
Abstract
Objectives
Pregnancies with Edwards or Patau syndrome are often detected through screening for Down’s syndrome. We aimed to evaluate the impact of screening for Down’s syndrome on the prevalence of live births and antenatal diagnoses of Edwards and Patau syndrome.
Setting
England and Wales, 2005 to 2012.
Methods
Data from the National Down Syndrome Cytogenetic Register, which contains information on nearly all ante- or postnatally diagnosed cases of Edwards or Patau syndrome in which a karyotype was confirmed, were analysed.
Results
From 2005 to 2012, 3,941 diagnoses of Edwards syndrome and 1,567 diagnoses of Patau syndrome were recorded (prevalence of 7.0 and 2.8 per 10,000 births respectively). Only 11% (95% confidence interval [CI]: 10–12) of diagnoses of Edwards syndrome and 13% (95% CI: 11–14) of Patau syndrome were live births, resulting in live birth prevalences of 0.8 (95% CI: 0.7–0.8) and 0.4 (95% CI: 0.3–0.4) per 10,000 live births respectively. About 90% of pregnancies with Edwards or Patau syndrome were diagnosed antenatally, and this proportion remained constant over time. The proportion of diagnoses detected before 15 weeks increased from 50% in 2005 to 53% in 2012 for Edwards syndrome, and from 41% in 2005 to 63% in 2012 for Patau syndrome.
Conclusions
Almost 700 women per year had a pregnancy with Edwards or Patau syndrome. Over 90% of these pregnancies were detected antenatally, with the increased use of first trimester screening for Down’s syndrome resulting in the reduction in the mean gestational age at diagnosis of these syndromes.
Introduction
Edwards syndrome (trisomy 18) and Patau syndrome (trisomy 13) are the second and third most common autosomal trisomies in live births (Down’s syndrome, trisomy 21, is the most common), with live birth prevalence in the absence of antenatal screening and selective termination of 2.3 per 10,000 births for Edwards syndrome and 1.4 per 10,000 births for Patau syndrome. 1 Both syndromes affect multiple systems, and have a high risk of fetal death 2 and a median postnatal survival of two weeks, with only 1 in 12 surviving for one year or more. 3
Both first and second trimester screening tests for Down’s syndrome also identify some pregnancies with an increased risk of Edwards or Patau syndrome. The fetal anomaly scan between 18+0 and 20+6 weeks’ gestation will, in addition, detect structural anomalies associated with these syndromes. In 2010 the NHS Fetal Anomaly Screening Programme in England assigned a target detection rate of 90% for both Edwards and Patau syndromes for the fetal anomaly scan. Antenatal diagnoses of both syndromes can be obtained by karyotyping cells from amniocentesis or chorionic villus sampling.
This study used data from the National Down Syndrome Cytogenetic Register (NDSCR) to determine the proportions of pregnancies with these syndromes that are antenatally detected in England and Wales, and to evaluate whether the increased use of the first trimester combined screening test for Down’s syndrome from 2005 to 2012 has influenced the antenatal detection of these syndromes.
Methods
The data
Since 1 January 2004, all 20 clinical cytogenetic laboratories in England and Wales have completed a form for the NDSCR for each diagnosis of Edwards syndrome and Patau syndrome, and their variants. 4 Almost every baby with clinical features suggesting Edwards or Patau syndrome, as well as any antenatal diagnostic sample from a pregnancy suspected to have either syndrome, receives a cytogenetic examination, as the definitive test for the syndromes is detection of a whole or part of an extra chromosome 18 (Edwards syndrome) or chromosome 13 (Patau syndrome). The cases include live births, fetal deaths comprising stillbirths (24+ weeks) and late miscarriages (20–23 weeks) and terminations of pregnancy for fetal anomaly. Earlier fetal deaths (before 20 weeks) are rarely karyotyped, and those that were registered are unlikely to be representative of those in the population.
Data collected on each case include the sampling date, place of and indications for referral, karyotype, maternal age, family history, maternal postcode of residence, pregnancy outcome and the date of the outcome, and enough information to detect duplicates. Most laboratories send a copy of this form to the referring physician, for confirmation and completion. Annual reports of the findings are produced, the most recent for the year 2012. 5
The data from the NDSCR have been compared with those from other congenital anomaly registers in England and Wales, and with those of the Office for National Statistics. These comparisons have shown that, since its inception in 1989, the register has captured data for an estimated 93% of all diagnosed births and pregnancy terminations for Down’s syndrome. 6 Data from 2004 were excluded, as it was the first year of data collection of Edwards and Patau syndrome, and there was likely to be under-reporting in that year. Since then it is likely that the register is similarly complete for Down's, Edwards and Patau syndromes.
Statistical Analysis
Poisson regression was used to analyse any changes in prevalence from 2005 to 2012. All comparisons between categorical variables were made using chi-squared tests, and between continuous variables using t-tests, as appropriate. The Poisson distribution was used to calculate 95% confidence intervals (CI) for prevalence, and the binomial distribution was used to calculate 95% CIs for proportions. Statistical analyses were carried out using STATA version 12.
Results
From 2005 to 2012, 3,942 diagnoses (live births, stillbirths [24+ weeks], late miscarriages [20–23 weeks] and terminations of pregnancy for fetal anomaly) of Edwards syndrome, and 1,567 of Patau syndrome were notified to the NDSCR; a prevalence of 7.0 (95% CI: 6.8 to 7.2) per 10,000 (live and still) births for Edwards syndrome and 2.8 (95% CI: 2.6 to 2.9) per 10,000 births for Patau syndrome. The prevalence of both syndromes remained constant between 2005 and 2012. The prevalence of Edwards syndrome was significantly higher amongst females than males: 7.4 (95% CI: 7.1 to 7.8) and 5.7 (95% CI: 5.4 to 6.0) per 10,000 births respectively. The prevalence of Patau syndrome did not differ between females and males: 2.5 (95% CI: 2.3 to 2.7) and 2.7 (95% CI: 2.5 to 2.9) per 10,000 births respectively.
The majority of cases of Edwards and Patau syndrome had an additional chromosome (97% and 90% respectively), as previously observed. 7 Just over 1% of cases of both Edwards and Patau syndrome were mosaic (some cells had an additional chromosome and others did not). However, there was a much larger proportion of cases with translocation Patau syndrome than translocation Edwards syndrome (8% vs. 1%) (each cell had an additional part of a chromosome, not the full additional chromosome).
There were 69 twins (1.8%; 95% CI: 1.4% to 2.2%) with Edwards syndrome (eight in whom both twins were affected) and 35 twins (2.2%; 95% CI: 1.6% to 3.1%) with Patau syndrome (four in whom both twins were affected), compared with the national twinning rate of 1.6% in 2012. 8
The prevalence of both syndromes increased significantly with maternal age, the mean age of mothers being 36.3 years for Edwards syndrome and 34.4 years for Patau syndrome, significantly higher than for all mothers in England and Wales in 2012 (29.8 years). 9
Number of cases, percentage and 95% confidence intervals of Edwards and Patau syndrome according to birth outcome; England and Wales: 2005–2012.
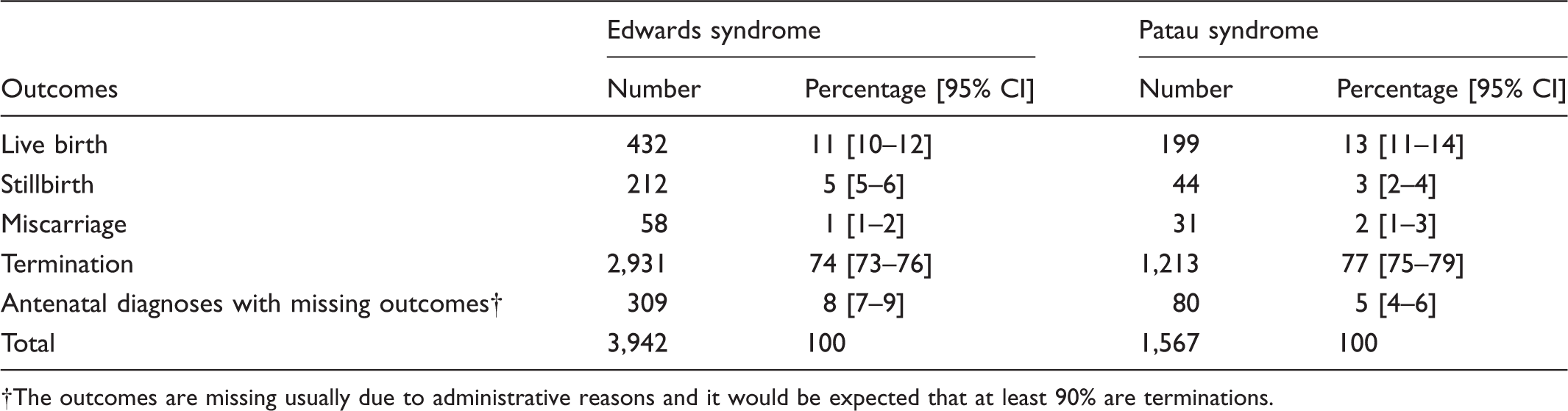
The outcomes are missing usually due to administrative reasons and it would be expected that at least 90% are terminations.
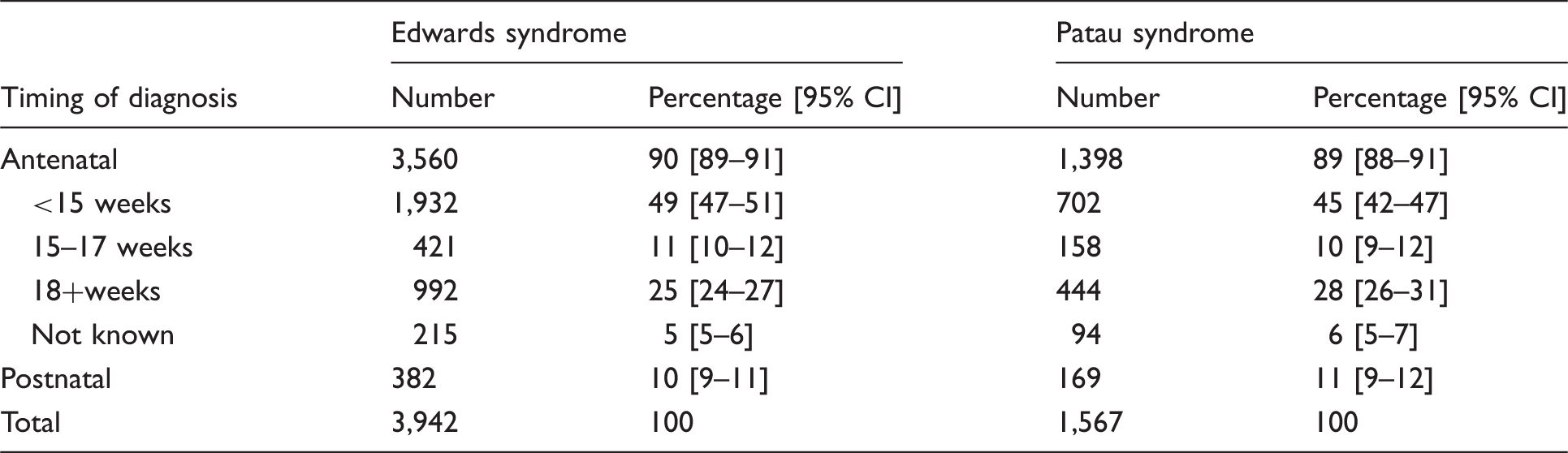
Number of cases, percentage and 95% confidence intervals of Edwards and Patau syndrome according to timing of diagnosis; England and Wales: 2005–2012.
After an antenatal diagnosis of Edwards syndrome, 10% of women decided to continue the pregnancy. Of these, 63% (95% CI: 58 to 69) of fetuses were stillbirths and miscarriages. This was similar for Patau syndrome, with 8% of women continuing with the pregnancy, in which 42% (95% CI: 33 to 51) of the fetuses were stillbirths and miscarriages. These fetal loss rates are consistent with those reported by Morris et al. 10
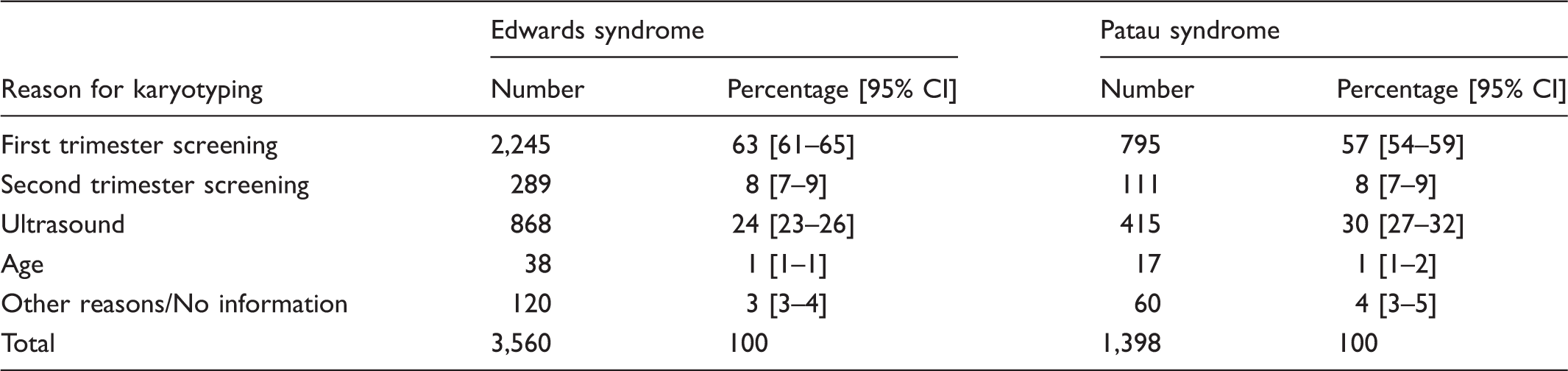
Number of cases, percentage and 95% confidence intervals of Edwards and Patau syndrome according to reason for antenatal karyotyping; England and Wales: 2005–2012.
Of the 382 postnatal diagnoses for Edwards syndrome (Table 2), 81 were recorded as declining screening, 98 were screened, and there were no data for 203. It is therefore known that at least 21% (81/382) were not diagnosed as screening had been declined. Similarly, for 169 postnatal diagnoses of Patau syndrome, 35 declined screening, 40 were screened, and there was no information for 94; at least 21% were not diagnosed as screening had been declined. When including only those women who accepted screening, the proportion antenatally diagnosed is 92% (3,559/(3,941-81)) for Edwards syndrome and 91% (1,398/(1,567-35)) for Patau syndrome, both of which fall above the NHS Fetal Anomaly Screening Programme target detection rate of 90%.
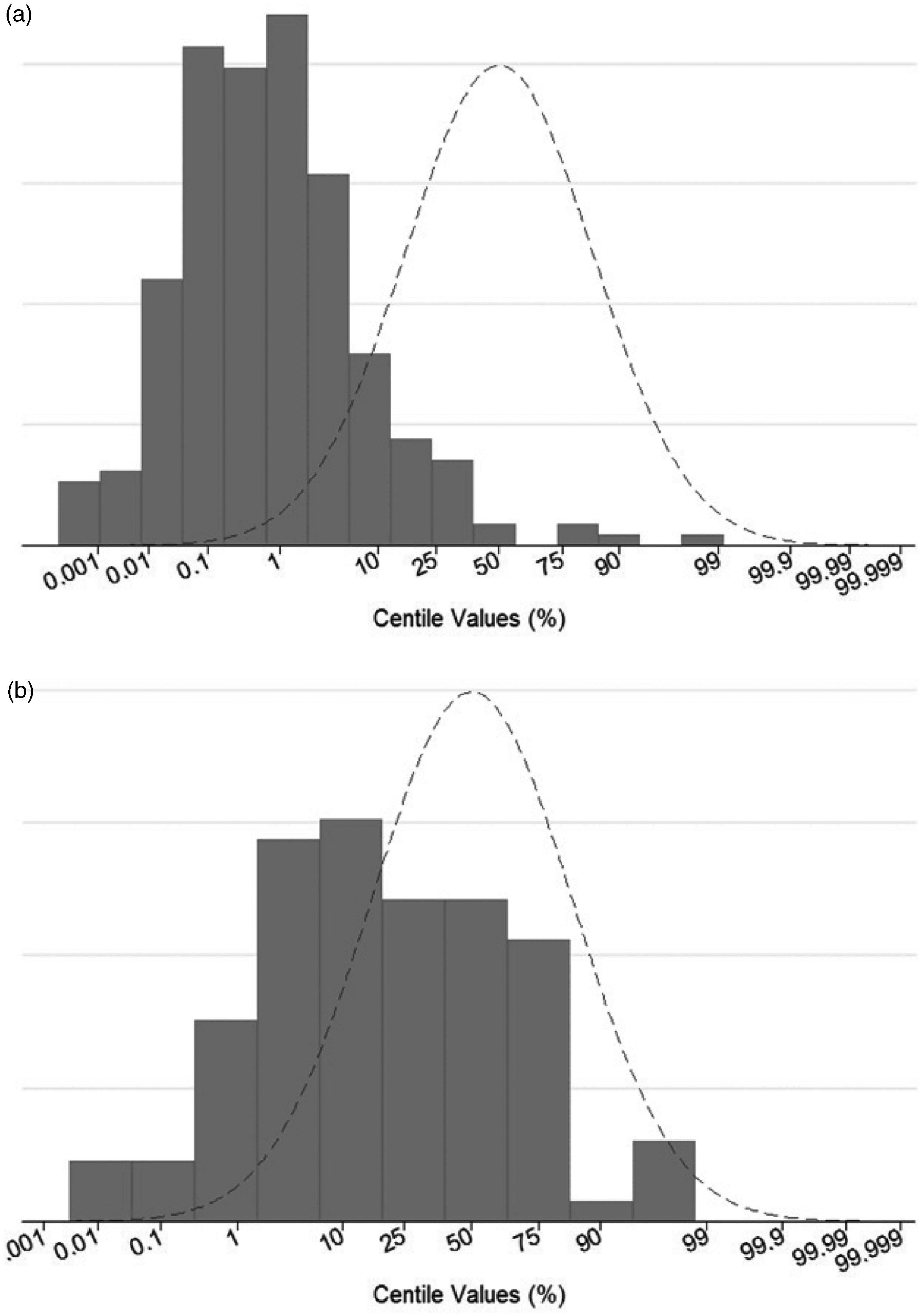
Figures 1 and 2 show that babies with Edwards and Patau syndrome tended to be born earlier than unaffected babies (median gestational age is 37 weeks), and were much lighter than unaffected babies, even when adjusted for gestational age, with over 75% of babies with Edwards syndrome and 22% of babies with Patau syndrome lying below the 3rd centile. The mean birth weight at 37 weeks’ gestation was 1900 g (1st centile) for Edwards syndrome, and 2600 g (23rd centile) for Patau Syndrome.
The distribution of gestational age at birth in babies with Edwards (a) and Patau (b) syndrome (bars) (2005–2012) compared with unaffected babies (line) (Office for National Statistics 2011). Proportion of live born cases of Edwards (a) and Patau (b) syndrome (bars) and unaffected cases (curve) according to birth weight centiles adjusted for gestational age; England and Wales: 2005–2012.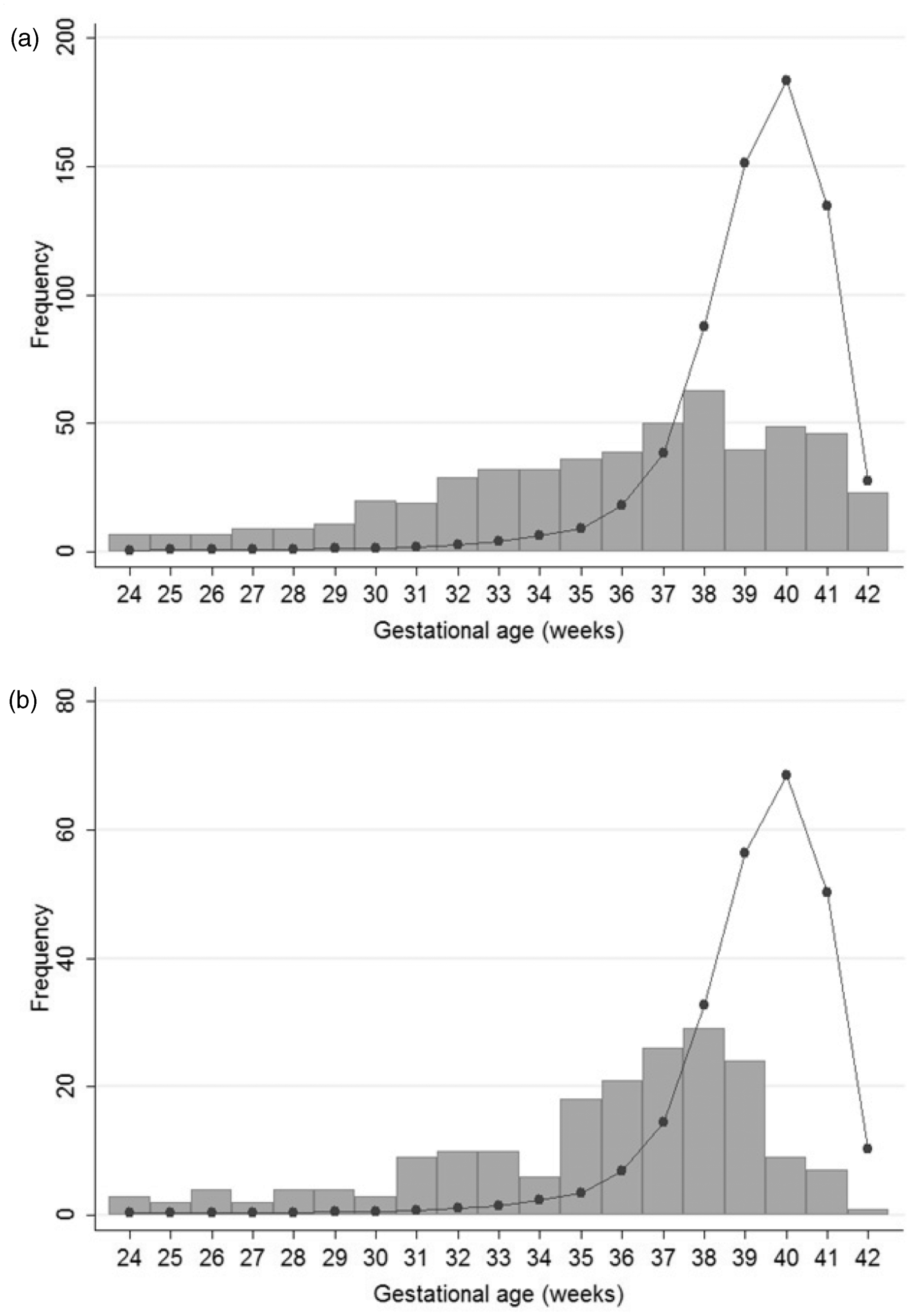
Discussion
This study shows that the prevalence of Edwards syndrome was 7.0 per 10,000 births, and the prevalence of Patau syndrome was 2.8 per 10,000 births in England and Wales between 2005 and 2012. During this time, 90% of cases of Edwards syndrome and Patau syndrome cases were diagnosed antenatally, and the proportions diagnosed before 15 weeks’ gestation significantly increased for both syndromes.
Strengths and limitations of the study
The major strength of this study is that it is the largest of its kind, covering the whole population of England and Wales, with a likely 93% ascertainment level.
The major weakness of this study is the missing data relating to pregnancy outcome (7%). The missing outcomes were largely due to administrative delays in receiving data on pregnancy outcomes after an antenatal diagnosis. However, these delays are unrelated to the outcome in cases that we have subsequently managed to trace, of which 90% were terminations of pregnancy.
The NDSCR also lacks information on anomalies associated with Edwards and Patau syndrome, which will affect the diagnosis, survival, and outcome. Approximately 45% of babies with Edwards syndrome and 35% of babies with Patau syndrome have a heart anomaly. Babies with Edwards syndrome frequently have trachea-oesophageal fistula, cleft lip, diaphragmatic hernia, and spina bifida, while babies with Patau syndrome frequently have oro-facial clefts, abdominal wall defects, limb defects, and nervous system anomalies. 11
Comparison with other studies
The prevalence of Edwards and Patau syndrome were highly dependent on maternal age as, has been observed in many other studies.12,13 This may partially explain why the total prevalence of Edwards and Patau syndrome in this study (7.0 and 2.8 per 10,000 births respectively) were significantly higher than other European registries that are members of the European Surveillance of Congenital Anomalies (EUROCAT) 14 (4.4 and 1.7 per 10,000 births). Only the Paris registry had a higher prevalence. A second explanation may be that England introduced first trimester screening at an earlier time than many other European countries, 15 and therefore more pregnancies are being detected during the first trimester rather than resulting in fetal losses later in pregnancy before being diagnosed. This will increase the total prevalence, but as many of these pregnancies result in fetal losses, it will not increase the live birth prevalence. As expected, the live birth prevalences were comparable for both Edwards (0.77 per 10,000 live births in this study and 0.79 per 10,000 live births in EUROCAT registries) and Patau syndrome (0.36 and 0.37), due to the high level of fetal loss and terminations of pregnancy for fetal loss for both of these syndromes. The high ascertainment of cases in the NDSCR data 6 may also partially explain the higher prevalence in England and Wales compared with the other European registries.
The early gestational age at birth and the low birth weight observed in this study are consistent with those observed by Boghossian et al in their 2012 study of 1,053 infants with Edwards syndrome aged 22–41 weeks, and 613 infants with Patau syndrome aged 22–40 weeks. 16 Due to the high levels of prenatal detection, the gestational age at birth should be interpreted with caution, as it may be influenced by clinicians deciding to induce the birth early. However, there is strong evidence that the median gestational age at birth is 38 weeks rather than 40 weeks gestation for babies with Down’s syndrome, and the same effect may be occurring in Patau and Edward syndrome. 15
The future
It is likely that cell-free fetal DNA screening for Down’s syndrome will become widely available in Europe during the next few years, and that such screening will also include screening for Patau and Edwards syndrome. The availability of a more accurate screening test may encourage more women to have screening and the detection of affected pregnancies to occur earlier. However, as over 90% of such affected pregnancies are already detected prenatally, it is unlikely that a large impact on the live birth rate will occur.
Conclusion
From 2005 to 2012 almost 700 women per year in England and Wales had a pregnancy with Edwards or Patau syndrome. Over 90% of these pregnancies were detected antenatally, with a continual decrease in the gestational age at diagnosis. At least a quarter of the 10% of cases not detected antenatally were not diagnosed because the parents did not wish to have an antenatal diagnosis, not because the screening tests missed cases.
Footnotes
Ethical approval
The NDSCR (as part of the British Isles Network of Congenital Anomaly Registers) has multicentre research ethics committee approval from Trent MREC. It was granted section 251 class support under the NHS Act 2006 for the collection of personal information without consent.
Acknowledgments
We thank Professor Sir Nicholas Wald, Professor Judith Rankin, and Enid Hennessy for their comments on versions of this paper, and Haiyan Wu, Karen Clarke, and Ellen Clancy, who maintain the NDSCR database.
Declaration of conflicting interests
None declared.
Funding
The NHS Fetal Anomaly Screening Programme funded the NDSCR to collect data until March 2009, the Healthcare Quality Improvement Partnership funded the register until March 2013, and it is now funded by Public Health England. The funders played no role in the analysis or write up of this paper. Both authors are independent of all three funders, had full access to all of the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis.