
Abstract
Objectives
Positive rates in faecal immunochemical test (FIT)-based colorectal cancer screening programmes vary, suggesting that differences between programmes may affect test results. We examined whether demographic, pathological, behavioural, and environmental factors affected haemoglobin concentration and positive rates where samples are mailed.
Methods
A retrospective cohort study; 34,298 collection devices were sent, over five years, to screening invitees (median age 60.6). Participant demographics, temperature on sample postage day, and previous screening were recorded. Outcomes from colonoscopy performed within a year following FIT were collected. Multivariate logistic regression identified significant predictors of test positivity.
Results
Higher positive rate was independently associated with male gender, older age, lower socioeconomic status, and distally located neoplasia, and negatively associated with previous screening (p < 0.05). Older males had higher faecal haemoglobin concentrations and were less likely to have a false positive result at colonoscopy (p < 0.05). High temperature on the sample postage day was associated with reduced haemoglobin concentration and positivity rate (26–35℃: Odds ratio 0.78, 95% confidence interval 0.66–0.93), but was not associated with missed significant neoplasia at colonoscopy (p > 0.05).
Conclusions
Haemoglobin concentrations, and therefore FIT positivity, were affected by factors that vary between screening programmes. Participant demographics and high temperature at postage had significant effects. The impact of temperature could be reduced by seasonal scheduling of invitations. The importance of screening, and following up positive test results, particularly in older males, should be promoted.
Keywords
Introduction
Screening for colorectal cancer (CRC) using faecal immunochemical tests (FIT) for haemoglobin leads to earlier detection of CRC, 1 and reduces incidence by 22%. 2 As positive screening results require further investigation (ie. colonoscopy), test positivity rates have a direct impact on demand for colonoscopy services. 3
Replacing guaiac-faecal occult blood test (gFOBT) with FIT has improved both cancer and adenoma detection.4,5 FIT circumvents many of the gFOBT disadvantages, including the risk of false positive results from upper gastrointestinal bleeding, and dietary intake of red meat, or fruits and vegetables that contain peroxidases, 6 (although colonic bleeding also results from benign non-neoplastic disease). False-positive results lead to unnecessary colonoscopy, with associated risks and potential costs to participants and programmes. 4 Despite the removal of recognized confounding factors that affect gFOBT, FIT screen positive rates vary widely across regions: Australia, 4.6–9.0%,7–10 Korea 7.3–11.2%,4,11 Netherlands 5.5–8.8%,12–14 Italy 3.7%, 15 Germany 5.0%, 16 and USA 2.6%. 17
In addition to the test configuration (ie. number of samples, cut-off haemoglobin concentration for positivity), other factors (ie. participant age, gender, and socioeconomic status mix) might contribute to this variation. Older males are more likely to have a positive screening result.7,8,11,13,14 Ambient temperature and seasonality following sample collection may affect positivity rates, but there have been conflicting findings.13,18–22 As positivity is a surrogate marker for faecal haemoglobin concentration, global variation in positivity can also be related to differences in faecal haemoglobin with the different variables.23–25 Other factors, such as screening round, specimen collection device storage condition, and time until samples are returned for processing may also affect results. While studies have assessed the effect of some of these variables, there has not been a comprehensive study examining the relative contribution of each factor on FIT positivity rates in a combined multivariate analysis. We therefore aimed to investigate how different demographic, pathological, behavioural, and environmental factors might influence haemoglobin concentrations and test positivity rates.
Methods
Study population
The cohort was derived from average-risk population screening and hospital based CRC surveillance programmes provided by the Bowel Health Service (Repatriation General Hospital, South Australia), from August 2008–2013. The population demographics were sufficiently broad to enable assessment of a range of factors that could influence positive rate, and to make the findings generalizable. Age, gender, and home postcode were recorded. Socioeconomic status was determined from postcode using the Index of Relative Socioeconomic Advantage and Disadvantage (Australian Bureau of Statistics), and ranked by quintile (lowest quintile being most deprived). Ethical approval was obtained from the Southern Adelaide Clinical Human Research Ethics Committee. All participants provided written informed consent.
FIT offer and analysis
People were invited by mail to participate in screening each year where appropriate. As there was continuous study enrolment throughout the five years, subjects received between one and five offers for CRC screening. The kit included an invitation letter, instructions, two specimen collection devices (OC Sensor, Eiken Chemical Co. Ltd, Tokyo, Japan), a sample tube pouch, two sample collection sheets, and a reply paid envelope. Participants were asked to collect samples at home from two different bowel motions (avoiding urine contamination), to record the sample dates and storage conditions (room temperature, refrigerator or freezer), and to post the samples to the Bowel Health Service laboratory. Dietary or medicine restrictions were not required. A reminder letter was sent to non-participants at six weeks. Tests not correctly completed (eg. collection was not from two separate bowel motions), or returned to the laboratory more than two weeks after the first sample collection date, were not analysed and a new kit was issued for a repeat test.
Dates of laboratory receipt and analysis were recorded. Time since collection was defined as the number of days between first sample and laboratory analysis. To assess the effect of temperature on test outcome, maximum temperatures on the day of sample postage were obtained for the Adelaide (Kent Town) weather station from the Australian Bureau of Meteorology. 26 Date of postage was estimated to be the day prior to receipt at the laboratory, (unless received on a Monday, when day of postage was estimated as the preceding Friday).
OC Sensor is a quantitative FIT, with chemistry based on human haemoglobin antibody mediated latex agglutination. The sample collection device consists of a serrated probe that holds approximately 10 mg of faeces (collected from the outer surface of the faeces), and contains 2 mL of haemoglobin stabilization buffer. Barcoded specimen collection devices were tested for the presence of haemoglobin using the automated analyser (OC-Sensor DIANA, Eiken Chemical Co. Ltd). The majority of samples (82.5%) were analysed either on the day of return, or the following day. FIT samples not analysed on the day of receipt were stored at 4.0℃ until analysis (median time until analysis = 0 days, range 0–13 days). Prior to analysis, the autoanalyser was calibrated with a standard curve of known haemoglobin concentration, and low- and high-haemoglobin concentration quality control samples were run with each batch to ensure machine accuracy (as per manufacturer instructions). Both FIT samples were analysed once, unless the haemoglobin concentration was above the analytical range (0–200 µg haemoglobin/g faeces), in which case the sample was diluted and re-assayed. Results were recorded electronically. A result was considered positive if either sample contained ≥20 µg haemoglobin/g faeces (corresponding to 100 ng haemoglobin/mL buffer).
Colonoscopy and pathology
Participants with positive FIT results were advised to undergo colonoscopy. Colonoscopy and histopathology results were obtained from 85.1% of positive tests. Outcomes were also ascertained for a sub-group of participants who underwent colonoscopy (86.0% for surveillance purposes) within one year following a negative FIT result. Significant colorectal neoplasia was defined as adenoma with any of the following characteristics: (a) ≥10 mm, (b) >20% villous change, or (c) high grade dysplasia, or carcinoma with invasion beyond the muscularis mucosae. If more than one neoplasm was present, the characteristics of most advanced finding were used for analysis. The location of any significant neoplasia was recorded as distal colon if it was located distal to the transverse colon. A FIT result was considered a false positive if neoplasia was not detected at colonoscopy.
Statistical Analysis
Odds ratios (OR) and 95% confidence intervals (CI) were estimated by multivariate logistic regression, to assess the relative influence of age, gender, socioeconomic status, previous FIT screening participation, and temperature on FIT postage day, on the positive rate. Age, socioeconomic status, and temperature were assessed as categorical variables, with age divided into <50, 50–59, 60–69 and ≥70; socioeconomic status was assessed by quintiles (5 being highest socioeconomic status); and maximum temperature on the postage day was divided into: ≤17℃, 17.1–26℃, 26.1–35℃ and ≥35℃. Sub-group multivariate logistic regression analysis adjusting for colonoscopy outcomes was also performed. An additional sub-group, including the participants who had provided their sample storage conditions, was analysed to calculate OR of a positive FIT result after adjusting for time since collection and storage temperature. As described elsewhere, 13 time between the first sample collection and development was classified as: short (≤3 days), medium (4–6 days), or prolonged (≥7 days). Haemoglobin concentrations were determined for all variables, and compared with Krusall-Wallis non-parametric analysis of variance (ANOVA) or a Mann-Whitney Rank Sum test (for the variable gender). Statistical analyses were carried out using Stata (v13, StataCorp), with p < 0.05 considered significant.
Results
Participant demographics
Over the five year period 13,433 subjects, aged 19 to 92 (median 60.6; 18.8–92.4) and 48.6% male, were offered FIT. Of 34,298 screening packs mailed, 64.2% were completed correctly (n = 21,929; 45.4% male; median age 62.1; 18.8–92.4 y; median number of completed tests per person = 2); 6.1% (n = 1345) were positive.
Multivariate logistic regression of FIT participant demographics, previous screening behaviour, and ambient maximum temperature on day of sample postage, on test positive rate (excluding subjects with significant neoplasia).
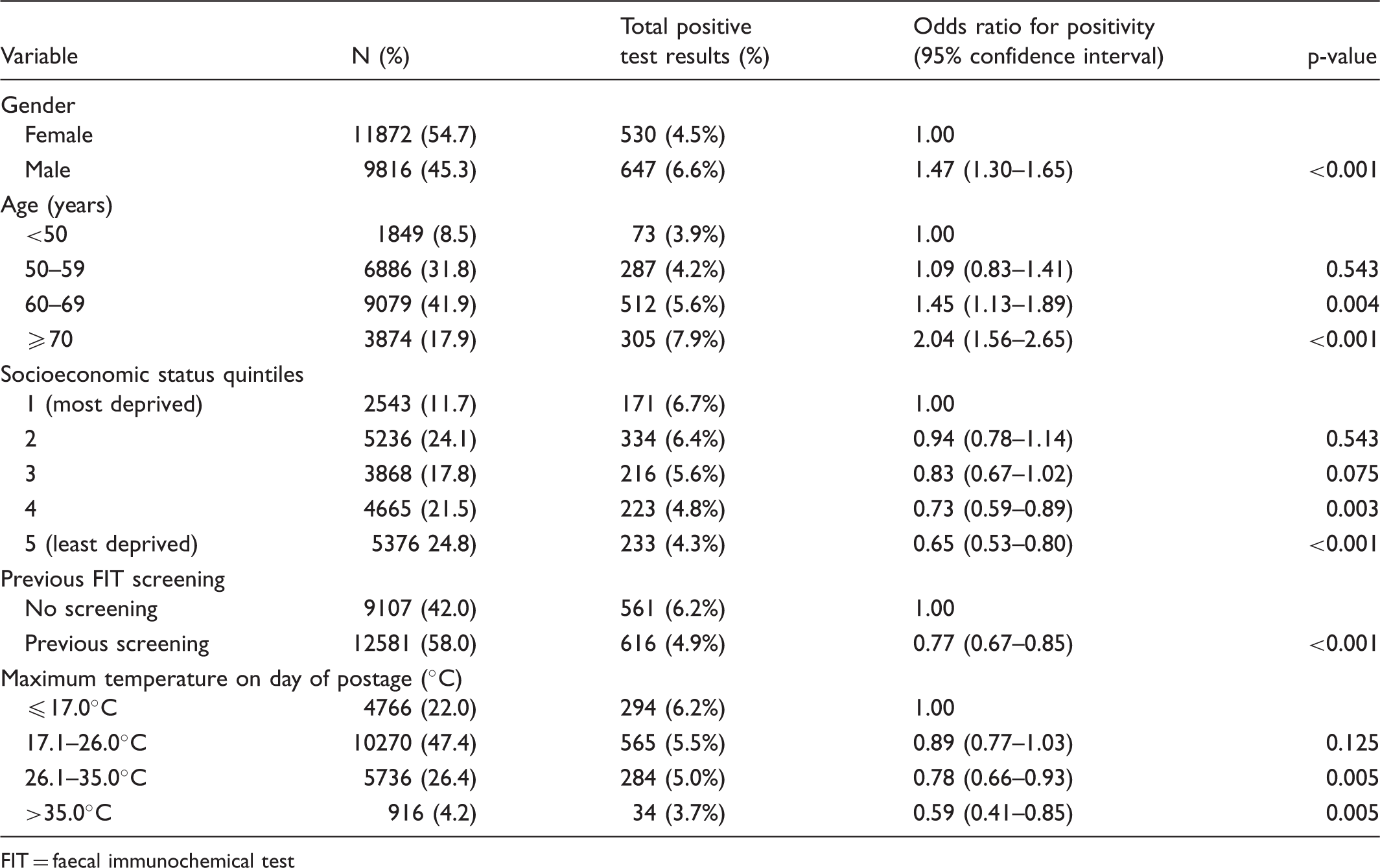
FIT = faecal immunochemical test
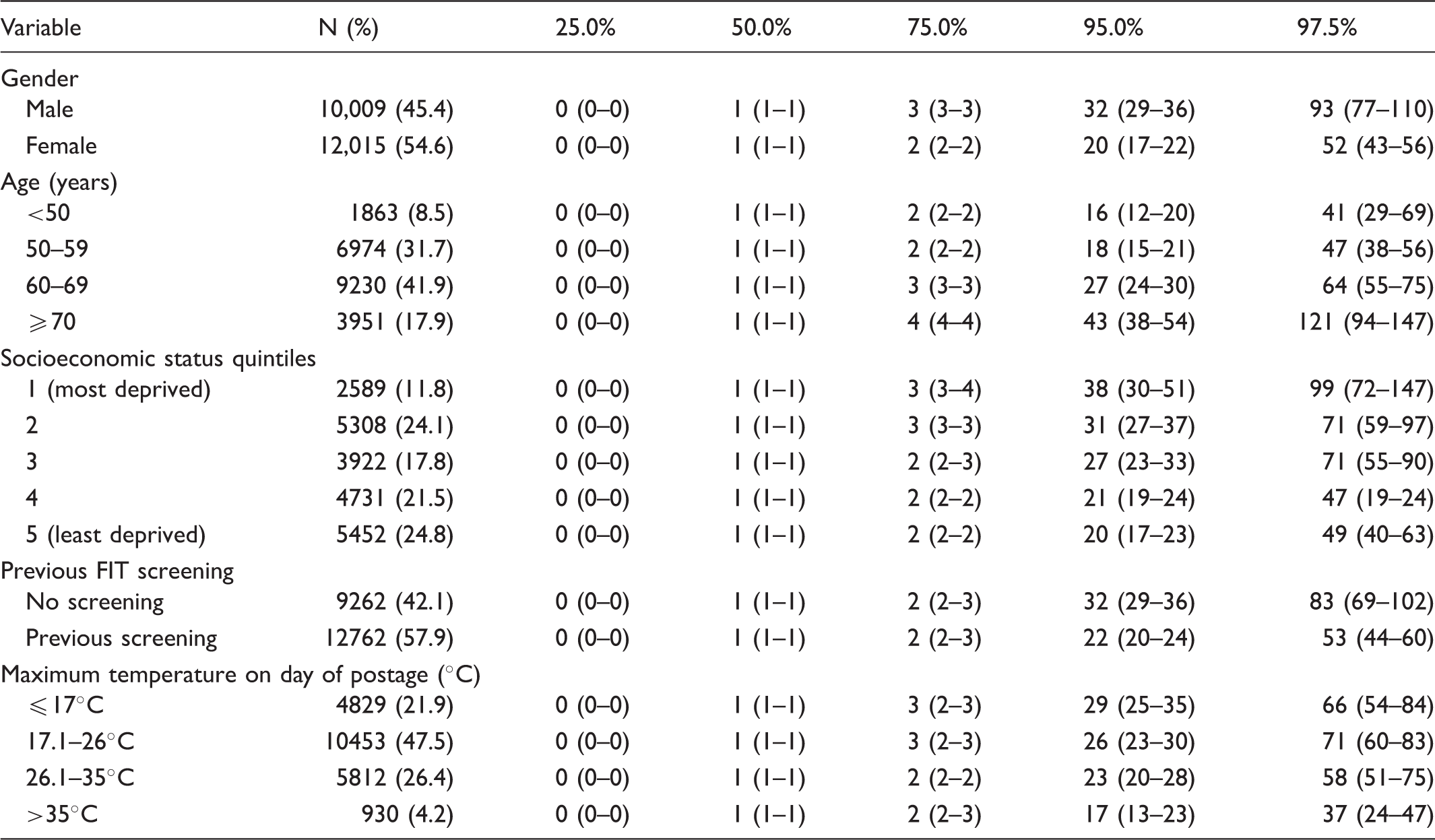
Percentiles (with 95% confidence intervals) of faecal haemoglobin concentrations (µg haemoglobin/g faeces) for participant demographics, previous screening behaviour, and ambient maximum temperature on day of sample postage.
Maximum temperature on postage day
Maximum daily temperature in South Australia ranged from 10.8℃ to 45.0℃ (Figure 1). FIT positivity was lowest in summer (5.2%) and highest in winter (7.5%). Multivariate logistic regression, with adjustment for demographic factors and previous completion of FIT screening, showed that temperature affected test positivity, with lower positive rates occurring when the temperature on the day of postage was greater than 26.0℃ (Table 1). When analysis was repeated with temperature expressed as a continuous variable, a 1℃ increase in temperature decreased the chance of a positive result by 1.8% (OR 0.982, 95% CI 0.973–0.991). Sample collection devices returned during temperatures exceeding 35.0℃ had significantly lower faecal haemoglobin concentration compared with samples returned at lower temperatures (p < 0.001, Table 2).
Monthly positivity rate from completed faecal immunochemical tests (FIT) (n = 21,996) and median daily maximum temperature.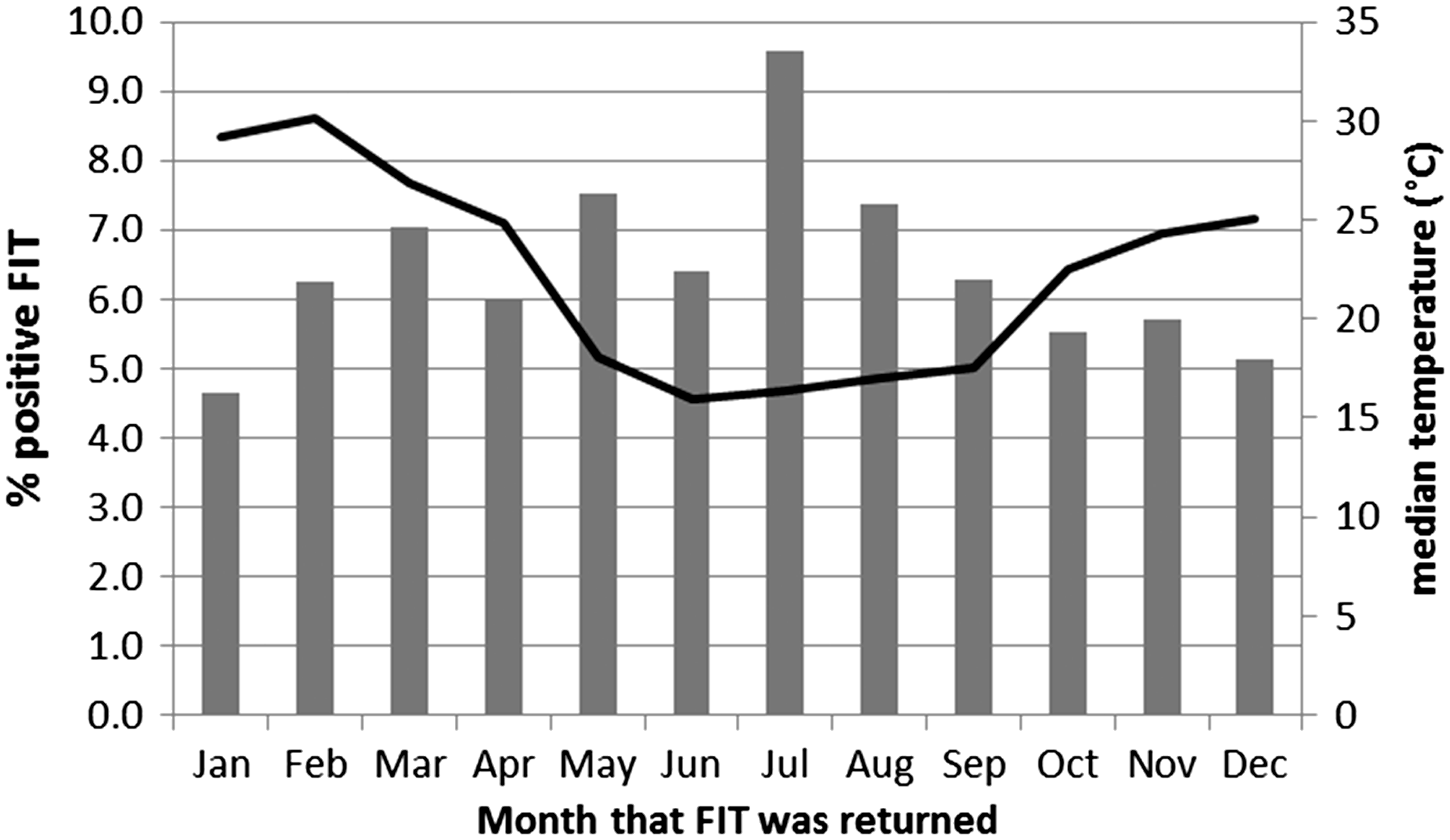
Storage conditions and sample return time
Sample storage conditions prior to mailing the kit were recorded by 8,702 participants, with 61.8% recording storage in the refrigerator, 30.0% at room temperature, and 8.2% in the freezer. Time taken for participants to return their samples after first collection was ≤3 days for 51.5%, 4–6 days for 40.8%, and ≥7 days for 7.7% (median = 3.0 days, range 0–14). Multivariate logistic regression, with adjustments for age, gender, previous screening, and ambient temperature on day of postage, showed that neither storage conditions nor specimen return time affected positivity (p > 0.05).
Colonoscopy outcomes
Multivariate logistic regression of FIT participant demographics and previous screening behaviour on false positive rate (a false positive was defined as the absence of neoplasia at follow-up colonoscopy).
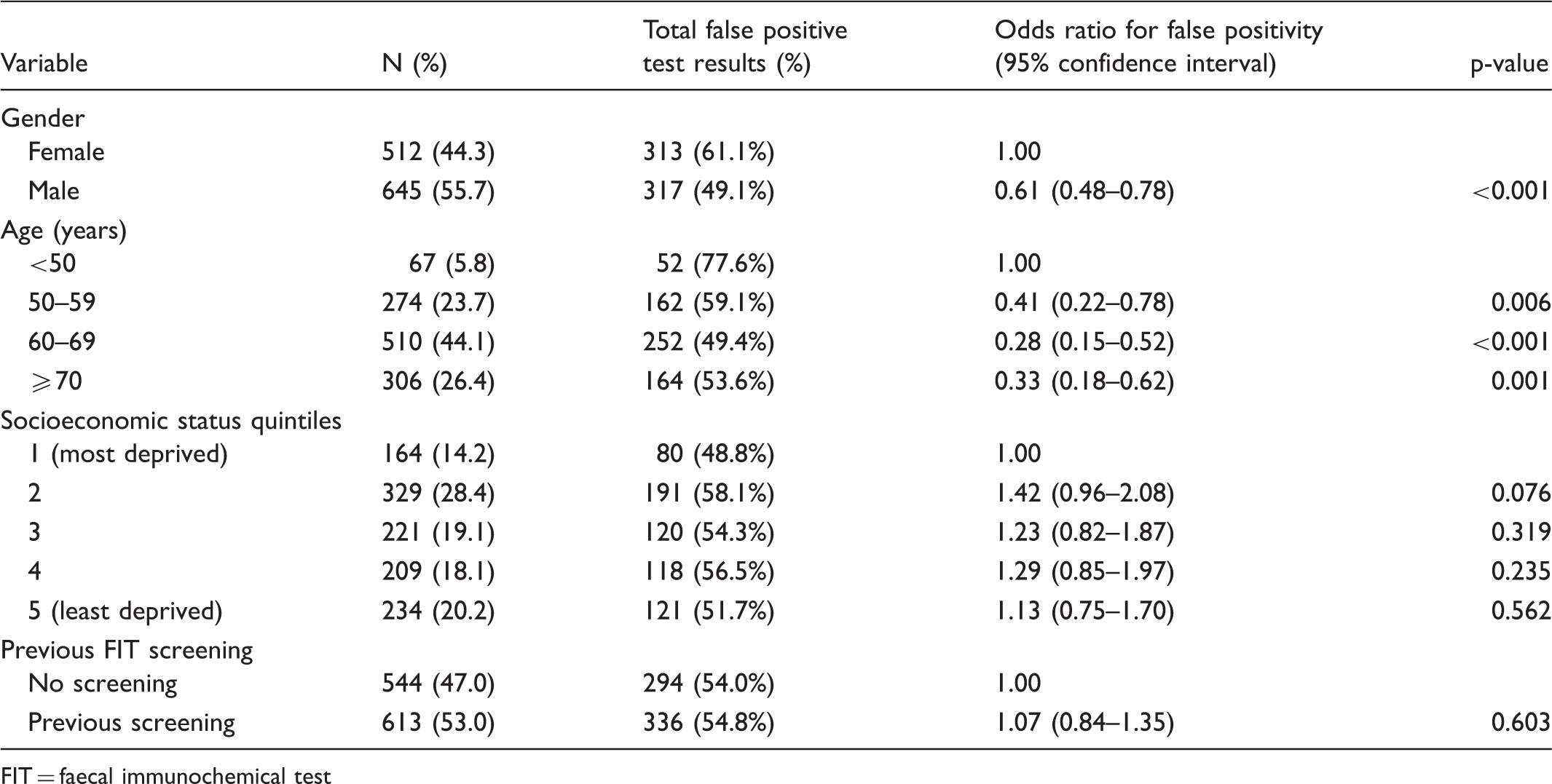
FIT = faecal immunochemical test
Discussion
Marked differences in positivity rates across different programmes make it important to understand the factors that influence FIT outcomes. This is the first study to assess a combination of factors and their relative contributions to FIT outcome. FIT positive rate was independently associated with variables including demographic factors, previous screening behaviour, and temperature, in addition to the presence of colorectal pathology. The presence and degree of impact of these factors could vary between screening programmes, resulting in differing reported positive rates.
Previous studies have reported that increasing age, male gender, and lower socioeconomic status are all significantly associated with FIT positivity.3,11,13,27 We assessed the effect of these factors on test positivity, while correcting for other factors that may also influence test outcome. We found that significance was retained, with each of these variables being an independent predictor of FIT positivity. Older age, male gender, and lower socioeconomic status had the highest positivity rates, with the combination of these high risk factors having a 1.8 times higher likelihood of returning a positive FIT than found in people without these characteristics. Older age groups and males had a lower false positive rate, and therefore increased positivity in this group reflects the increasing incidence of neoplasia with age.8,28 It is concerning that the lowest participation rates for FIT screening occur in males and those who are more socioeconomically deprived.8,14,27,29
We also found that increased positivity reflects higher faecal haemoglobin concentrations within these demographics. Similar findings have been reported with elevated haemoglobin concentrations in males, lower socioeconomic status groups, and in older ages.23–25 The reasons are not certain, but are possibly due to biological differences between the groups. Global differences in measured faecal haemoglobin concentrations have also been reported. 24 Our data could contribute to establishing individualized positivity cut-off haemoglobin concentrations for different demographics.
Environmental factors may also influence FIT positivity. Studies in Italy and the Netherlands have reported lower positive rates in winter compared with summer,13,18–20 but a small study in the Netherlands found no seasonal influence, 22 while a study in Korea found lower faecal haemoglobin concentrations in summer, but no change to overall positivity rate. 21 The relationship between positivity and temperature may become more marked above 20℃. 19 The average summer temperature in South Australia is 28℃, providing an excellent opportunity to explore the effect of temperature relative to other variables. Following adjustment for these other variables, test positivity was reduced at higher temperatures, and was associated with significantly lower haemoglobin concentrations, indicating degradation of the haemoglobin within the sample collection devices. One limitation of our analyses is that we used a maximum temperature estimate based on Bureau of Meteorology data, but the specimens were probably exposed to much higher summer temperatures while being held in a post box prior to postal collection.
Seasonal variation in FIT positivity may also affect detection of significant pathology. There are conflicting findings regarding the detection of advanced neoplasia in different seasons,13,18,20,22 and with another study reporting no seasonal effect. 21 We found that temperature did not influence detection of significant neoplasia, however, detection of low risk adenoma may be affected, as these lesions are typically found to have a haemoglobin concentration just above the cut-off concentration for positivity. 30
The success of a screening programme relies greatly on participation. Screening downstages CRC 1 and, therefore, having previously completed screening with FIT would be expected to reduce the likelihood of a positive subsequent screening result, however this was unclear from previous studies. One study found that positive rate was not influenced by the number of screening rounds, but this study included only data from two screening rounds. 12 Two larger studies found a 27–35% lower positive rate if participants had previously undergone screening.2,13,19,20 Participants in our study had been offered up to five FIT screening rounds, and we found a similar level of reduction of test positivity (OR 0.73, 95% CI 0.65–0.81). Faecal haemoglobin concentration was also lower in those with previous screening. This may be explained by the finding that multiple rounds of screening (with follow-up colonoscopy for positives) should detect and treat those with bleeding neoplasia, or remove the benign bleeding conditions from the screening programme. 15
Screening programme effectiveness also relies on test accuracy. As expected, we found that a positive FIT result was a predictor for significant neoplasia. Taking into consideration the neoplasia risk factors of age and gender, we found that FIT positivity was influenced by neoplasia location, with a distal significant neoplasia more than two-fold more likely to result in a faecal haemoglobin concentration above 20 µg/g faeces. Other studies have also reported that FIT is less sensitive for right-sided neoplasia,11,12,15 which could be due to a different biology of right-sided lesions, due to haemoglobin degradation during transit through the colon, or because haemoglobin is less likely to be on the outer sampled surface of the faeces.
FIT positivity is based on the detection of faecal haemoglobin above a set cut-off concentration, but it is not neoplasia specific, and FIT may detect blood from any lower gastrointestinal source, potentially producing positive results for participants with conditions including haemorrhoids and inflammatory bowel disease. Data from the Australian National Screening Program indicate that 43% of findings following a positive FIT are non-neoplastic. 8 Other research shows that false positive rates may increase with age in men. 31 Conversely we found that false-positives were more likely in younger participants and females. One other study has also reported higher false positive rates in females, 32 but this is an area that requires further investigation to optimize screening programme performance.
Conclusions
A number of factors independently influence FIT positivity rates, and may explain differences between screening programmes across the world. We found that the positivity rate is higher in males, older age groups, and in those of lower socioeconomic status, with older males less likely to have a false positive result. These findings support a need to promote CRC screening in certain demographics, especially as older age and lower socioeconomic status are also associated with more advanced cancer stage at diagnosis. 1 While it is clear that the presence of significant neoplasia increases the chance of a positive FIT, demographic factors confer a similar risk. We have also shown that in a region with high summer temperatures, haemoglobin concentrations and positivity rates fall independently of the effect of all other variables. Therefore in any programme that involves return of specimen collection devices via mail, screening should not be undertaken in the summer months unless the sample buffer is proven to stabilize haemoglobin.*
Footnotes
*
As of 2013, the manufacturer changed the OC Sensor sample buffer formulation to improve sample stability.
Declaration of conflicting interests
The authors have no competing interests to declare.
Funding
Faecal immunochemical tests for the studies were subsidised by Eiken Chemical Co., Japan. Parts of this research were supported by a project grant from NHMRC Australia (ID# 480428).