
Abstract
Objective
Antenatal reflex DNA screening for Down’s syndrome has a high screening performance. We aimed to determine the performance of trisomy 18 and trisomy 13 reflex DNA screening when added to Down’s syndrome screening.
Methods
In our modelled screening protocol, women provide two samples: a serum sample for a Combined test and a plasma sample for a possible DNA test. Women with Down’s syndrome, trisomy 18, or trisomy 13 Combined test risks above a single cut-off have a reflex DNA test using the plasma sample, without the need to recall them to collect another sample and provide counselling. Women with a failed DNA test (after a second attempt using a fresh plasma sample) have an Integrated test, and are classified as positive if any of the Down’s syndrome, trisomy 18, or trisomy 13 Integrated test risks are greater than 1 in 25.
Results
At 1 in 800 term risk cut-offs for Down’s syndrome, trisomy 18, and trisomy 13, an estimated 10% of women are reflexed to DNA screening, yielding a 91% Down’s syndrome detection rate, an 89% trisomy 18 detection rate, and a 79% trisomy 13 detection rate for a 0.05% false-positive rate. At a 1 in 1900 term risk cut-off for Down’s syndrome, trisomy 18, or trisomy 13, an estimated 20% of women are reflexed to DNA screening, and this yields a 94% Down’s syndrome detection rate, a 92% trisomy 18 detection rate, and an 84% trisomy 13 detection rate for a 0.10% false-positive rate.
Conclusion
Reflex DNA screening for trisomies 18 and 13 can be usefully added to reflex DNA screening for Down’s syndrome.
Keywords
Introduction
Antenatal maternal serum and ultrasound screening for Down’s syndrome incidentally detects trisomy 18 and trisomy 13 pregnancies. 1 The addition of trisomy 18 and trisomy 13 screening algorithms increases the detection of these two disorders, with little increase in the false-positive rate. 1 Maternal plasma DNA screening has detection rates of 99% for Down’s syndrome, 96% for trisomy 18, and 91% for trisomy 13, with respective false-positive rates of 0.20%, 0.13%, and 0.13%, but is costly, and sometimes the test fails.2–4
Antenatal reflex DNA screening for Down’s syndrome has advantages such as reducing the false-positive rate, preventing test failures and reducing cost.5,6 Women provide two blood samples at about 11–13 weeks’ gestation, one for measurement of the serum marker components (free β-human chorionic gonatrophin [hCG], pregnancy-associated plasma protein-A [PAPP-A]) of the Combined test (which also includes the ultrasound marker nuchal translucency [NT] and maternal age) and another sample for a possible DNA test. Women with a Combined test risk above a specified level are reflexed to a DNA test using the sample already collected, without the need to recall them for another sample and counselling. Women with a failed DNA test after a second attempt using a fresh sample have the next best test: an Integrated test (Combined test with second trimester alphafetoprotein [AFP], unconjugated oestriol [uE3], and inhibin-A). Compared with DNA screening for all women, reflex DNA screening, with a 10% reflex rate, has been estimated to reduce the false-positive rate eight-fold (from 0.2% to 0.025%) whilst maintaining a Down’s syndrome detection rate greater than 90% and avoiding test failures. 6 We here assess reflex DNA screening for Down’s syndrome, trisomy 18, and trisomy 13. We also determine the improvement in the trisomy 18 and trisomy 13 screening performance by reflexing women using Combined test risk cut-offs for each of the three disorders, rather than using only a Down’s syndrome Combined test risk cut-off.
Methods
The screening performance of reflex DNA screening for Down’s syndrome has been previously described.5,6 Two million Down’s syndrome, trisomy 18, trisomy 13, and unaffected pregnancies were simulated, each with a set of ultrasound and serum marker values and a maternal age based on published screening marker parameters1,7,8 and the maternal age distribution of England and Wales 2006–2008. 9 For each simulated pregnancy and each disorder, a Combined test risk was calculated, by multiplying the maternal age-specific odds of having an affected live birth10,11 by the likelihood ratio of the pregnancy being affected (for the simulated set of marker values) which were calculated from the multivariate Gaussian distributions of NT, free β-hCG, and PAPP-A levels in affected and unaffected pregnancies. Women with any of the three disorder-specific risks greater than a specified cut-off level have a reflex DNA test, with a 2.5% failure rate (assuming a 5% initial rate with half successfully re-tested in a fresh blood sample 6 ). Among women who have a successful DNA test, the DNA test result was classified as positive or negative based on published detection rates and false-positive rates as follows: Down’s syndrome 98.6% and 0.20%, 2 trisomy 18 96.3% and 0.13% 4 , and trisomy 13 91.0% and 0.13%. 4 The overall false-positive rate is the sum of the individual false-positive rates (0.46%). For those with failed DNA tests, Integrated test risks were calculated for each disorder, and classified positive if any of the three Integrated test risks was greater than 1 in 25. An analysis in which women are reflexed to DNA screening based on using only Down’s syndrome test risk cut-offs was also performed.
Overall detection rates and false-positive rates for each disorder were estimated for Combined test risk cut-offs between 1 in 100 and 1 in 32,000. The results are given for women having first trimester Combined test markers measured at 11, 12, or 13 completed weeks of pregnancy. All analyses were performed in Stata version 12.
Results
Proportion of women reflexed to DNA screening and Down’s syndrome, trisomy 18, and trisomy 13 screening performance according to disorder-specific (Down’s syndrome, trisomy 18 and trisomy 13). Combined test risk cut-offs (risk at term) used to reflex women to DNA screening Combined test markers measured at 11 completed weeks’ gestation.
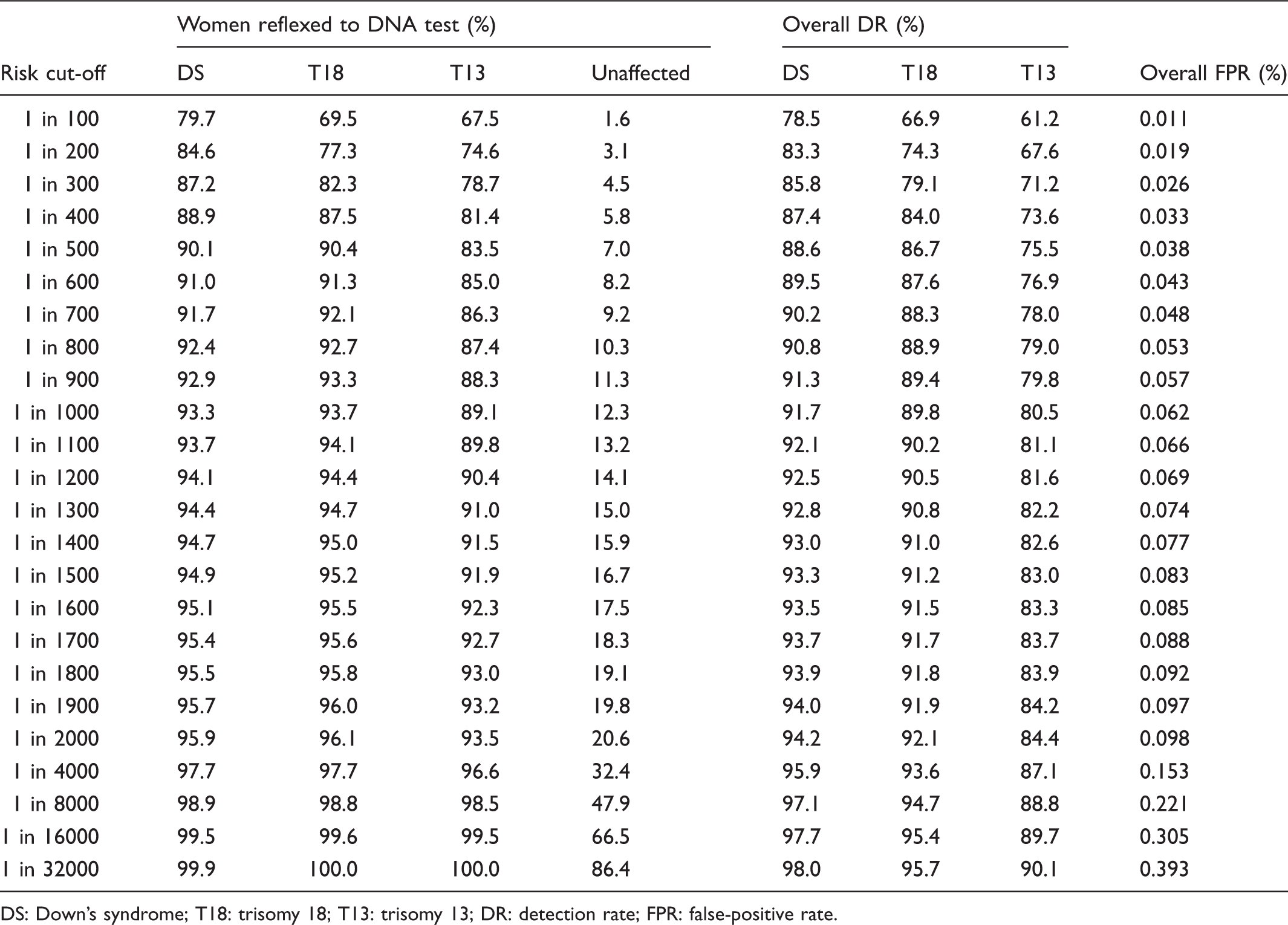
DS: Down’s syndrome; T18: trisomy 18; T13: trisomy 13; DR: detection rate; FPR: false-positive rate.
Supplementary Tables 1 and 2 show the results with first trimester Combined test markers measured at 12 and 13 completed weeks’ gestation, respectively. The results are similar to those shown in Table 1.
Comparison of screening performance of reflex DNA screening based on disorder-specific (Down’s syndrome, trisomy 18, and trisomy 13) Combined test risk cut-offs with reflexing women to DNA screening based on a Down’s syndrome Combined test risk cut-off only: Down’s syndrome, trisomy 18, and trisomy 13 detection rates, and false-positive rates according to Combined test risk cut-off(s) (risk at term) used to reflex women to DNA screening and completed week of gestation Combined test markers measured.
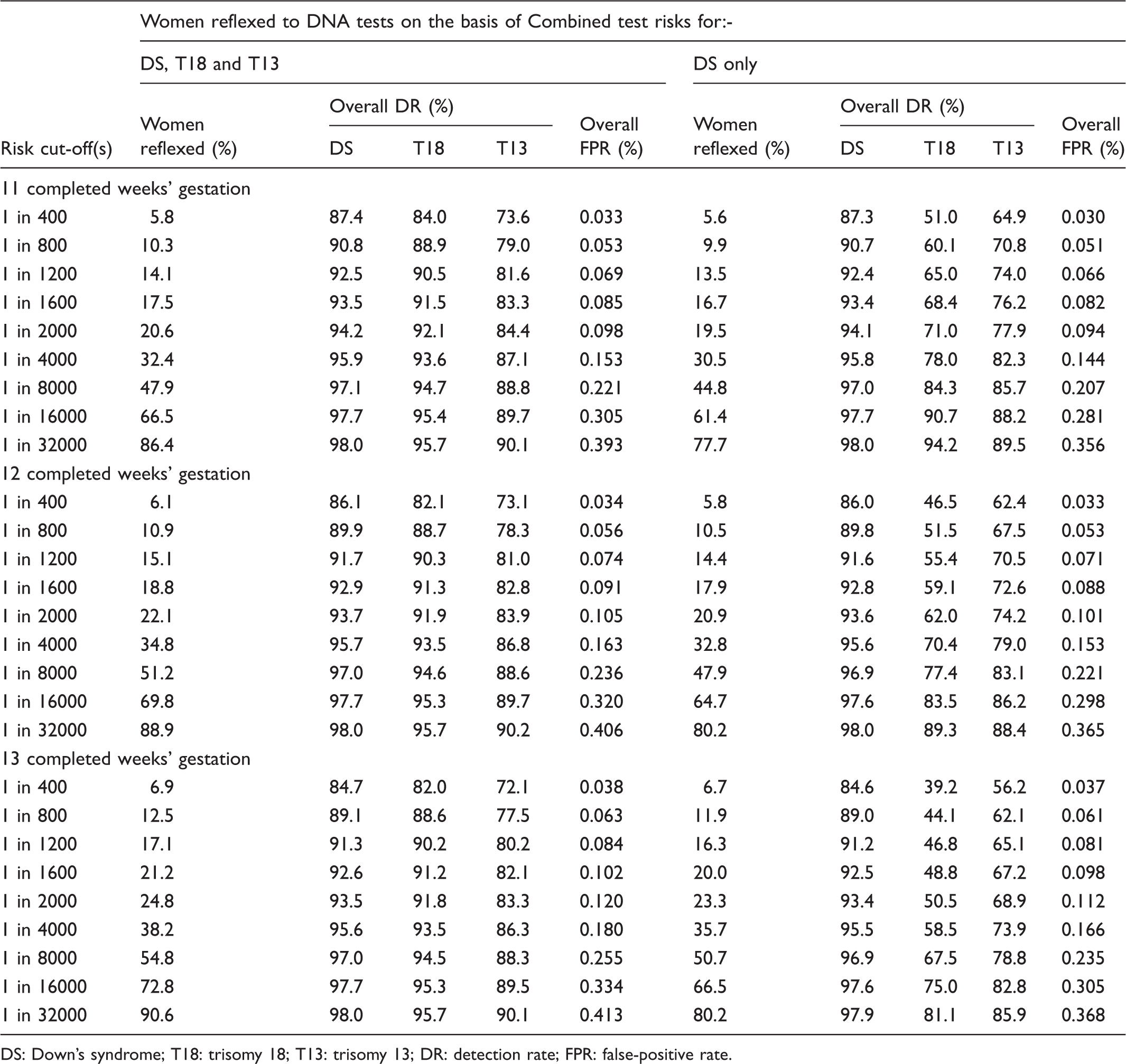
DS: Down’s syndrome; T18: trisomy 18; T13: trisomy 13; DR: detection rate; FPR: false-positive rate.
Discussion
Our results show that adding reflex DNA screening for trisomies 18 and 13 to reflex DNA screening for Down’s syndrome results in a high screening performance for the two disorders, with the additional detection of trisomy 18 and trisomy 13 pregnancies increasing with the gestation at which the Combined test markers are measured. Further, reflex DNA screening for Down’s syndrome, trisomy 18, and trisomy 13 results in a negligible increase in the false-positive rate compared with reflexing based on a Down’s syndrome Combined test risk only. Therefore it is better to use Combined test risk cut-offs for each of the three disorders to reflex women to DNA screening, rather than only a Down’s syndrome Combined test risk cut-off, and screening software programmes can enable this.
An advantage of the reflex DNA approach for all three disorders is a nine-fold reduction in the false-positive rate (from 0.46% to 0.053%)2–4 at a cost of an 8% point reduction in the Down’s syndrome detection rate (from 98.6% to 90.8%), a 7% point reduction in the trisomy 18 detection rate (from 96.3% to 88.9%), and a 12% point reduction in the trisomy 13 detection rate (from 91.0% to 79.0%) using Combined test risk cut-offs of 1 in 800. Using lower Combined test risk cut-offs to select women for DNA testing, for example, 1 in 1900, increases detection by about 3 to 5% points for the three disorders, but increases the false-positive rate about two-fold, and increases the costs due to performing twice the number of DNA tests. In practice, the advantage of an increase in the detection will need to be balanced against the extra cost of increasing the proportion of women reflexed to a DNA test.
The addition of reflex DNA screening for trisomy 18 and trisomy 13 to reflex DNA screening for Down’s syndrome leads to a small increase in the reflexing rate (about 1%), resulting in a small increase in the cost of DNA testing, and some saving from the avoidance of more diagnostic tests.
In summary, additional reflex DNA screening for trisomy 18 and trisomy 13 detects about 90% of trisomy 18 pregnancies and 80% of trisomy 13 pregnancies, with a low false-positive rate, so that only about 1 in 2000 unaffected pregnancies would be offered chorionic villus sampling or amniocentesis. Antenatal reflex DNA screening for trisomies 18 and 13 can be usefully added to reflex DNA screening for Down’s syndrome.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nicholas Wald holds patents for the Integrated test, and is Director of Logical Medical Systems Ltd, which produces software for the interpretation of Down’s syndrome screening tests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.