
Abstract
Objectives
To establish the reliability and validity of an automated hearing screening test system for preschoolers and to investigate the risk factors for hearing loss.
Methods
The study used a cross-sectional design in a comparative study of subjects. The automated hearing screening test was performed in 6231 preschoolers (3–7 years old) from 41 kindergartens in Shanghai, China. Sensitivity and specificity of the automated test were investigated with subjects who failed the screening test and a group of control subjects.
Results
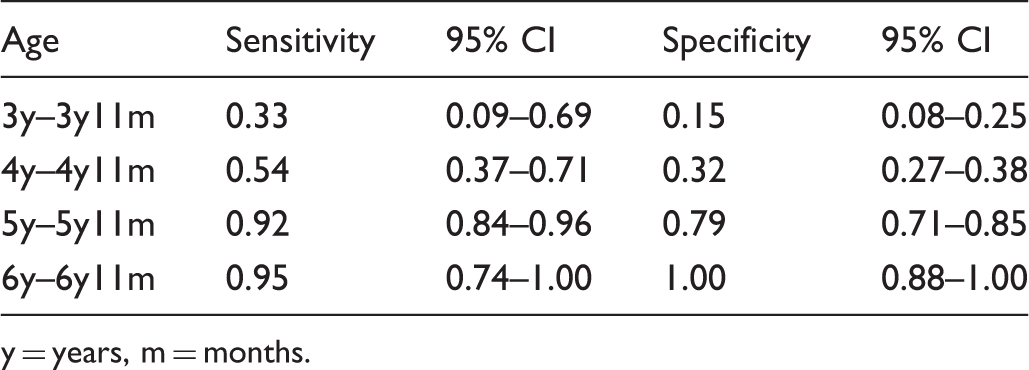
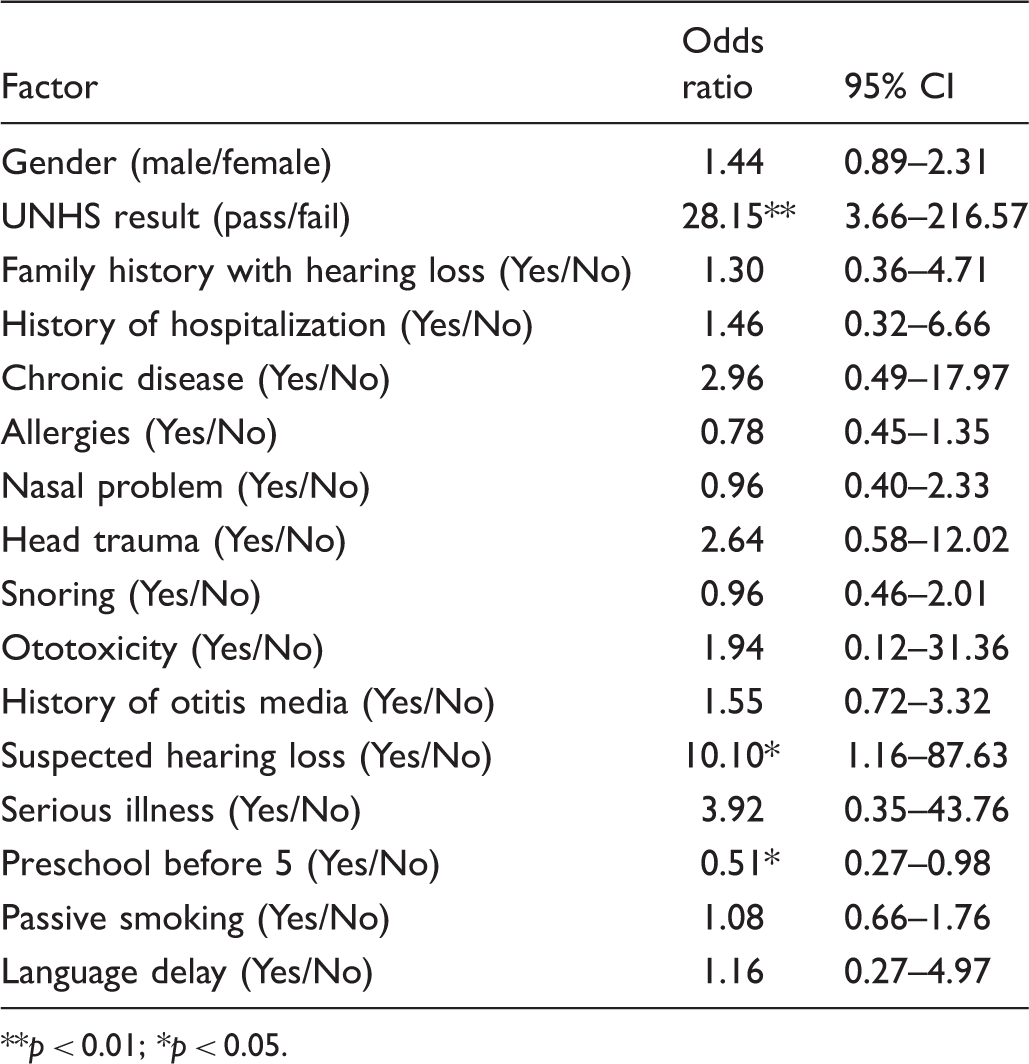
Six hundred and forty-seven children were referred for diagnostic audiological assessment after the automated pure-tone screening test. Using the conventional pure-tone audiometry as the “gold standard,” the sensitivity and specificity of the automated hearing screening test increased from 0.33 and 0.15 in the youngest age group to 0.95 and 1.00 in the oldest age group, respectively. There was no statistically significant gender effect, but there was an age effect (χ2 = 22.96, p < 0.01). In the univariate analysis of 104 cases and 201 controls, significantly elevated odds ratios (OR) for hearing loss were correlated with universal newborn hearing screening test results (OR = 28.15, p < 0.01), parental suspicion of hearing loss (OR = 10.10, p < 0.05), and attendance at preschool before the age of five (OR = 0.51, p < 0.05).
Conclusions
The results suggest that the automated hearing screening test system can be used in screening programmes for preschoolers aged older than five years.
Introduction
Early identification of children with hearing loss has been made possible with the implementation of newborn hearing screening tests. Continued screening for preschool- and school-aged children can help to identify children with progressive or late-onset hearing impairment. The American Academy of Pediatrics recommends newborn hearing screening and periodic hearing screening for every child through adolescence. 1 Among the available audiometric screening tools, such as the pure tone test, otoacoustic emission test (OAE), auditory brainstem response (ABR), tympanometry, and questionnaires, the pure tone test has been considered the gold standard in hearing screening for children.2–8 However, young preschool children may have difficulty in understanding the instructions of the pure-tone test and their attention spans may be too limited to complete the test.9–10
We used a previously developed automated pure-tone hearing test system 11 composed of a tablet computer and a pair of noise-cancelling headphones that help to control the ambient noise levels common in schools. The hearing test is incorporated into an interactive listening game designed to engage children’s attention. A previous study showed that the automated test could be implemented in school hearing screening programmes in places where professional audiological support is scarce. 11 This study further investigates the validity and feasibility of using the system to conduct hearing screening programmes in kindergartens.
Subjects and methods
Subjects
The subjects were children recruited from 41 kindergartens in Yangpu District, Shanghai, one of China’s urban districts. All 96 kindergartens in the district were invited to join the study; 41 chose to participate. The subjects were recruited on a voluntary basis and written consent was obtained from parents before the testing.
Equipment and test setting
Automated hearing screening test
The automated hearing screening test was developed and written in Java. The hearing test was administered on a tablet computer (Samsung Galaxy Tab 7.7) with headphones (a pair of Bose QuietComfort® 15 Acoustic Noise Cancelling® headphones) as the transducer for testing. Details of the automated hearing screening system, including the calibration of the system and the adapted screening procedures, have been previously described. 11 The system tests three frequencies (1000, 2000 and 4000 Hz) as recommended in the most commonly adopted testing guidelines. 2 Continuous pure-tones for each of the test frequencies were first presented on the right side. If a threshold higher than 30 dB HL was obtained at any tested frequency in either ear, the test result would be regarded as “initial refer”, and an immediate rescreen with the same test system would be done to confirm the result. If the subject passed the rescreen, the overall result would be regarded as “pass”. Otherwise, the test result would be regarded as “refer”, indicating that the subject should be referred for professional assessment.
Nurses who had received two hours of training on the use of the automated screening system acted as facilitators and monitored the automated testing. The tests were conducted in quiet rooms in the kindergartens, with an ambient noise level ranging from 40 to 51 dBA. During the conditioning phase, some introductory pictures were displayed on the tablet while the facilitator explained the test to the subject and ensured that they understood the task. During the testing phase, no cues were provided and only neutral acknowledgements (such as nodding and praising for the child’s effort) from the facilitator were allowed.
Diagnostic audiological assessment
Children who failed the automated rescreening were subsequently referred for a diagnostic audiological assessment, carried out in sound booths in the Shanghai Children’s Hearing and Speech Centre. Five percent of the children who had passed the automated screening test were also referred for a diagnostic assessment as controls. The diagnostic assessment included an otoscopy, tympanometry, distortion product otoacoustic emissions test, and standard pure-tone audiometry or play audiometry.
Air-conduction thresholds were obtained at 0.25, 0.5, 1. 2. 4 and 8 kHz according to ANSI S3.6-2004 testing guidelines. 12 Bone-conduction thresholds at 0.5, 1, 2 and 4 kHz were also obtained. The equipment used was a Madsen Conera clinical audiometer with Telephonics TDH-39 headphones, a GSI Tympstar middle ear analyzer and a Madsen Capella OAE system. The parents of the subjects who underwent the diagnostic test were asked to fill in a questionnaire asking about medical history and other risk factors for hearing loss.
Follow-up arrangement
Hearing screening reports on all of the tested children were provided to the schools and parents within one week of the screening. Further audiological and medical follow-up procedures were recommended according to the results of the diagnostic test.
Results
Subject demographics
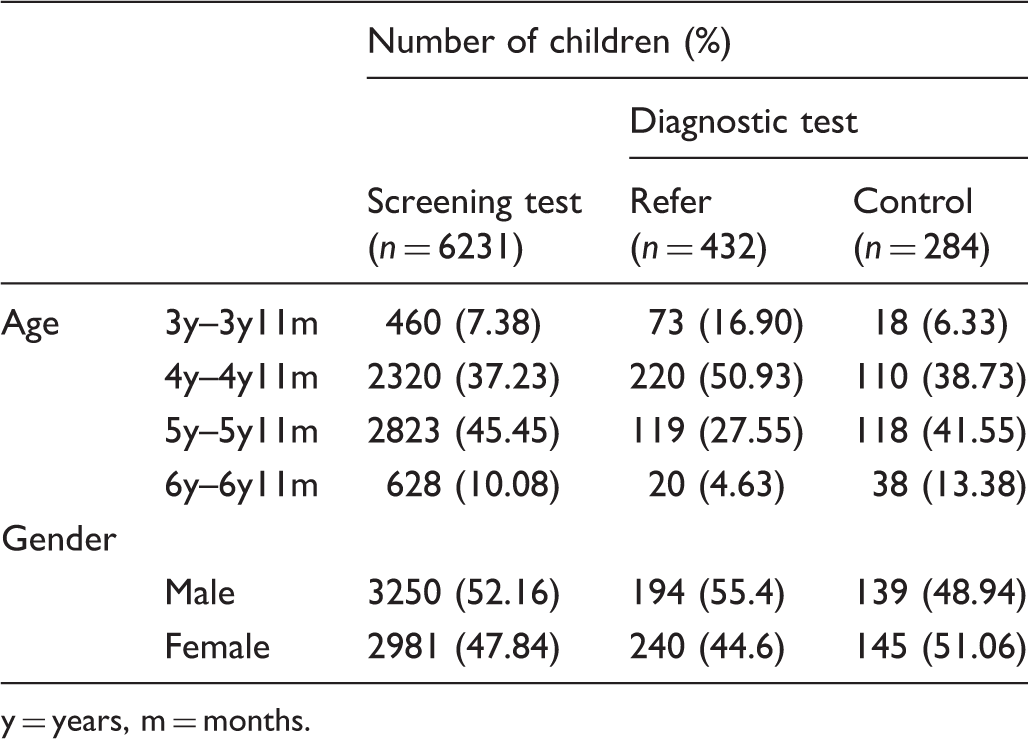
Demographic data of subjects who attended the screening and diagnostic test.
y = years, m = months.
Referral rate
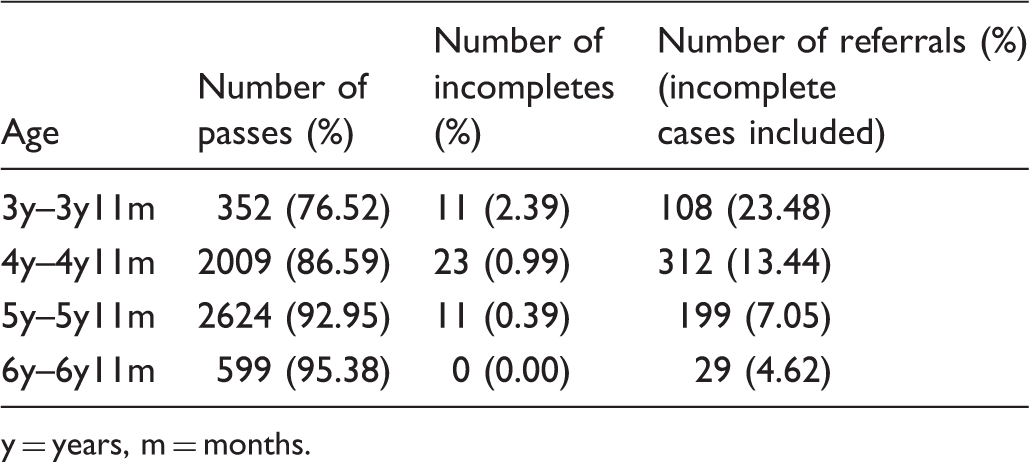
Screening results for different age groups.
y = years, m = months.
Diagnostic test results
Of 959 children referred for a diagnostic assessment, 647 had failed the automated hearing rescreening test (refer group) and 312 had passed the initial screening test (control group); 432 children from the refer group and 284 children from the control group underwent the diagnostic test. The age and gender distributions of the children are listed in Table 1. The follow-up diagnostic assessment compliance rate was 66.8% and 91.0% for the refer and control groups, respectively. Hearing loss was confirmed in 131 children from the refer group and in 31 children from the control group. Among these 162 children, 15 (9.26%) had sensorineural loss and 147 (90.47%) had conductive hearing loss.
Sensitivity and specificity of the automated screening test
Sensitivity and specificity of the automated hearing screening test in different age groups.
y = years, m = months.
Risk factors for hearing loss
The results of the univariate analysis of the studied factors.
p < 0.01; *p < 0.05.
Discussion
In this study, an automated hearing screening system for preschool children was evaluated.
A previous study evaluating the system in school children (6 – 10 years old) 11 found the sensitivity and specificity of the system to be 0.63 and 0.82, respectively. There are several possible reasons for the improvement in sensitivity and specificity in the present study. In the previous study, screening was only performed once, and all of the children who failed the test the first time were placed in the refer group. It was found that some of these children failed the test because they were unfamiliar with the test system and needed more practice. Thus in the present study, an immediate rescreen for those who failed the first attempt was mandatory, and only those who failed the rescreen were placed in the refer group. This procedure may help to decrease the number of false positive cases in the testing. However, the test may become boring if too much practice is performed. Although the attention problem was not observed in this study, children’s attention may be maintained by adding a wider variety of reinforcers in the future version of the automated hearing screening system.
Another possible reason for the higher sensitivity and specificity in the present study was the better control of ambient noise level in the test environment. The ambient noise level ranged from 45 to 65 dBA in the previous study, whereas the range of ambient noise level measured in the present test environment was 40 to 51 dBA. As shown in the previous study, even when noise-cancelling headphones were used with the automated test system, the test results were still significantly affected by ambient noise levels. Thus, it is not surprising that a lower ambient noise level would result in fewer false positives.
Most of the children were able to complete the automated tests by themselves in this study. The incompletion rate dropped from 2.39% in the 3 years–3 years 11 months age group to 0% in the 6 years–6 years 11 months age group. The use of conventional pure-tone screening in the preschool populations has been questioned, as some research has found that the incompletion rate of the test could reach 45% in the 3-year-old age group and 7% in the 4-year-old age group. 13 The incompletion rates for the automated system were much lower than those reported for the conventional pure-tone screening. There was a significant age effect on the failure rates, suggesting that the automated screening system is more suitable for children aged 5 or older. The sensitivity and specificity of the automated screening test were low in the 3 year–3 years 11 months and 4 year–4 years 11 months group, but high in the two older groups. This further suggests that the automated hearing screening test was a reliable and valid test for children as young as 5 years old.
Noncompliance for follow-up care has been considered as the greatest challenge that affects the success of any mass-screening programme. 14 The follow-up diagnostic assessment compliance rate was only 66.8% for the refer group. This is relatively low, especially when compared with the compliance rate of 91.0% for the control group. The follow-up diagnostic assessment was provided free of charge for both subject groups. It is interesting that parents of the control group were more willing to bring their children to obtain the diagnostic assessment than the refer group. It is possible that some parents do not think their child has a significant hearing problem, or some parents may fear the possibility of their child needing amplification and the long-standing stigma of hearing aid use. 14 If these are the reasons, public education should be strengthened to enhance awareness of the importance of early identification of and intervention in hearing loss.
Universal newborn hearing screening has been implemented in Shanghai since 2002. Subjects with congenital hearing loss may have been identified well before this study. It is possible that parents of children with known sensorineural hearing loss did not think they need the diagnostic assessment. It may also explain why so few cases of sensorineural hearing loss, but a relatively high proportion of conductive hearing loss was identified in this study. All of the conductive hearing loss cases identified were caused by otitis media with effusion (OME). The prevalence of OME was 2.36% (147/6231) in this study but the figure may have been underestimated as our screening system does not test the 500 Hz which is an important frequency for assessing the auditory impact of middle ear disease. 15
Risk factors for hearing loss were also investigated in this study. The newborn hearing screening test results were the most significant risk factor for hearing loss, followed by parental suspicion of hearing loss. Interestingly, none of the parents of those children who failed the newborn hearing screening test suspected that their children had hearing loss. The follow-up service that these children had received after the newborn screening was unknown. Long-term monitoring, and at the very least parental observation, may be warranted for children who failed newborn hearing screening.
The automated screening test results are now stored as online data (cloud storage). Cloud data management enables systematic and accurate follow-up even for large-scale screening programmes. Cloud storage has been proven to be a reliable and stable method for handling this study’s thousands of participants. Compared with the conventional pure tone screening test, the automated test is more engaging and is better able to maintain children’s attention. A facilitator with minimal training, rather than an audiologist, can monitor the automated test. The automatic screening system is thus more feasible for use in places where professional support is scarce.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Ethical considerations
Research ethics approval was granted by the Medical Ethics Committee of the Xinhua Hospital, Shanghai Jiaotong University for the study (No. XHEC-C-2012-006).
Funding
This project was supported by grants from the Health Ministry Special Fund, China (grant number 201202005) and the 12th Five-Year National Key Technologies R&D Program (2012BAI12B01).