
Abstract
Objectives
Changes in the prevalence of faecal occult blood test positivity over time have not been previously reported, but could have important implications. This study examined the positivity of the initial guaiac faecal occult blood test, a surrogate marker for colorectal bleeding, in participants aged 50 in a national bowel screening programme.
Methods
Data from the Scottish Bowel Screening Programme were used to study the initial positivity of the guaiac faecal occult blood test between 2007 and 2017. Positive predictive values of the testing process for colorectal cancer and adenoma were assessed over the same time period.
Results
Across Scotland, the initial guaiac faecal occult blood test positivity increased from 4.1 to 10.8%. In NHS Grampian and NHS Fife, two of the three NHS Boards which began roll-out of screening in 2007, it increased from 4.0 to 10.9%. In the Scottish Bowel Screening Programme, the positive predictive value declined from 11.0 to 6.6% for colorectal cancer and increased from 31.6 to 39.8% for adenoma.
Conclusions
In the Scottish programme over a decade, initial guaiac faecal occult blood test positivity increased in participants aged 50. This may be associated with changes in lifestyle and might have implications for screening clinical outcomes, including positive predictive value.
Introduction
In many countries, regular testing for the presence of occult blood in faeces is used for colorectal cancer (CRC) screening, 1 but how the prevalence of detectable blood in faeces changes over time has not been rigorously documented. This is important for several reasons. First, if there is a change in the background prevalence of faecal occult blood test positivity, this could have an impact on the positive predictive value (PPV) of screening using this modality. Second, changes in test positivity have implications for service provision in terms of endoscopy capacity. Third, we have recently shown that a positive guaiac faecal occult blood test (gFOBT) result is associated with premature mortality from all causes, independent of its association with risk of death from CRC, 2 so changes in gFOBT positivity may act as an index of possible changes in mortality. To assess changes in gFOBT positivity, this study examined the results of the initial gFOBT, a surrogate marker for colorectal bleeding, over a decade in participants aged 50 in a national bowel screening programme.
Methods
In Scotland, CRC screening using gFOBT as the first-line investigation was piloted over three screening rounds in three NHS Boards (Tayside, Grampian, and Fife) from 2000 to 2007. The Scottish Bowel Screening Programme (SBoSP) was rolled out to the rest of Scotland between June 2007 and December 2009. The algorithm used in the SBoSP differed from those used in the pilot screening rounds (details described elsewhere 3 ). In simple terms, it consisted of an initial gFOBT where the invitees were asked to provide a total of six faecal samples (two from each of three separate bowel movements) on cards with a window for each sample, followed by a card-based qualitative faecal immunochemical test for haemoglobin (FIT) if one to four windows gave a positive result on the initial gFOBT, a ‘weak positive’ result. If five or six windows were positive on the initial gFOBT, or the qualitative FIT was positive, colonoscopy was offered immediately. This two-tier reflex gFOBT/FIT algorithm continued until November 2017, when it was replaced by a single faecal sample quantitative FIT. 4 All samples were analysed in the Scottish Bowel Screening Laboratory, which holds ISO 15189 accreditation. The Laboratory performed comprehensive internal quality control, including assessment of individual screener staff performance, both analytically and through monitoring of positivity reported. As gFOBT requires visual interpretation of the colours on the test card, all positive test results were confirmed by a second screener. External quality assessment was undertaken through participation in the United Kingdom National External Quality Assessment Scheme. Acceptance quality checks were undertaken for all new manufacturing lots of gFOBT and FIT. 5 There were no significant changes in the testing processes, faecal test characteristics, or gFOBT manufacturer and supplier, from 2000 to 2017. The instructions given to participants did not change during the study; no dietary restrictions (including vitamin C intake), nor cessation of medicines such as non-steroidal anti-inflammatory drugs and anti-coagulants, were advocated.
Estimation of changes in gFOBT positivity over time using data from the SBoSP is not straightforward. First, if all results were used, the data would comprise a mixture of prevalence (first time) and incidence (repeat) screening from participants of a range of ages between 50 and 74, the proportions of which change over time. As it is known that the gFOBT positivity in incidence screening is less than that of prevalence screening 6 and increases with age, 7 it would be difficult to disentangle these effects from a true change in gFOBT positivity in the whole population accepting screening. Second, as the SBoSP was being rolled out between 2007 and 2009, and the effect of adding a screening naive NHS Board takes two years (a single screening round) to be complete, the screened population has only been geographically stable since the end of 2011. Because the gFOBT positivity varies considerably between NHS Boards, 8 possibly as a result of varying degrees of socio-economic deprivation, this adds another effectively uncontrollable variable. Third, the final result in the context of the SBoSP up until November 2017 is derived from an algorithm that, by design, cuts-down the overall positivity and minimizes false positive results by excluding a high proportion of those participants who exhibit lower (weak) degrees of positivity on the initial gFOBT (only a small proportion of those with one to four windows positive on this initial gFOBT have a positive FIT result 3 ). Because of this, using the overall final result of the screening algorithm to assess variation in gFOBT positivity over time would underestimate any changes.
For these reasons, this study examined the overall positivity of only the initial gFOBT, not the final positivity of the overall screening algorithm, that is the positivity in those who had any one or more windows positive, but only in participants aged 50. This ensured that all subjects in this study were the same age and were undergoing only prevalence screening. This initial gFOBT positivity was determined for every year from 2007 to 2017 for the whole of Scotland and, to eliminate the possible effect of adding different NHS Boards during roll-out of the SBoSP, an additional analysis was carried out, restricted to NHS Grampian and NHS Fife. Along with NHS Tayside, these two NHS Boards were the first to participate in the roll-out of the SBoSP in 2007, having taken part in the three pilot screening rounds from 2000 to 2007. 6 However, NHS Tayside performed an evaluation of quantitative FIT as the first-line screening test between 1 July 2010 and 31 December 2010, 9 and was therefore excluded from the analysis because, during this time, this could have introduced a spurious fluctuation in positivity.
The data for these analyses were obtained from the Bowel Screening Database held by the Information Services Division of National Services Scotland. Data from the pilot screening rounds could not be studied, as the overall positivity rate of the initial gFOBT was not recorded; only the final outcome of the screening algorithms used in these three rounds was available. Formal ethical approval for the study was not required because individual participants were not approached, and only routinely collected data were used. These data can be requested via the Information Services Division’s Electronic Data, Research and Innovation Service (
Results
For the whole of Scotland, there was a steady rise in gFOBT positivity (i.e. any positive window on the initial gFOBT card) in participants aged 50, from 4.1% (95% confidence intervals (CIs): 3.7–4.6) in 2007 to 10.8% (95% CI: 10.3–11.3) in 2017 (Figure 1). In NHS Grampian and NHS Fife (Figure 2), a similar rise was seen, from 4.0% (95% CI: 3.5–4.6) to 10.9% (95% CI: 9.7–12.1). As evidenced by the wide separation of the higher CIs for the 2007 data and the lower CIs for the 2017 data, these differences were highly statistically significant (p < 0.00001 by X2 testing in both instances). Positivity rates for women were lower than those for men, as has been found previously overall in the SBoSP, 7 although these did converge in 2017 in NHS Grampian and NHS Fife.
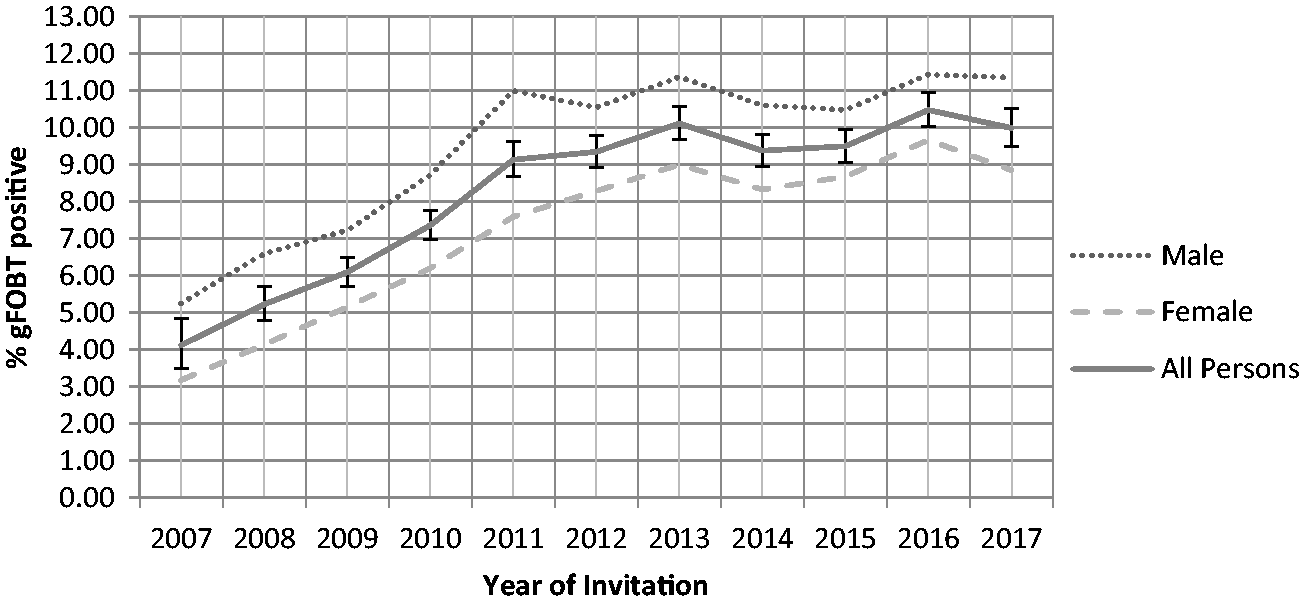
Change in the positivity of the initial gFOBT participants aged 50 in the SBoSP between 2007 and 2017 for the whole of Scotland (X2= 305.6, p < 0.00001).
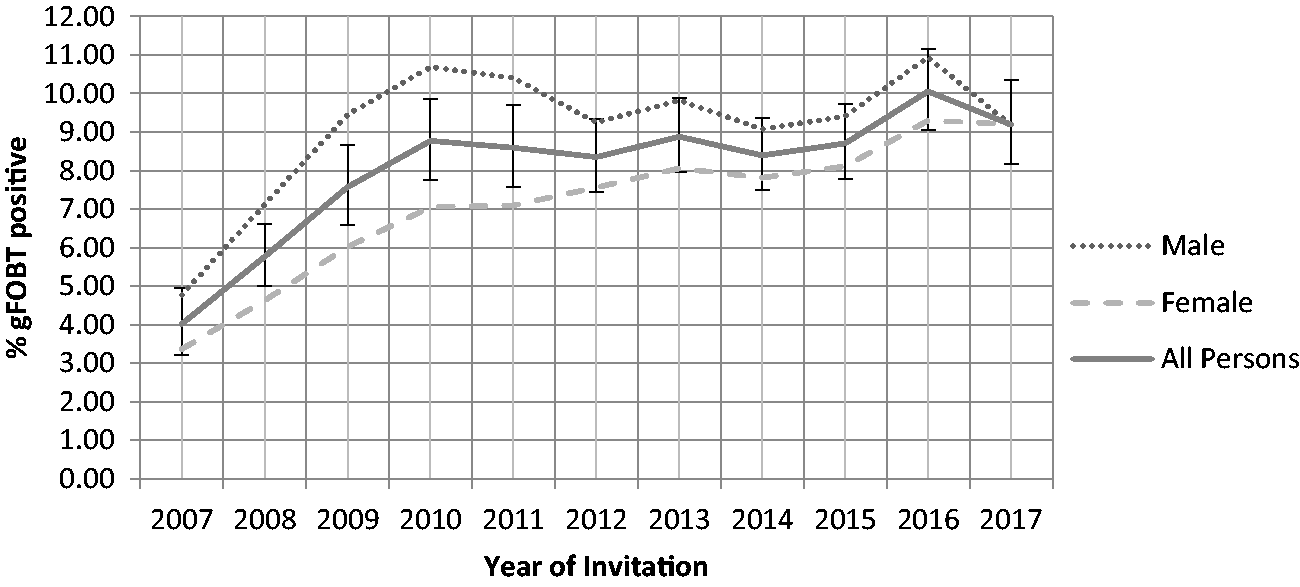
Change in the positivity of the initial gFOBT in participants aged 50 in the SBoSP between 2007 and 2017 from NHS Grampian and NHS Fife Boards only (X2= 115.1, p < 0.00001).
For completeness, the final results of the screening algorithm (derived from the gFOBT/FIT two-tier reflex approach) were also examined; the positivity in those aged 50 for the whole of Scotland increased from 0.68% (95% CI: 0.53–0.88) to 1.6% (95% CI: 1.4–1.7) (p < 0.00001 by X2 testing) between 2007 and 2017. This supports the view that the rise in initial gFOBT positivity was due to the presence of occult blood in faeces, and not to other moieties, as these would not be detected by the qualitative FIT used to determine the need for further investigation in those participants with one to four windows (weak) positive, because the qualitative FIT used is based upon the reaction with antibodies specific to the globin moiety of human haemoglobin.
As a change in background gFOBT positivity could affect the PPV for neoplasia, the PPVs for both CRC and adenoma over time were also examined. By necessity, this had to be calculated on the basis of those who had a final positive test result based on the whole screening algorithm, but as described in the preceding paragraph, the positivity derived in this way has also increased during the study period. Between 2007 and 2017 the PPV for CRC fell from 11.0 to 6.6% (p < 0.00001 by X2 testing) (Figure 3), and for adenoma it increased from 31.6 to 39.8% (p < 0.00001 by X2 testing) as shown in Figure 4.
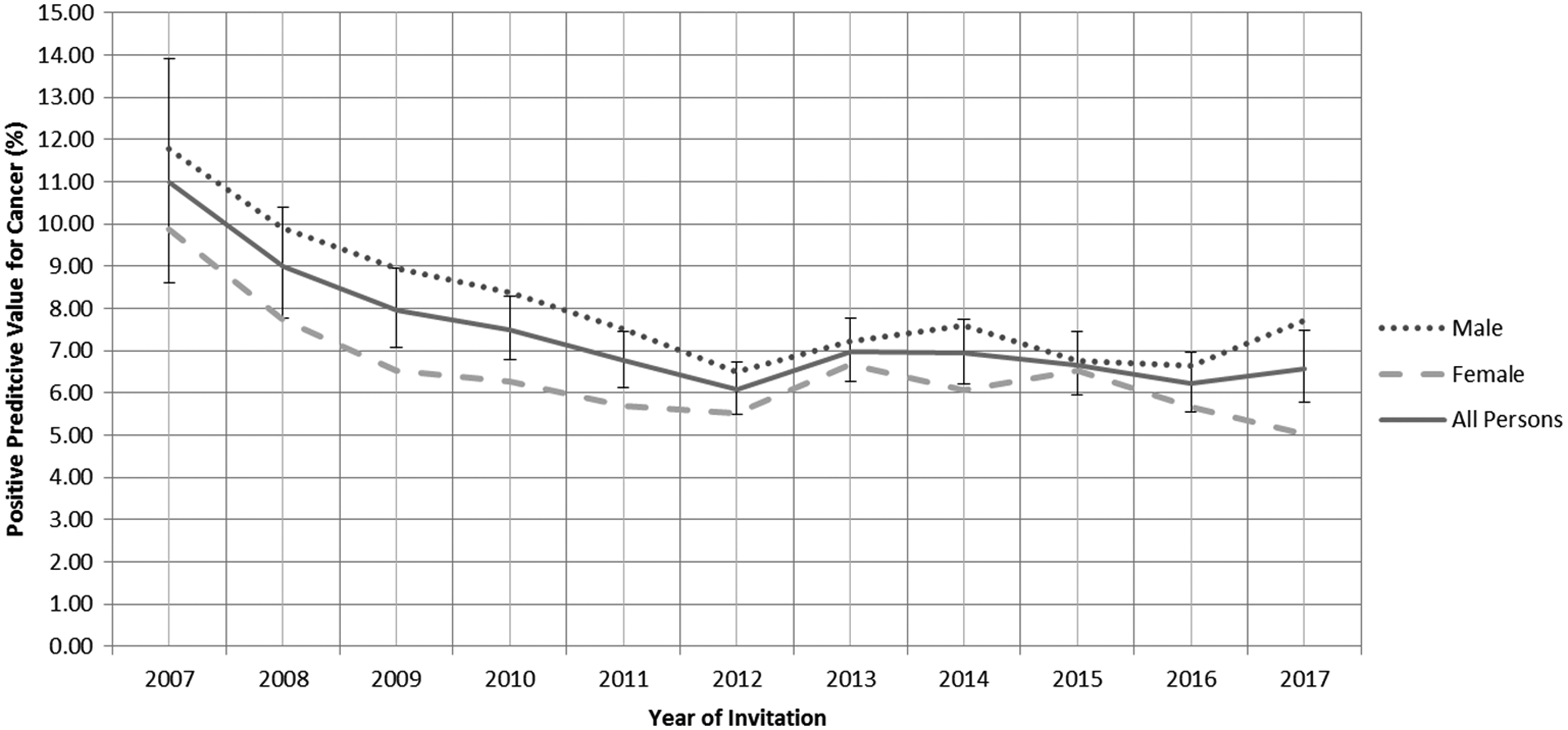
PPV for CRC in the SBoSP between 2007 and 2017 (X2=24.8, p < 0.00001).
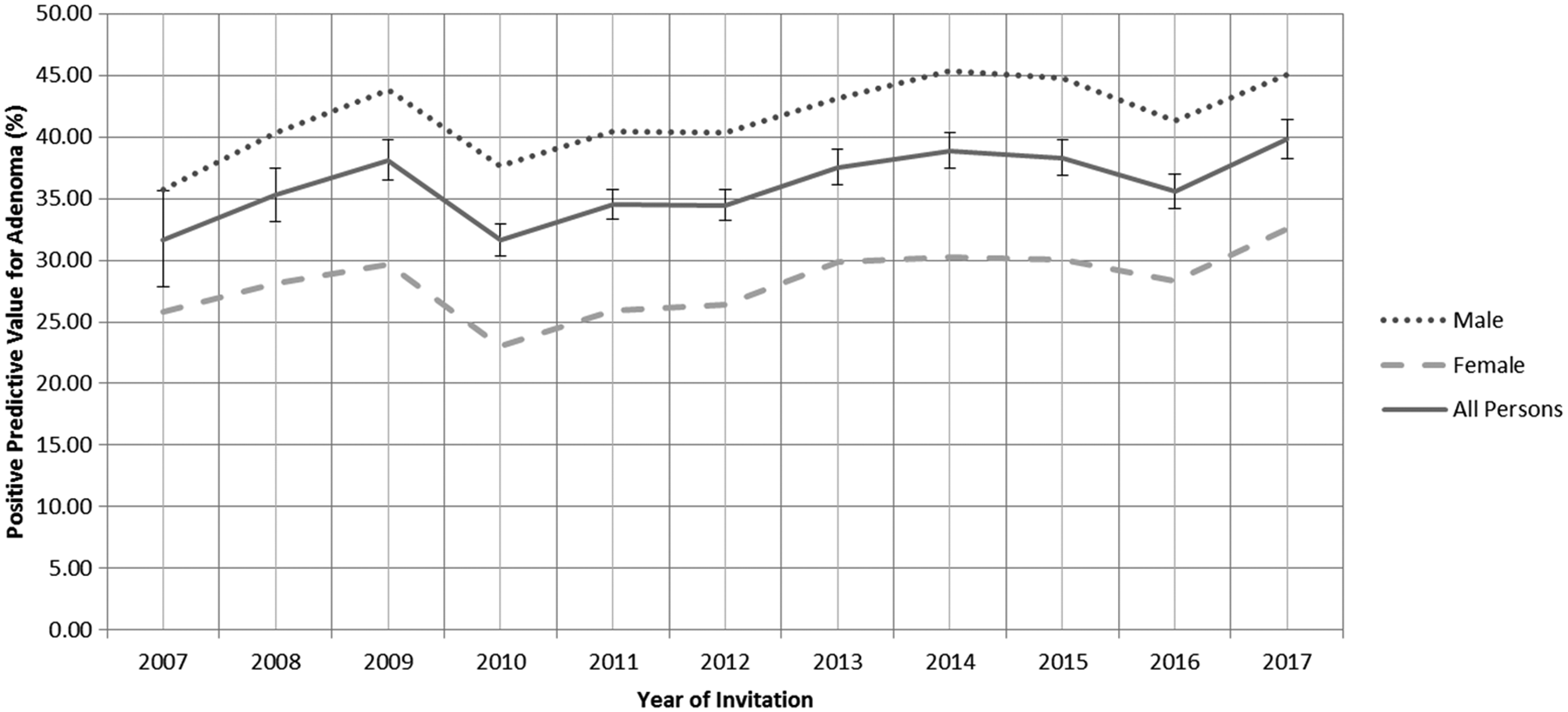
PPV for adenoma in the SBoSP between 2007 and 2017 (X2=23.4, p < 0.0001).
Discussion
To our knowledge, this is the first time that the change over time of faecal occult bleeding, as inferred from initial gFOBT positivity, has been reliably investigated. It is true that gFOBT provides an indirect measure of gastrointestinal, particularly colorectal, bleeding, as it is based on a chemical reaction that can give false positive results from peroxidase containing materials in the diet, and dietary restriction was not mandated in the SBoSP. However, there is evidence that, when gFOBT cards are allowed to dry for some days prior to development in the laboratory, as was the case in the SBoSP, such dietary effects are negligible.10,11
Using FIT would clearly provide a more secure estimate of the presence of occult blood in faeces, but there are no screening programmes using this approach that are of sufficient duration to study the change in faecal haemoglobin concentration over time. However, this will be interesting to study in the future, both in the nations of the UK and other countries, especially as FIT is now replacing gFOBT worldwide.
The reason behind this highly likely increase in faecal occult bleeding in the population studied is not clear, but it is noteworthy that our recent study of gFOBT results and all-cause mortality showed that a positive gFOBT result was associated with an increase in all-cause mortality, in all non-CRC mortality, and in death from a variety of chronic conditions including cardiovascular disease, respiratory disease, and cancer excluding CRC. 2 This study demonstrates that this effect was independent of medicines that could cause bleeding, such as anti-coagulants, aspirin, and other non-steroidal anti-inflammatory medicines, and the hypothesis was generated that a positive gFOBT result, implying gastrointestinal bleeding, might reflect systemic inflammation caused by factors predisposing to ill health, such as obesity,12,13 sedentary behaviour,14,15 smoking, 16 alcohol dependence, 17 and a ‘Western’ diet.18,19
The rise in initial gFOBT positivity seen in the 10-year interval between 2007 and 2017 could be related to changing lifestyle factors. Trends data from the Scottish Health Survey from 2008 to 2017 report less than ideal levels of physical activity, fruit and vegetable intake, alcohol, smoking, and obesity in adult men and women aged 45–54. 20 It is notable that the only lifestyle risk factor which has increased during this time in this age group is obesity (from 30 to 36% prevalence in men and 29 to 34% prevalence in women) which, given that physical activity has increased, implies that caloric intakes have increased. Obesity per se is associated with increased inflammation and changes in the microbiota, 13 which might in turn influence gFOBT results. It is also of note that, in Scotland, average life expectancy is beginning to decline, 21 which is in keeping with our observations.
The hypothesis that faecal haemoglobin concentrations are a reflection of systemic inflammation could be addressed by carrying out a similar study using faecal calprotectin, or possibly other markers of inflammation, but this is impractical given the time scales involved. Notably, in our study of gFOBT positivity and all-cause mortality, a number of non-neoplastic causes of death known to be associated with systemic inflammation were also associated with a positive gFOBT result. 2
Quite apart from any public health implications of this observation, an increase in the background rate of faecal occult bleeding that is unrelated to the incidence of CRC could have an impact on the overall performance of a population-based CRC screening programme predicated on the detection of the presence of occult blood in faeces, through decreasing the PPV of the test result. The PPVs of final test results for both CRC and adenoma have been key performance indicators since the beginning of the SBoSP. 7 Examination of the PPV for CRC over time demonstrated a decline between 2007 and 2017 from 11.0 to 6.6%, leading to a small decrease in cancer detection rate in those with a final screening test result, 7 albeit accompanied by an increase in overall uptake, as has been described in detail. 22 This could be explained by a decrease in the ratio of prevalence to incidence screening episodes, or changes in colonoscopy quality, although in Scotland, as we have described, 23 no new measures were introduced to improve or audit colonoscopy performance throughout the study periods. An increase in background population gFOBT positivity is an alternative or additional explanation, and this could be interpreted as an inherent weakness of this approach to screening.
The PPV for adenoma increased between 2007 and 2017 from 31.6 to 39.8%. This is in keeping with the hypothesis that adenomas are detected by tests for the presence of occult blood in faeces, not simply because they bleed, but because chronic inflammation is involved in the initiation of the neoplastic process, so that adenomas tend to arise in a sub-clinically inflamed colon. If this is the case, an increase in faecal occult bleeding in the population might signal an increase in the incidence of colorectal adenomas. Thus, testing for the presence of occult blood in faeces might prove to be an effective means of finding adenomas that will take account of changes in incidence, especially if the faecal haemoglobin concentration threshold for triggering a colonoscopy from quantitative FIT is lowered. This, in turn, could enhance the ability of screening programmes to prevent the development of invasive CRC by interrupting the adenoma–carcinoma sequence.
Conclusion
Over the studied decade, initial gFOBT positivity increased in participants aged 50 in the SBoSP. This may be associated with changes in lifestyle, and might have implications for screening clinical outcomes, including PPV.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NHS Tayside, through Callum G Fraser, had a paid consultancy contract with Immunostics Inc., Ocean, NJ, USA, the suppliers of gFOBT and qualitative FIT. All other authors declare no interests.
Funding
The author(s) disclosed receipt of the financial support for the research, authorship and/or publication of this article: Scottish Government. The views expressed are those of the authors.