
Abstract
Objective
Maternal plasma DNA analysis has a high but imperfect antenatal Down’s syndrome screening performance. We aimed to determine the effect of combining DNA testing with current tests.
Methods
In our modelled screening protocol, women provide two samples, one serum sample for a Combined test, and a plasma sample for a possible DNA test. Women with a Combined test risk above a specified level have a DNA test using the plasma sample without the need to recall them for another sample and counselling (ie. in a reflex manner). Women with a failed DNA test after a second attempt using a fresh plasma sample have an Integrated test. Screening performance was estimated according to the proportion of women reflexed to DNA testing and compared with universal DNA testing.
Results
Reflexing 10% of women to a DNA test yields a 91% detection rate (DR) for a 0.025% false-positive rate (FPR) and no failed tests, compared with a 98% DR, 0.2% FPR and a 2.5% test failure rate with universal DNA testing (94% for 0.046% if 20% reflexed). DNA test failure rate has little influence on screening performance
Conclusion
Reflex DNA testing substantially reduces the FPR with a relatively small loss in detection compared with universal DNA testing, and reduces patient anxiety by avoiding the recall of women for DNA testing.
Introduction
Maternal plasma DNA analysis has the highest screening performance of any single test used in the antenatal detection of Down’s syndrome.1–11 These DNA testing methods achieve a Down’s syndrome detection rate (proportion of Down’s syndrome pregnancies with positive results) (DR) of 98–99% for a false-positive rate (proportion of unaffected pregnancies with positive results) (FPR) of about 0.2%, but, in a few percent of samples received, the test fails. The precise screening performance and failure rate is likely to depend on the particular DNA analysis used. The FPR, though low, is not low enough for the test to be used diagnostically; chorionic villus sampling (CVS) or amniocentesis is still needed to make the diagnosis.
Incorporating a DNA test into current screening methods, so that only a proportion of women have a DNA test, could have medical advantages as well as saving costs compared with universal DNA testing, by substantially reducing the FPR, with a relatively small reduction in DR. We conducted a modelling study to investigate this, by estimating the DRs and FPRs according to the percentages of women that have a DNA test on the basis of the screening result from a first trimester Combined test (free β-human chorionic gonatrophin [hCG], pregnancy associated plasma protein-A [PAPP-A], and nuchal translucency [NT] with maternal age). Collecting a plasma sample at the same time as the serum sample and using a “reflexing” approach12,13 in which, if necessary, the second blood sample is automatically used for DNA testing avoids the need to recall women for counselling and the collection of another blood sample. We here estimate the screening performance of this reflexing protocol (see Figure 1) and consider the implications. We compare its screening performance with screening using the Combined test or the Integrated test (first trimester PAPP-A and NT with second trimester free β-hCG, alphafetoprotein [AFP], unconjugated oestriol [uE3], and inhibin-A). We also compare it with screening based on universal DNA testing.
Flow chart of reflex DNA testing with the Combined test.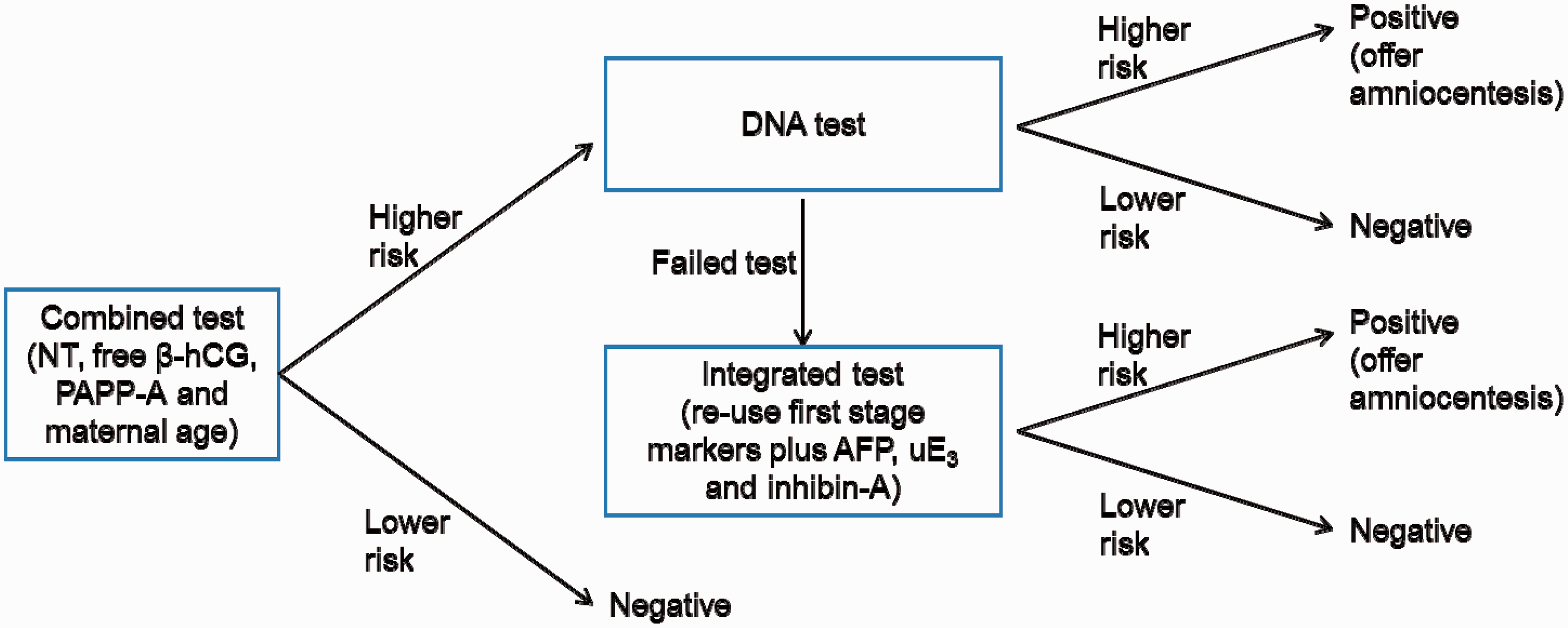
Methods
The screening performance of reflex DNA testing was estimated using the multivariate Gaussian distribution parameters (means, standard deviations and correlation coefficients) of the screening markers from a large cohort study (the Serum Urine and Ultrasound Screening Study [SURUSS]), 14 revised to incorporate subsequent improvements. 15 Two million Down’s syndrome pregnancies and two million unaffected pregnancies were simulated, each with a set of marker values (first trimester marker values measured at 11, 12, or 13 completed weeks’ gestation). Each simulated pregnancy was assigned a maternal age based on the distribution of maternities in England and Wales from 2006 to 2008 16 inclusive and the maternal age-specific odds of an affected livebirth.17–19
For each simulated pregnancy, a risk of being affected with Down’s syndrome based on the Combined test was calculated by multiplying the maternal age specific odds of having an affected live birth by the likelihood ratio of being affected (for the simulated set of marker values) which were calculated from the multivariate Gaussian distributions of NT, free β-hCG and PAPP-A levels in affected and unaffected pregnancies. The risk cut-offs for proportions reflexed to DNA testing from 1% to 99% were determined. A DNA result for those with a risk greater than the calculated risk cut-off levels was generated. The DNA test failure rate was taken as 2.5%, assuming a higher initial failure rate of 5%, with half of these successfully re-tested in a fresh blood sample collected later in pregnancy. Of those tests in which a DNA result was assumed to have been successfully obtained, the screening performance was taken from Palomaki et al, 2 so 98.6% of the simulated Down’s syndrome pregnancies and 0.2% of the simulated unaffected pregnancies were randomly classified as being screen positive based on DNA sequencing. If the DNA test failed, an Integrated test was performed, re-using the first trimester Combined test markers with the second trimester markers AFP, uE3 and inhibin-A in the multivariate Gaussian model to obtain an Integrated risk estimate of Down’s syndrome. Pregnancies with an Integrated test risk greater than or equal to 1 in 25 were classified as being screen positive. Overall DRs and FPRs were estimated, and compared with the corresponding estimates for women having either a Combined test or an Integrated test only (no DNA testing) and with the estimates for universal DNA testing. The latter involves either offering women with failed tests (i) a diagnostic amniocentesis (or CVS), or (ii) a second trimester Quadruple screening test (AFP, uE3, hCG, inhibin-A, and maternal age). The results are given for women having first trimester markers measured at 11, 12, or 13 completed weeks of pregnancy. All analyses were performed in Stata version 12.
Results
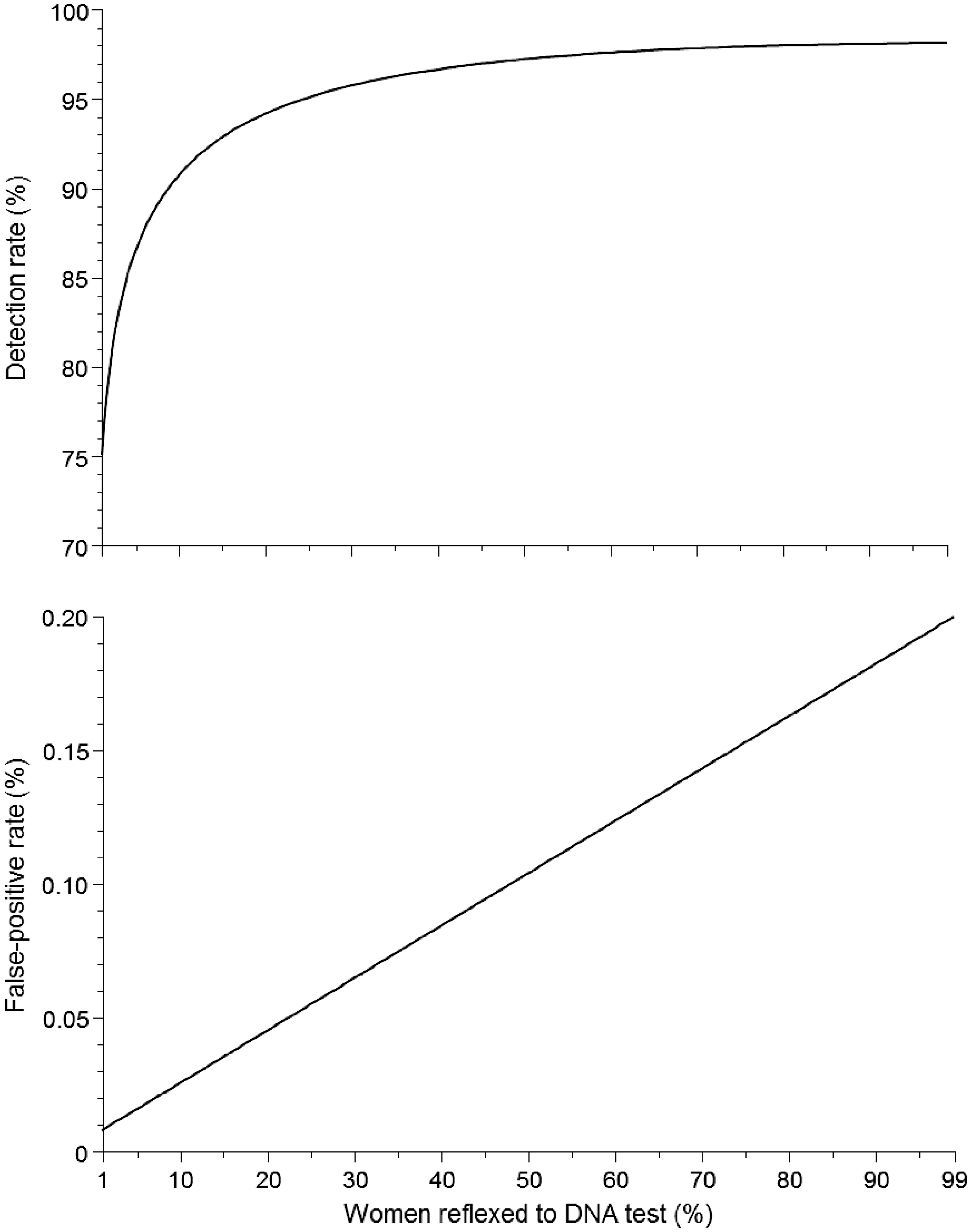
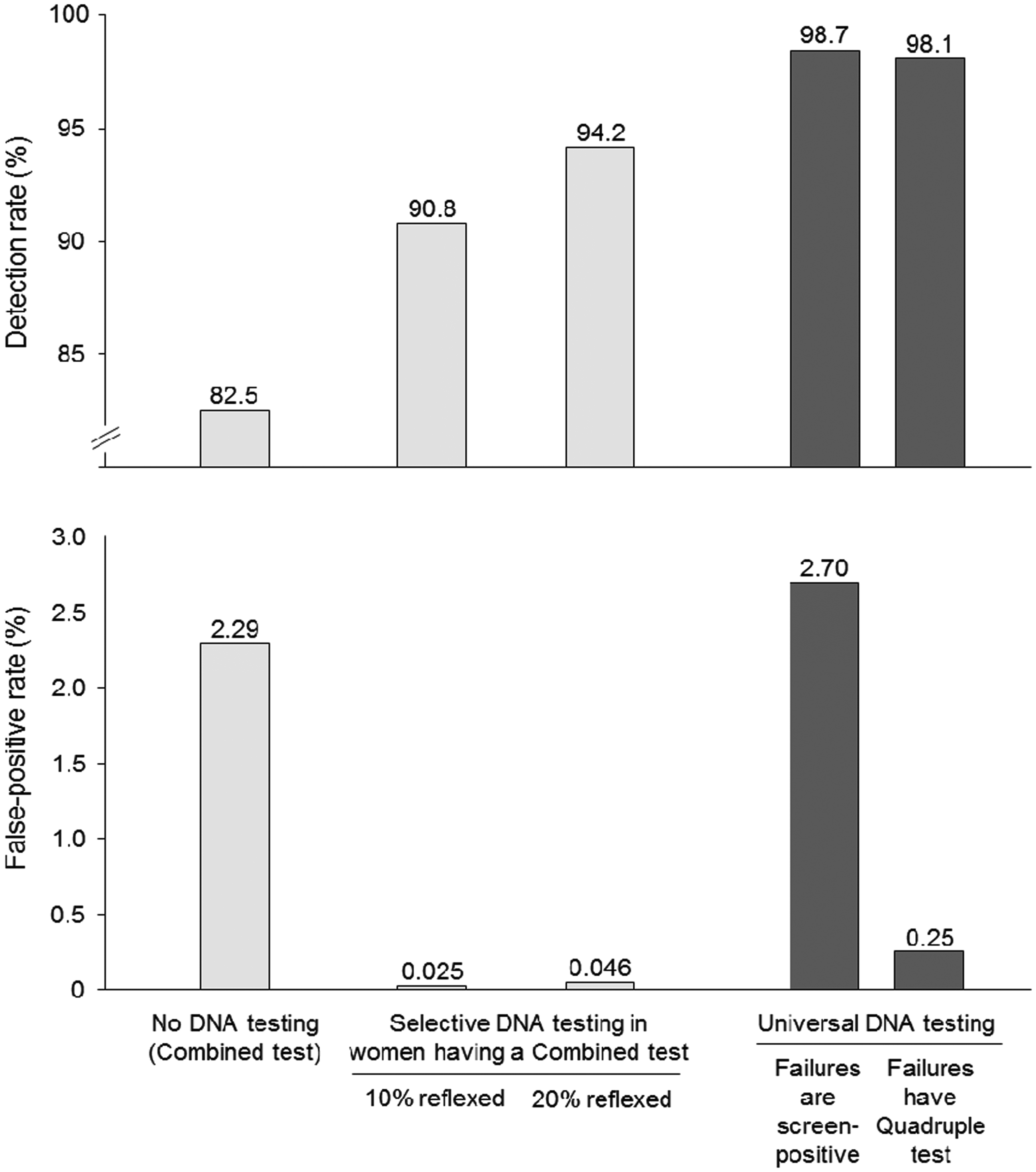
Figure 2 is a flow diagram of the reflex screening protocol, in which 10% of women have a DNA test. The DR is 91% and the FPR is 0.025%. Figure 3 shows the DR and FPR according to the percentage of women reflexed to a DNA test. As this increases, the DR increases (upper part of figure 3), as well as the FPR (lower part of figure 3). Figure 4 shows the DRs and FPRs according to three policies: (i) no DNA testing (Combined or Integrated test only), (ii) reflex DNA testing with 10% or 20% of women reflexed to a DNA test, and (iii) universal DNA testing, with women who have DNA test failures offered an amniocentesis (or CVS) or have the second trimester Quadruple screening test. The figure shows that the reflexing policy has a relatively small loss in detection but a substantial reduction in the FPR compared with universal DNA testing. For example, a universal DNA testing policy with test failures having an amniocentesis (or CVS) has a DR of 98.7% and a FPR of 2.70%, compared with a DR of 94.2% and a FPR of 0.046% with a 20% reflexing policy.
Reflex DNA screening with the Combined test: 10% of women have DNA test. First trimester markers measured at 11 completed weeks of gestation (DR = detection rate; FPR = false-positive rate). Detection rate and false-positive rate according to proportion of women reflexed to DNA testing; DNA test linked to Combined test. First trimester markers measured at 11 completed weeks of gestation. Detection rate and false-positive rates of selected screening policies. First trimester markers measured at 11 completed weeks of gestation.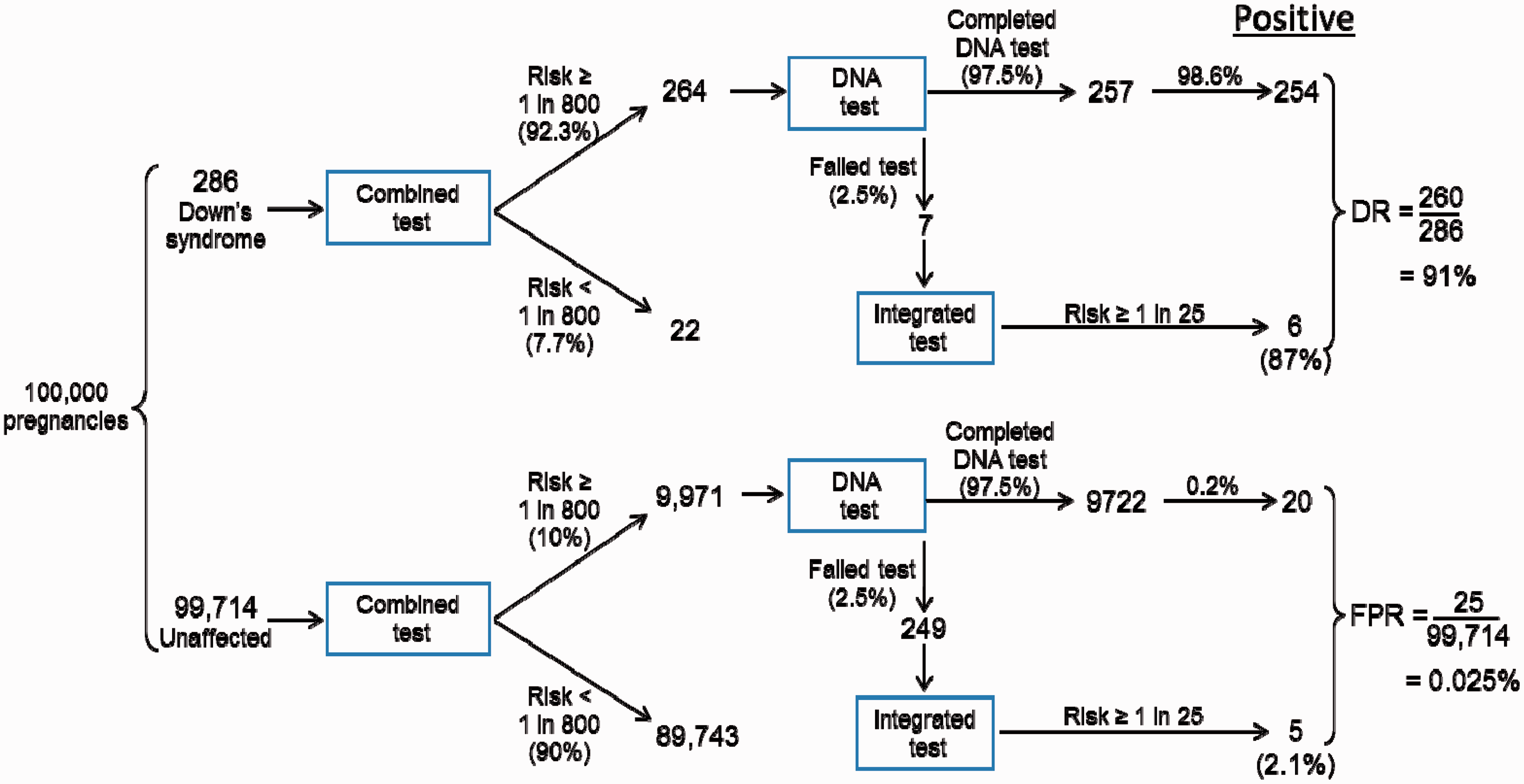
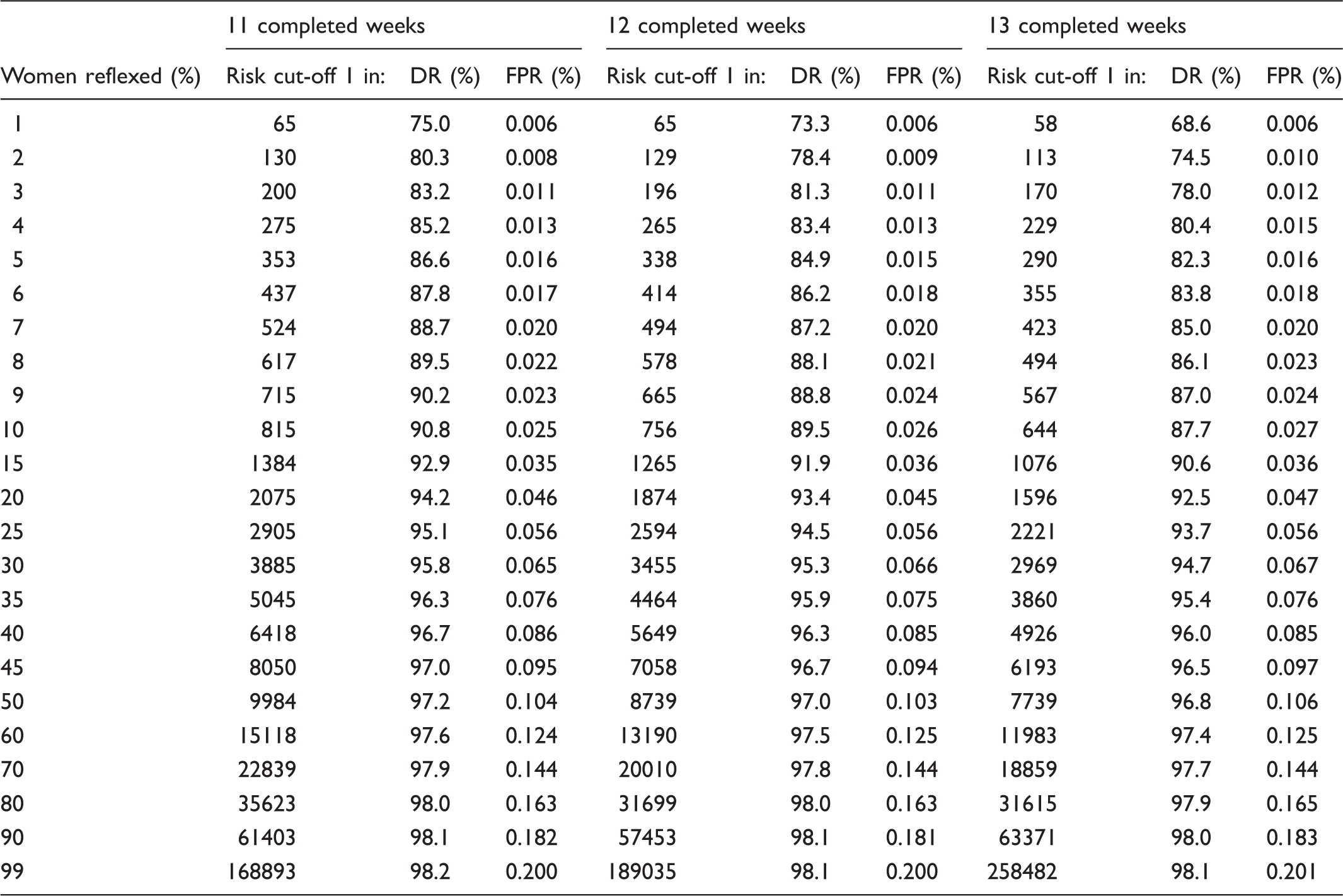
Reflex DNA screening linked to the Combined test: detection rate (DR) and false-positive rate (FPR) according to proportion of women reflexed to DNA testing (with risk cut-off specified) and completed week of gestation for the Combined test (DNA test failures have Integrated test using a risk cut-off 1 in 25).
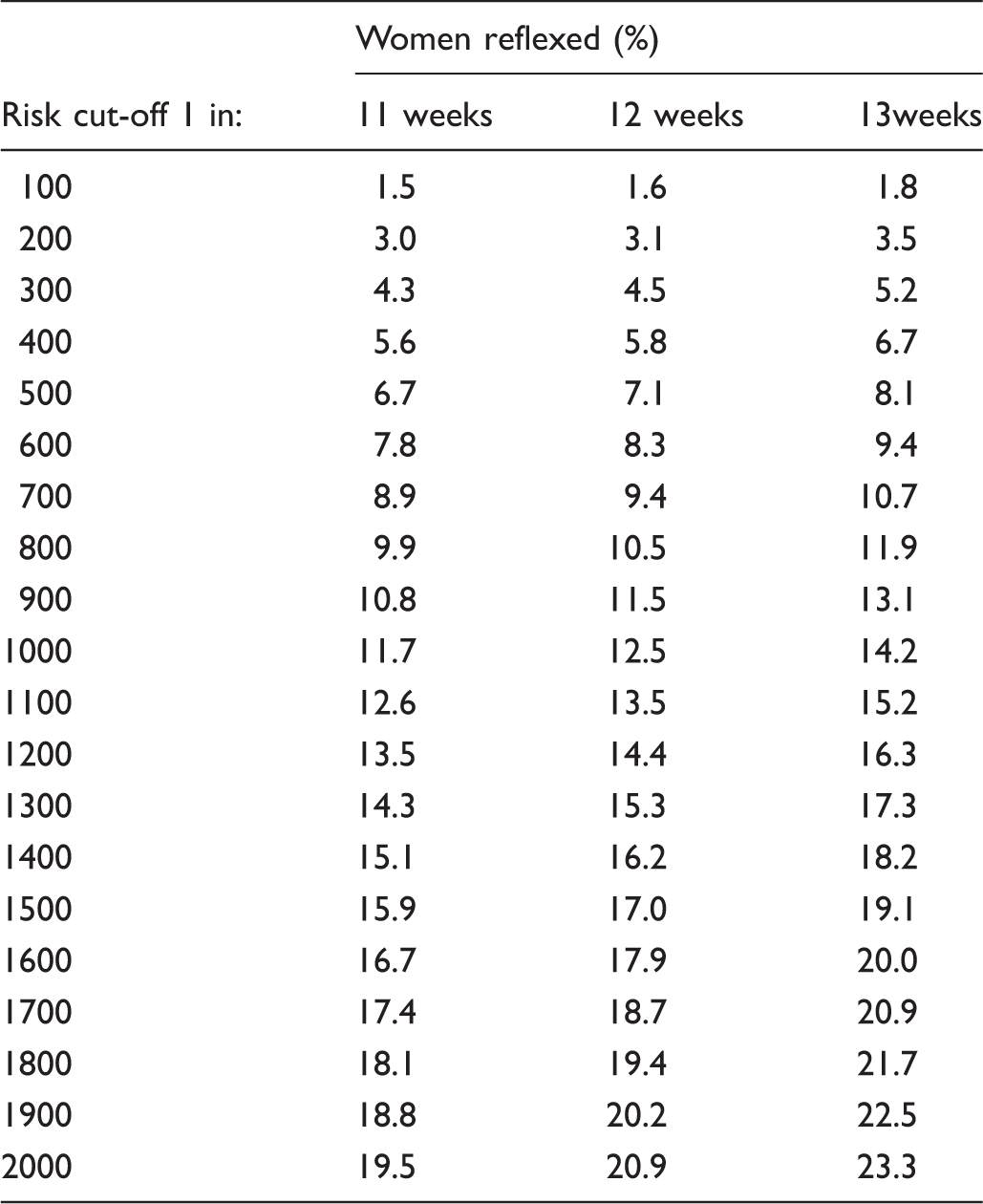
Reflexing proportion according to first trimester Combined test risk cut-off and week of pregnancy.
Discussion
Our results show that a high screening performance can be achieved through reflex DNA testing, with a FPR about one-eighth that of universal DNA testing, with a relatively small loss in detection.
The DNA test failure rate in the context of a reflexing policy has little impact on overall screening performance, for example if the rate were 1.25% instead of 2.5%, the DR would be 90.9% instead of 90.8% and the FPR 0.023% instead of 0.025%, and if the failure rate were 5%, the corresponding DR would be 90.5% and FPR 0.030%. With a universal DNA testing policy, test failures is a problem (see figure 4). If DNA testing had no false-positives, no failed tests, and was inexpensive, universal DNA testing could replace current screening methods. At present this is not the case, so a combination of current routine methods of screening and DNA testing offers the most effective approach.
Reflex DNA screening results in a lower FPR than universal DNA testing because the DNA test is limited to a subset of the women screened, namely those with a Combined test risk high enough to lead to a DNA test. In the example shown in Figure 4, with 10% reflexed to DNA testing, and with a DNA test FPR of 0.2%, the use of both in sequence yields an expected testing of 0.2% of 10%. With an Integrated test performed when the DNA test fails, this increases the FPR from 0.02% to 0.025%
With a DNA reflexing approach,12,13 plasma samples are collected from all women screened at the time of blood collection for the measurement of first trimester markers hCG and PAPP-A at 11, 12, or 13 weeks of pregnancy. Then women selected for DNA testing do not need to be approached; their stored plasma samples are retrieved for DNA testing. The screening strategy is explained and consent obtained when screening is initially offered. Others have reported on the advantages of incorporating DNA testing into current antenatal screening practice20–22 but have not suggested a reflexing approach. Without such an approach, women would need to be recalled for a DNA test, causing them anxiety through being singled out for further testing. The rationale for the reflexing approach is that it minimizes the FPR, and therefore the anxiety arising from screening, without loss of screening performance. It comes with an increased cost of having to collect and store plasma samples from all women, but only testing some. However, it avoids the cost of having to recall women for another blood sample.
The estimates in Table 2, linking the Combined test risk cut-off to the reflexing proportion can help to plan a reflex DNA screening programme, influenced also by the extent to which the DNA test failure rate is influenced by gestation.
Our statistical analysis is based upon the DNA result being categorical (positive or negative) and does not take account of the risk based on the result of the Combined test. An analysis that takes account of the Combined test risk produces almost identical screening results. For example with a reflexing proportion of 20% yielding an overall DR of 94.2%, the FPR is 0.045% instead of 0.046%. While combining information from two informative tests will yield a better screening performance than from either test alone, the discrimination of the DNA test is so much greater than that of the Combined test, adding quantitative information from the Combined test to a categorical DNA result has little effect. In expectation, the performance of such sequential screening would be improved if the DNA results were expressed quantitatively, rather than categorically. To this end, it would be valuable if, in future, DNA results were expressed in the underlying units of measurement (for example, percentage DNA fragments mapped to chromosome 21), and the distributions of this measurement determined in affected and unaffected pregnancies, as has been done in the past with conventional serum markers, such as hCG.
If women with failed DNA tests were automatically offered an amniocentesis (or CVS), the FPR would be approximately equal to the test failure rate, but the increase in the DR would be negligible (eg. from 98.00 to 98.01%), If women with failed tests were not tested further, the DR would decrease by an amount equal to the test failure rate (eg. from 98 to 96.5%) and the FPR would be unchanged.
To be fully successful, reporting a DNA test result should not take longer than it takes to report a Combined test result. If it takes much longer, women will suspect that their risk was sufficiently high to warrant a DNA test and as a result may become worried. If the DNA test does take significantly longer to report, reflex DNA testing can be linked to the Integrated test. Since women are scheduled to provide a second blood sample 3–4 weeks after the first, there is no anxious waiting period for a test result. DNA results can be reported before the second stage of the Integrated test and obviate the need for a second sample. Screening performance of reflex DNA testing linked to the Integrated test is similar to that linked to the Combined test and may be an option for centres that already have established routine Integrated screening programmes. The appendix provides quantitative estimates of screening performance of reflex DNA testing linked to the Integrated test.
The reflexing DNA policy could also be adopted in relation to the second trimester Quadruple test if first trimester screening markers are not available, in which case the requirements for a rapid DNA test become even greater. This achieves a 94% DR for a 0.10% FPR with 20% of women having a reflex DNA test, a DNA test failure rate of 2.5% and in women with a failed DNA test, a Quadruple test risk cut-off of 1 in 100 to determine which women are offered an amniocentesis.
In summary, reflex DNA screening reduces the FPR substantially, and hence the anxiety arising from screening, with a relatively small loss of detection compared with universal DNA testing, and avoids the problem of failed tests. Demonstration projects in which reflex DNA testing is introduced in routine antenatal screening programmes, coupled with appropriate clinical audit, would be useful.
Footnotes
Conflict of interest disclosure
Nicholas Wald holds patents for the Integrated test, and is Director of Logical Medical Systems Ltd, which produces software for the interpretation of Down’s syndrome screening tests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.