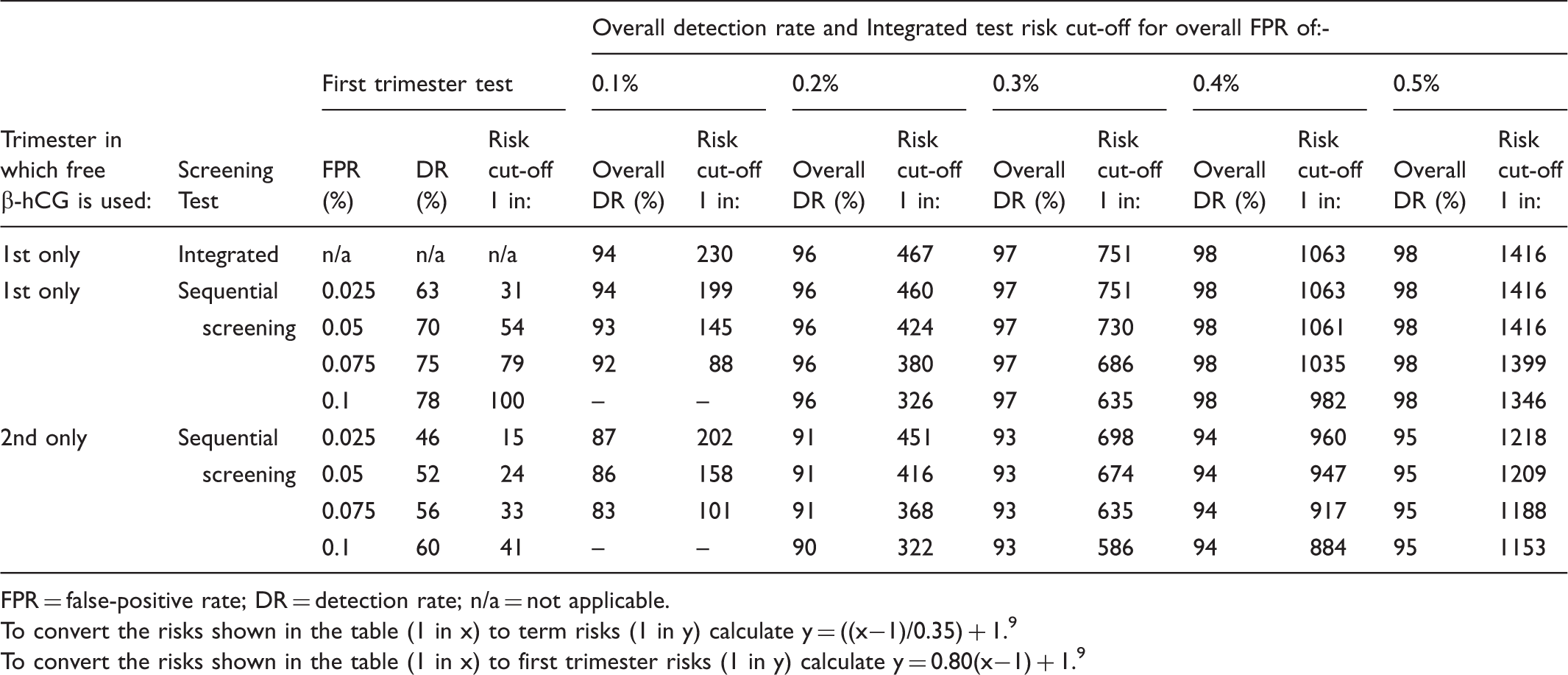
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.35) + 1. 9
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.80(x−1) + 1. 9
With free β-hCG used in the second (but not the first) trimester, at the same first trimester and overall false-positive rates, sequential Integrated screening detects 52% of trisomy 18 pregnancies in the first trimester, and 91% overall. As with sequential Integrated screening for Down’s syndrome, the Table shows that there is no material increase in the detection rate from increasing the overall false-positive rate.
Performance of Integrated and sequential Integrated screening for trisomy 18 according to risk cut-off levels and whether free β-hCG is used in the first or second trimester. Table based on early second trimester trisomy 18 risks.
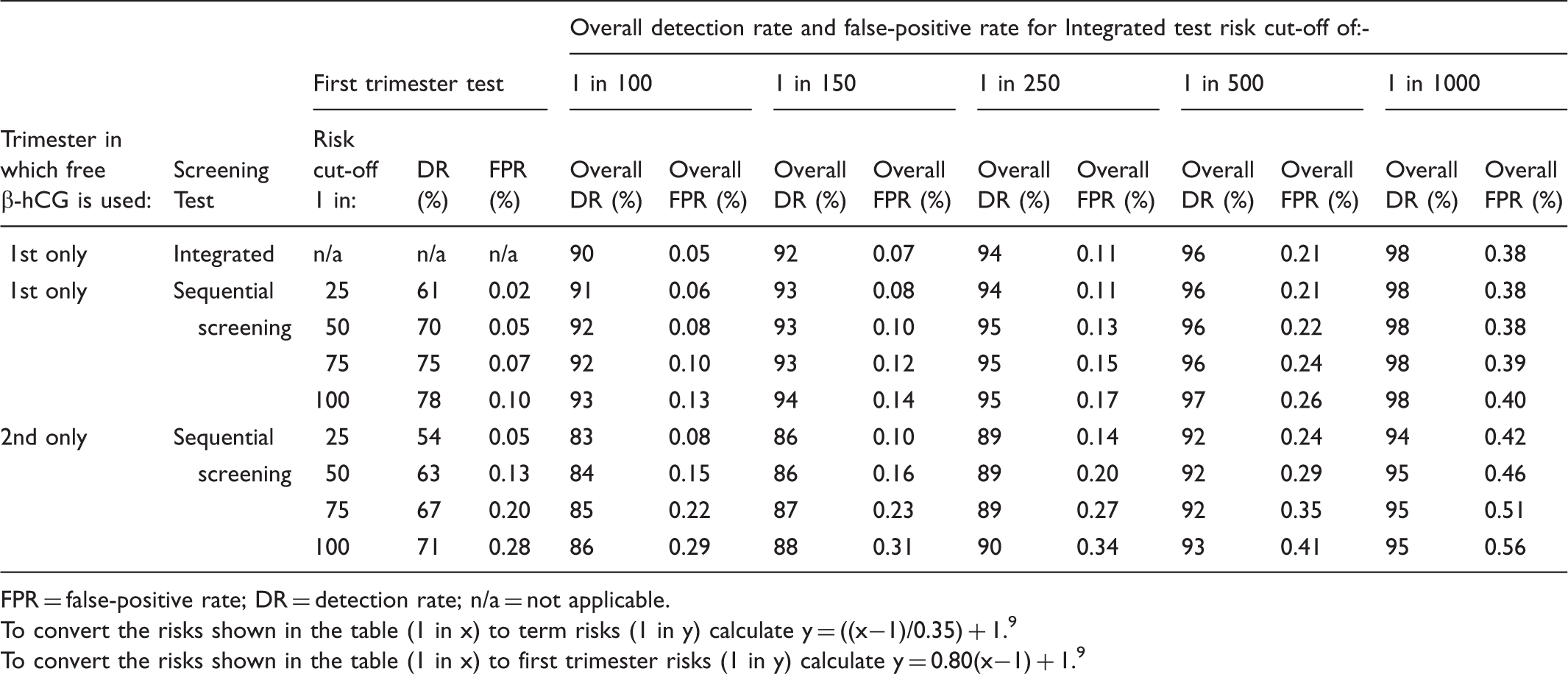
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.35) + 1. 9
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.80(x−1) + 1. 9
Performance of Integrated and sequential Integrated screening for trisomy 13 according to false-positive rates and whether free β-hCG is used in the first or second trimester. Table based on early second trimester trisomy 13 risks.
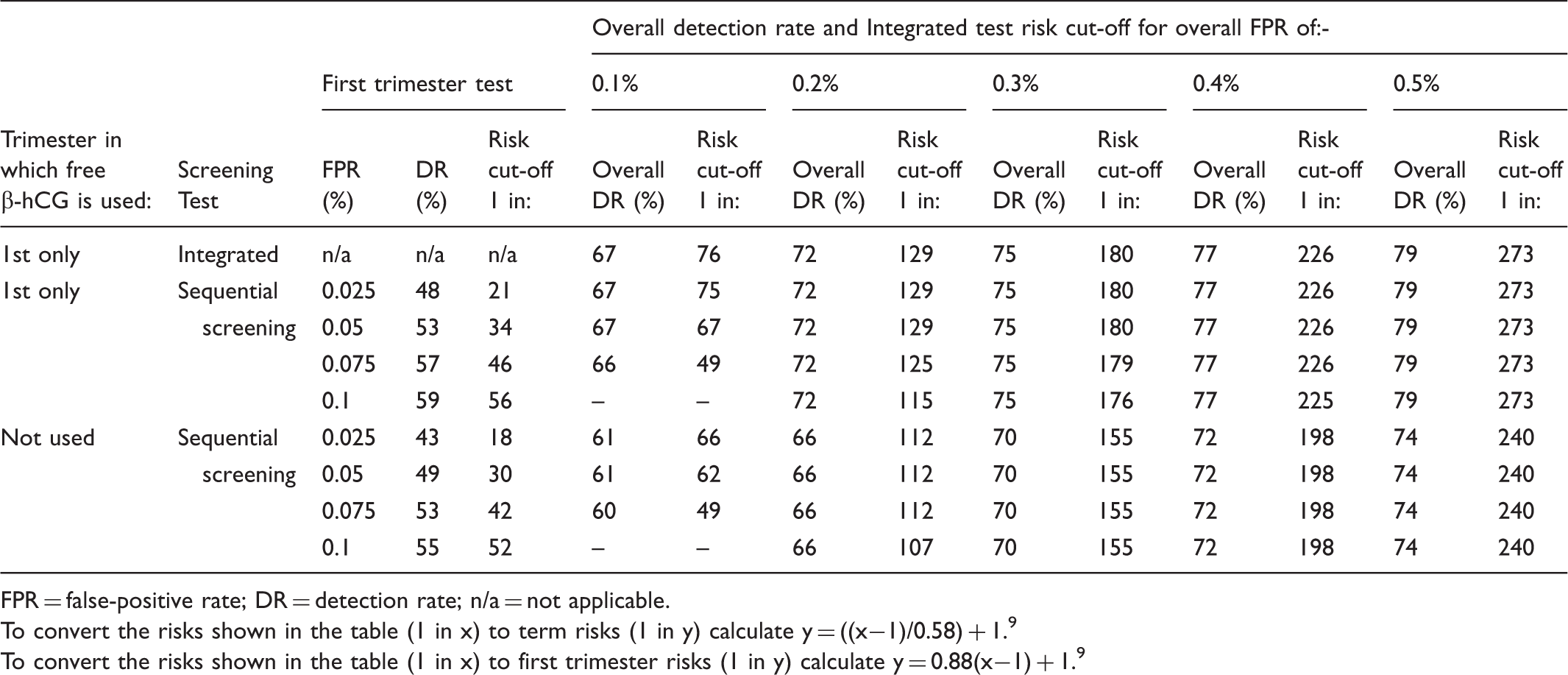
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.58) + 1. 9
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.88(x−1) + 1. 9
With free β-hCG not used in either trimester, at the same first trimester and overall false-positive rates, sequential Integrated screening detects 49% of trisomy 13 pregnancies in the first trimester, and 66% overall. As with sequential Integrated screening for Down’s syndrome and trisomy 18, the table shows that there is no material increase in the detection rate from increasing the overall false-positive rate.
Performance of Integrated and sequential Integrated screening for trisomy 13 according to risk cut-off levels and whether free β-hCG is used in the first or second trimester. Table based on early second trimester trisomy 13 risks.
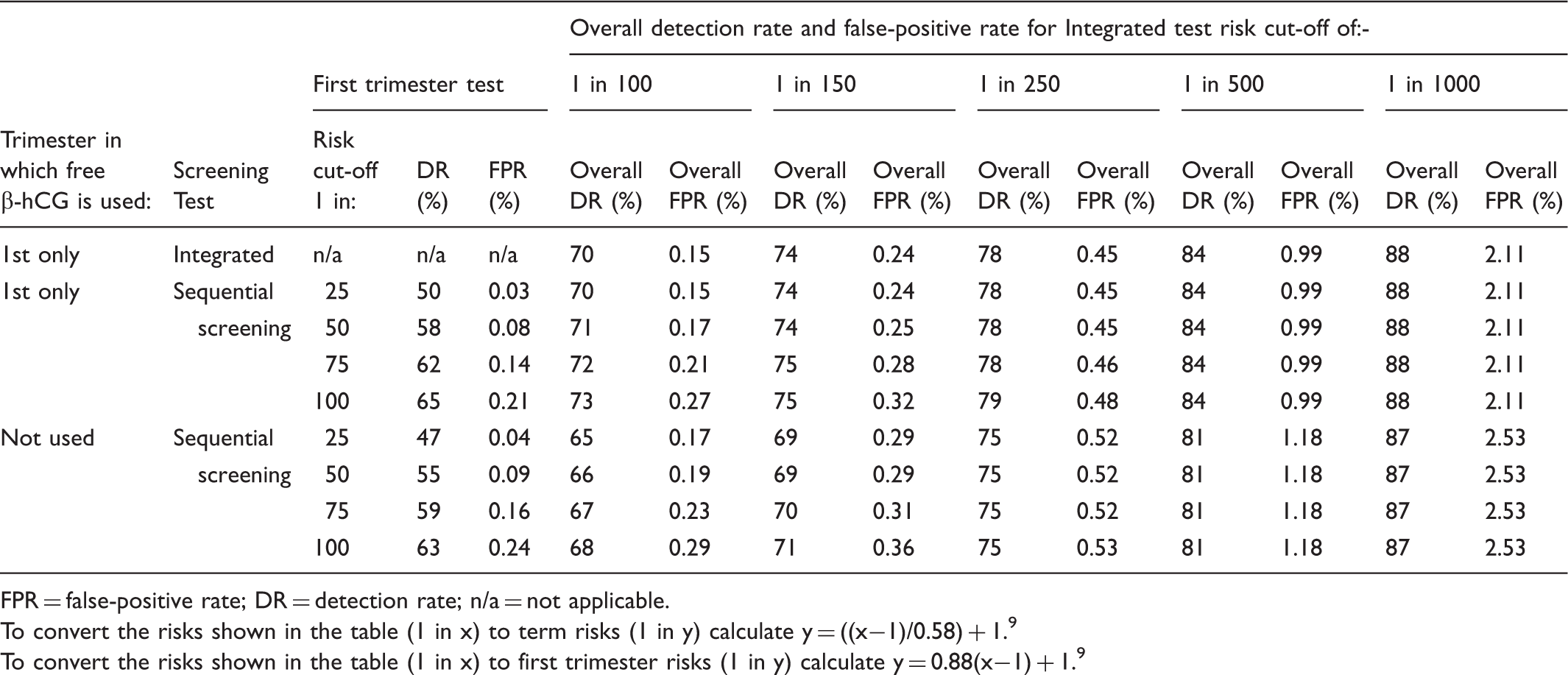
FPR = false-positive rate; DR = detection rate; n/a = not applicable.
To convert the risks shown in the table (1 in x) to term risks (1 in y) calculate y = ((x−1)/0.58) + 1. 9
To convert the risks shown in the table (1 in x) to first trimester risks (1 in y) calculate y = 0.88(x−1) + 1. 9
Supplementary Tables 1 to 15 provide more detailed estimates of the performance of sequential Integrated screening according to first trimester week of gestation for Down’s syndrome, based on the use of total hCG as well as free β-hCG, and according to term as well as early second trimester risks. The supplementary tables also provide estimates for all women having a Down’s syndrome Integrated test with hCG used in the first trimester only, and for all women having a trisomy 18 Integrated test with hCG used in the second trimester only.
Figure 1 is a flow diagram illustrating a protocol for sequential Integrated screening. The flow diagram uses first trimester test risk cut-offs of 1 in 25 for Down’s syndrome and 1 in 50 for both trisomy 18 and trisomy 13, and Integrated test risk cut-offs of 1 in 150 for Down’s syndrome and trisomy 13 and 1 in 250 for trisomy 18.
Flow diagram of sequential Integrated screening for Down’s syndrome (DS), Trisomy 18 (T18) and Trisomy 13 (T13). Figure based on early second trimester risks.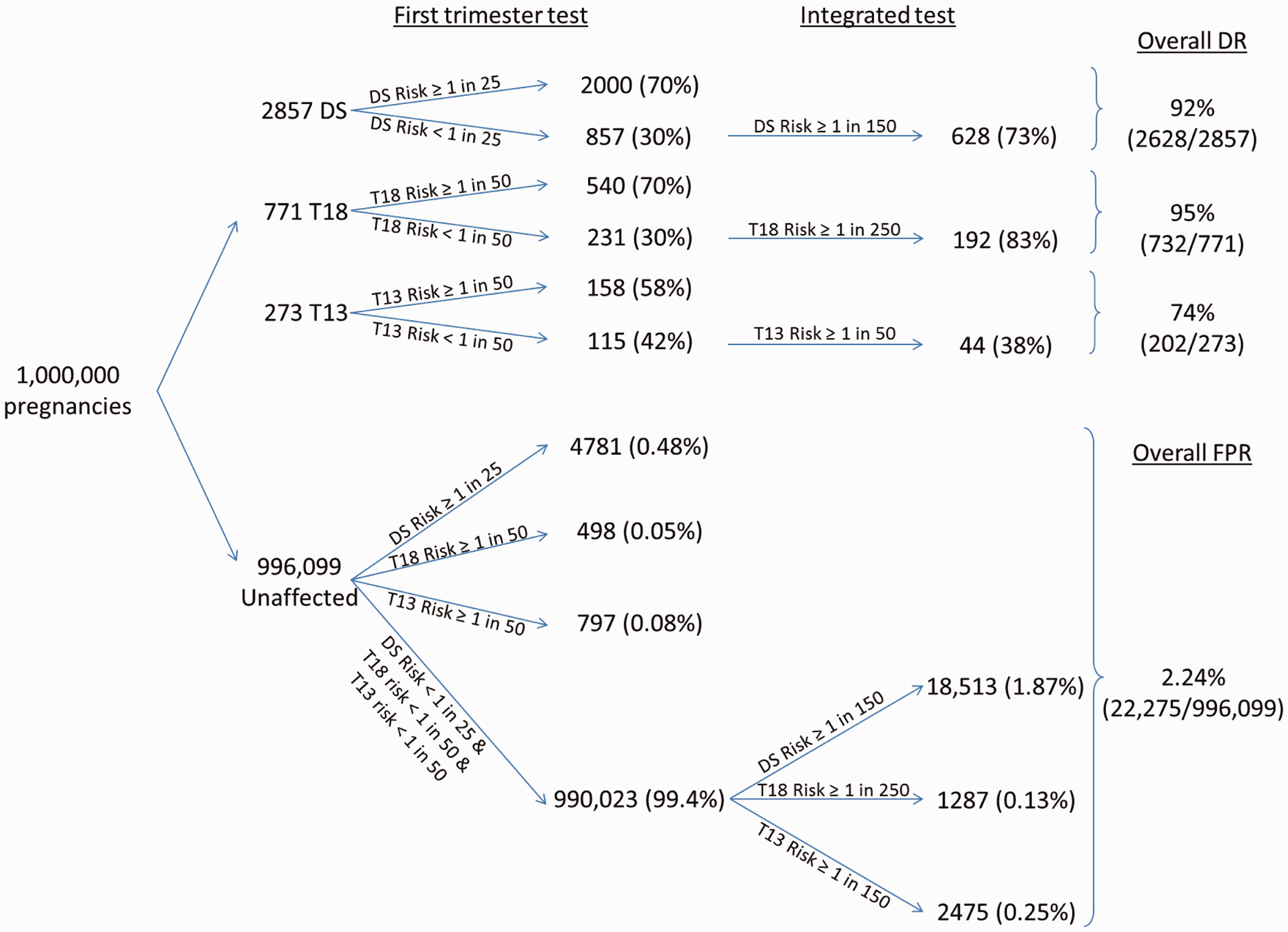
Discussion
Sequential Integrated screening has a high discriminatory performance that is similar to performing an Integrated test on all women, but with the advantage of identifying about 75% of Down’s syndrome and trisomy 18 pregnancies and about 55% of trisomy 13 pregnancies at about 10–12 weeks’ gestation, instead of 3–4 weeks later. Because the identification of trisomy 18 and trisomy 13 pregnancies is an ‘add-on’ to Down’s syndrome screening, the trisomy 18 and trisomy 13 false-positive rates need to be kept low, to avoid a large increase in the number of women exposed to invasive diagnostic testing. However, even at low overall trisomy 18 false-positive rates, over 90% of trisomy 18 pregnancies can be detected, and at low overall trisomy 13 false-positive rates, over 70% of trisomy 13 pregnancies can be detected. Of particular importance in sequential Integrated screening for trisomy 18 is that the first trimester risk cut-off must be set relatively high (about 1 in 50 for a first trimester false-positive rate of 0.05%), while the second trimester risk cut-off is relatively low (about 1 in 500). With these risk cut-offs, the overall detection rate is 96% and the false-positive rate 0.22%. The high first trimester cut-off follows the practice with sequential Integrated screening for Down’s syndrome, 1 but the second trimester risk cut-off is significantly lower than is typically used for Down’s syndrome (for example 1 in 150). In sequential Integrated screening for trisomy 13, the first trimester cut-off also needs to be set relatively high, but the second trimester risk cut-off would need to be similar to that used for Down’s syndrome, to avoid too high an increase in the overall false-positive rate.
In antenatal screening for Down’s syndrome, hCG (free β or total hCG) is a more discriminatory marker in the second trimester than in the first. 3 However, in antenatal screening for trisomy 18, hCG is more discriminatory in the first trimester, rather than the second trimester, and in antenatal screening for trisomy 13 hCG is only discriminatory in the first trimester. 5 To optimize screening performance for all three disorders, it would be beneficial for hCG to be measured in each trimester. If the screening policy was an Integrated test on all women, then the first trimester hCG measurements would be used to estimate the risk of a trisomy 18 or trisomy 13 pregnancy, but the second trimester hCG measurement would be used to estimate the risk of a Down’s syndrome pregnancy. In a sequential Integrated screening policy, a first trimester risk estimate would be calculated, using hCG for all three disorders, but for a Down’s syndrome Integrated test risk estimate the second trimester hCG measurement would be used, but not the first trimester measurement.
The spontaneous fetal loss rates of trisomy 18 and trisomy 13 pregnancies are high, and the early detection of the two disorders will necessarily mean that some pregnancies will be identified and offered a termination of pregnancy that would, in the absence of termination, have aborted spontaneously before completion of the second stage of the Integrated test. It can be estimated that because 72% of trisomy 18 and 49% of trisomy 13 pregnancies spontaneously abort between 12 weeks’ gestation and term, and 65% and 42% respectivey spontaneously abort between 18 weeks’ gestation and term, 7 about 1 in 5 trisomy 18 and about 1 in 8 trisomy 13 pregnancies would spontaneously abort before completion of the second stage of the Integrated test. In view of this, screening centres may choose to offer all women full Integrated tests for each disorder, rather than sequential Integrated screening. Whatever policy is adopted, our results should prove helpful in selecting the first and second trimester risk cut-off levels needed to achieve specified screening performance for Down’s syndrome, trisomy 18, and trisomy 13.
Screening performance for trisomy 18 and trisomy 13 is high, and compared with Down’s syndrome, the median survival for live births is low (14 days for trisomy 18 and 10 days for trisomy 13). 16 Because of this, some women may want to be screened for trisomy 18 and trisomy 13, but not for Down’s syndrome. This is likely to be a rare occurrence, and this option should probably rely on a woman requesting it, rather than introducing the choice as a matter of routine. To offer this choice to all women would require appropriately detailed pretest information and counselling, with the risk of misunderstanding and error, including the possibility of “ticking the wrong box” on a screening request form. It would probably be better to perform screening for all three disorders, and to provide counselling to women with positive results in respect of each one, so that a choice can be made at that stage on whether to proceed to a chorionic villus sampling (CVS) or an amniocentesis.
The false positive rates shown in the tables in this paper can approximately be added to the false positive rates calculated in screening for Down’s syndrome. This will overestimate the overall false positive rates to a small extent, because some women will be positive for both. For example, with full Integrated screening for all women, with a Down’s syndrome false-positive rate of 2%, the addition of Integrated screening for trisomy 18 and trisomy 13 with false-positive rates of 0.2%, the overall false-positive rate is 2.2% rather than 2.4%. 5 The same will be true for sequential Integrated screening for each of the three disorders, because the screening performance estimates are close to those for full Integrated screening on all women. The detection rates shown in our tables will also be slightly underestimated because, for example, a trisomy 13 pregnancy that is screen negative for trisomy 13 may be screen positive for either or both of Down’s syndrome and trisomy 18.
With the introduction of DNA screening methods, sequential Integrated screening protocols such as those described in this paper may be replaced by sequential screening using a first trimester test with a low, rather than a high initial risk cut off. Those with risks above the cut-off would have a DNA screening test, preferably adopting the reflex approach17,18 in which plasma from the original blood collection is retained and automatically retrieved, to avoid recalling women to collect a second blood sample.
The sequential Integrated screening protocol avoids causing unnecessary anxiety by only issuing a first trimester test result if it is positive. If all women were to receive their first trimester test risk estimate, some who were screen negative at this stage but with risk estimates that, in non-sequential screening, would still be judged to be high, would feel compelled to have a CVS or amniocentesis. This would undermine the efficacy and safety of sequential screening. Also providing women with more than one risk estimate for each disorder in the same pregnancy would be confusing, and women with a low risk after completing the Integrated test may be anxious about a higher first trimester risk and request an amniocentesis.
Our results should be useful to help centres that carry out sequential Integrated antenatal screening for Down's syndrome extend this, to screening for trisomy 18 and trisomy 13.
Footnotes
Declaration of conflicting interests
Nicholas Wald holds patents for the Integrated test, and is Director of Logical Medical Systems Ltd, which produces software for the interpretation of Down's syndrome screening tests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.