
Abstract
Although advanced diagnostic and treatment methods are available, congenital heart disease (CHD) holds an important place among the causes of death within the first year of age. Therefore, several prognostic factors are needed for diagnosis and monitoring of these patients. In this study, which includes 66 CHD patients and 38 healthy control children, serum cardiac troponin-I (cTnI), high-sensitivity C-reactive protein (Hs-CRP), and N-terminal prohormone brain-type natriuretic peptide (NT-proBNP) levels were analyzed for their prognostics values. The patient groups were categorized and then evaluated as cyanotic (n = 16), acyanotic (n = 50), symptomatic (n = 23), asymptomatic (n = 43), and isolated ventricular septal defect (VSD)-isolated atrial septal defect (ASD) groups. Cyanotic group was statistically compared with acyanotic group, symptomatic group with asymptomatic group, and VSD group with ASD group. Between the cyanotic, acyanotic, and control groups; between symptomatic and asymptomatic groups; and between the VSD and ASD groups, significant difference was not showed for age (p > 0.05). NT-proBNP was found to be significantly higher in the cyanotic group than acyanotic and control group, in the symptomatic group than asymptomatic group; and in the patient group than healthy control group (p < 0.05). Between the groups of VSD and ASD, significant difference was not showed (p > 0.05). The same comparison results for TnI and Hs-CRP were not significant (p > 0.05). TnI and Hs-CRP were only found significantly higher in the patient group than healthy control group (p < 0.05). Eventually, we think that NT-proBNP, Hs-CRP, and TnI might be used for clinical management and estimation of outcome of these disorders in the future and these also might be able to modify existing strategies, but much more studies are needed.
Introduction
Despite advanced diagnosis and treatment methods, congenital heart diseases (CHDs) are a group of diseases that are still an important reason for death within the first year after birth. 1 Therefore, various prognostic factors were needed for the diagnosis and follow-up of these patients. In recent years, number of research studies based on prognostic measurement of natriuretic peptides, cardiac troponins (cTns), and high-sensitivity C-reactive protein (Hs-CRP) levels in various pathologies of cardiovascular systems have been progressively increasing. However, the number of studies evaluating these parameters in children with CHDs is very low.
Natriuretic peptides are a class belonging to hormones that regulate blood pressure, electrolyte balance, and liquid volume. Brain-type natriuretic peptide (BNP) is a cardiac neurohormone.. They are secreted by ventricular myocytes as a cell response to the decline in volume or pressure increase. 2 –7 While measurement of plasma BNP levels have taken its place as an extremely useful biochemical marker in the diagnosis, treatment, and follow-up adult patients with congestive heart failure, limited knowledge on how the levels change due to CHDs limits the clinical use of this parameter. 3 Detecting plasma BNP levels in children with CHDs will provide data on BNP’s use in cardiovascular pathologies other than heart failure.
Even though CRP, in the past, was the only useful parameter in the diagnosis of tissue damage and inflammation, in recent years, it has been used in the diagnosis of cardiovascular diseases. In the studies conducted in adults, presence of a direct relation between atherosclerotic cardiovascular diseases, diabetes, chronic heart failure, and serum Hs-CRP concentrations have been shown. In some studies increased Hs-CRP has been shown in obese children and adolescents, and patients with a history of Kawasaki disease but very few information is available on its importance in CHDs. 8
Troponins are structural proteins regulating the relation between actin and myosin in skeletal muscle and cardiac myocytes. Its subgroups are troponin I (TnI), TnT, and TnC. Among these, TnI, under normal circumstances, cannot be detected or can only be detected at a very low level in serum; however, in conditions causing myocardial damage such as acute myocardial infarction, acute myocarditis, and obtuse cardiac trauma, it is very specific in showing cardiac damage. 9 In literature, there are a limited number of studies on serum TnT levels in CHD; however, we could find none on serum TnI.
A total of 66 congenital heart patients aged between 3 months and 16 years were diagnosed and followed by the Department of Pediatric Health and Diseases, Faculty of Medicine, Pediatric Cardiology Polyclinic, Yuzuncu Yil University (Hundredth Year University), Turkey, and 38 healthy children with no chronic diseases were enrolled in the current study. The objective of this study was to measure the patients’ cTnI, Hs-CRP, and N-terminal prohormone BNP (NT-proBNP) levels and to see whether a correlation among these existed.
Material and methods
This study was conducted on 66 congenital heart patients, aged between 3 months and 16 years, who were diagnosed and followed by the Department of Pediatric Health and Diseases, Faculty of Medicine, Pediatric Cardiology Polyclinic, Yuzuncu Yil University (Hundredth Year University), Turkey. Patients diagnosed with echocardiogram were separated as cyanotic (n = 16) and acyanotic (n = 50). Patients with complaints and clinical findings such as respiratory problems, cyanosis, pulmonary hypertension, cardiomegaly, and heart failure were categorized as symptomatic and patients with no complaints or clinical findings were placed in to asymptomatic group. Only three symptomatic and two asymptomatic patients were receiving digoxin treatment. Patients with isolated atrial septal defect (ASD) or isolated ventricular septal defect (VSD) were placed into two separate groups for evaluation. Thirty-eight children with similar ages to the patients group, presenting at the polyclinic without a chronic disease and with no abnormalities in their physical examinations and laboratory tests (liver and renal functions, full blood count, and electrolytes) were placed into the control group. Patients with infectious symptoms, obese patients, patients with serum cholesterol levels >220 mg/dl, diabetic patients or with elevated liver enzymes were excluded from the study.
Approximately 1 cc of venous blood, from both the patient and the control group, was drawn into a hemogram tube with potassium ethylenediaminetetraacetic acid for NT-proBNP and cTnI, and for Hs-CRP, approximately 1 cc of venous blood was drawn into a biochemistry tube and immediately sent to the laboratory. The blood samples were separated into serums by centrifuging at 4000 r/min for 5 min. Serums obtained were stored at −20°C until analysis. Care was given in choosing samples without hemolysis and that were not lipemic. When targeted number of samples were obtained, all samples were allowed to come to room temperature (15–18°C) while carefully turned to mix their contents. To avoid possible divergence, all samples were analyzed the same day.
NT-proBNP and cTnI were quantitatively measured using ReLIA immunoassay Diagnostic Device (SSJ-2) and ReLIA test kits at the Department of Pathology and Laboratory Medicine, Faculty of Medicine, Yuzuncu Yil University (Hundredth Year University), Turkey. Results for NT-proBNP and cTnI were expressed in picogram per milliliter. Values below 0.001 ng/ml could not be measured quantitatively. CRP was measured nephelometrically with high sensitivity using a Dade Behring BNII device and its own kits from the Department of Pathology and Microbiology Laboratory, Yuzuncu Yil University (Hundredth Year University), Turkey. Lowest and highest CRP values measurable with this method were 0.16 and 300 mg/l, respectively.
Statistical analysis
Definitive statistics for emphasized properties were expressed in terms of average, standard deviation, and minimum and maximum values. To determine whether there were differences between the groups with respect to these variables, one-way variance analysis was performed. To determine the relationship between properties, Spearman’s correlation coefficients for each group was calculated. During the calculations, statistical significance level was chosen as 5%, and for the calculations Statistical Package for the Social Sciences (SPSS) statistics package (SPSS Inc., Chicago, Illinois, USA) was used.
Ethical
This study was conducted in accordance with the Helsinki declaration principles. After the relatives of the children enrolled into the study were informed on the objectives of the study, their consent was obtained and included in the research. Ethical approval for the study was granted by Van Clinical Research Ethical Committee, Van, Turkey, with a decision dated 14 October 2010 and numbered 2010/04-06.
Results
A total of 66 (37 girls and 29 boys) patients comprising of 50 acyanotic (29 girls and 21 boys) and 16 cyanotic (8 girls and 8 boys) patients, and 38 (20 girls and 18 boys) healthy children as the control group were enrolled into the study. There was no statistically significant difference with respect to gender between the groups (p > 0.05). Children in terms of diagnosis are given in Table 1. The average age of the patients in acyanotic group was 2.89 ± 3.72 (0.25–14.75) years, in cyanotic group 3.34 ± 3.43 (0.25–11.00) years, and in control group 4.44 ± 2.82 (0.25–12.66) years. There were no statistically significant differences between the study groups with respect to age (p > 0.05).
The distributions of patients according to congenital heart disease.

Comparison of NT-proBNP, TnI, and Hs-CRP levels between the groups is shown in Table 2. In the cyanotic group, NT-proBNP was statistically significantly higher compared to both the acyanotic and the control groups (p < 0.05). While NT-proBNP was significantly lower in the acyanotic group compared with the cyanotic group (p < 0.05), it was significantly higher compared with the control group (p < 0.05). Furthermore, average NT-proBNP level in the patient group (cyanotic + acyanotic) was found to be 914.34 ± 1795.24 and 45.29 ± 46.10 pg/ml in the control group. Compared with the control group, NT-proBNP level was statistically significantly higher in the patient group (p < 0.05). TnI was statistically significantly higher in both cyanotic and acyanotic groups compared with the control group (p < 0.05). Average TnI level was found to be 0.071 ± 0.134 pg/ml in the patient group (cyanotic + acyanotic) and 0.009 ± 0.045 pg/ml in the control group. TnI was found to be statistically significantly higher in the patient group than the control group (p < 0.05). While Hs-CRP levels were found to be higher in acyanotic group compared with the cyanotic group, the difference was not statistically significant (p > 0.05). Hs-CRP was statistically significantly higher in both cyanotic and acyanotic group compared with the control group (p < 0.05). However, average Hs-CRP in the patient group (cyanotic + acyanotic) was found to be 1.350 ± 2.087 and 0.323 ± 0.431 in the control group. Compared with the control group, Hs-CRP levels were statistically significantly higher in the patient group (p < 0.05).
Comparison of acyanotic, cyanotic, and control groups according to NT-proBNP, troponin I, Hs-CRP levels.
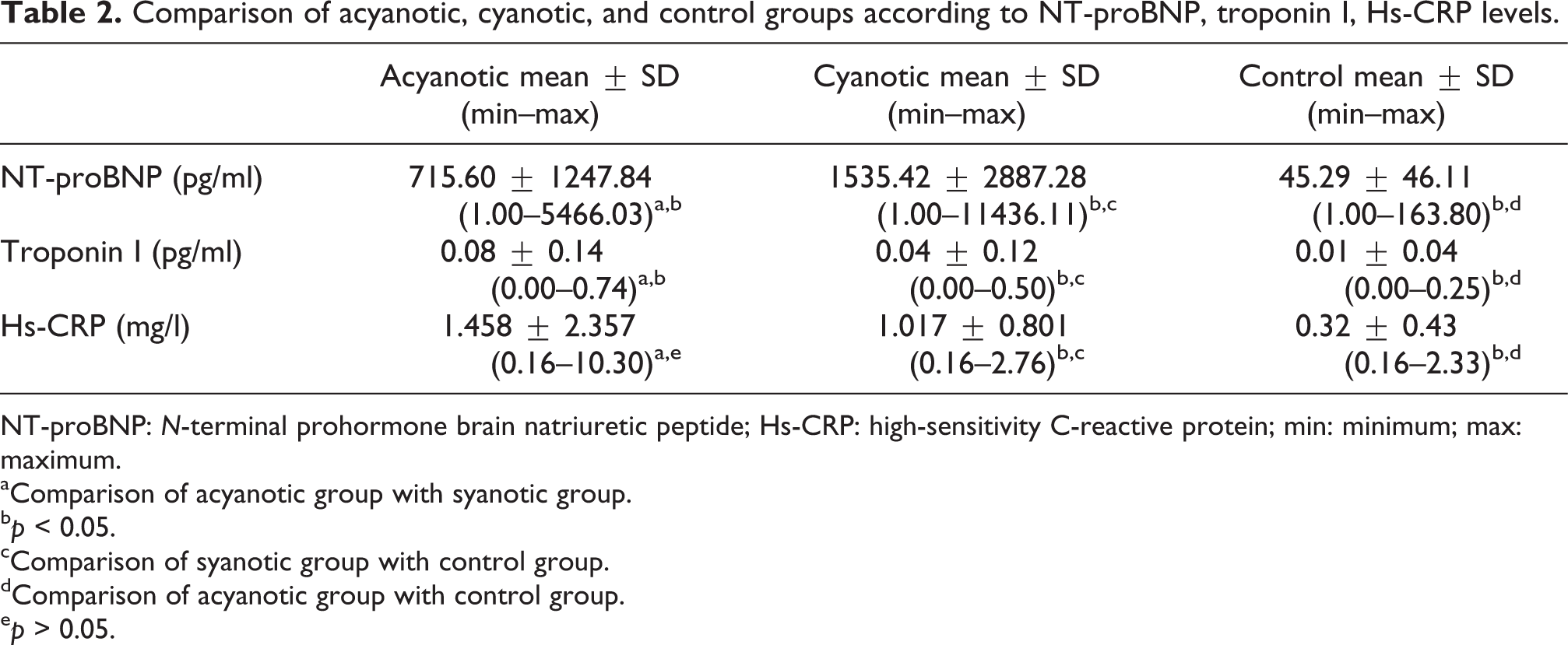
NT-proBNP: N-terminal prohormone brain natriuretic peptide; Hs-CRP: high-sensitivity C-reactive protein; min: minimum; max: maximum.
aComparison of acyanotic group with syanotic group.
b p < 0.05.
cComparison of syanotic group with control group.
dComparison of acyanotic group with control group.
e p > 0.05.
The relation between age, NT-proBNP, TnI, and Hs-CRP was investigated using Spearman’s correlation coefficients. There was a negative correlation between age and NT-proBNP (r = −0.568, p < 0.01) and age and Hs-CRP (r = −0.317, p < 0.05). There were no statistically significant correlations between other parameters. In cyanotic group, however, a negative correlation between age and NT-proBNP (r = −0.652, p < 0.01) and age and Hs-CRP (r = −0.586, p < 0.05) and a positive correlation between NT-proBNP and Hs-CRP (r = 0.623, p < 0.01) was found. When a similar comparison was performed in the control group, positive correlation was found between age and NT-proBNP (r = 0.445, p < 0.01) and NT- proBNP and Hs-CRP (r = 0.333, p < 0.05).
In all, 13 (26%) of the 50 patients in acyonatic group and 10 (74%) of the 16 patients in cyanotic group were symptomatic at the time of presenting to the clinic. Number of symptomatic patients at presentation was statistically significantly higher in cyanotic group compared with the acyanotic group (p < 0.05). There was no statistically significant difference in the groups with respect to the ages of asymptomatic and symptomatic patients (p > 0.05). When NT-proBNP levels of asymptomatic, symptomatic, and control groups were compared, a meaningful difference was found among the three groups (p < 0.05; Table 3). TnI levels were found to be significantly higher in asymptomatic and symptomatic groups compared with the control group (p < 0.05). No statistically significant difference was found between asymptomatic and symptomatic groups (p > 0.05). When Hs-CRP levels of asymptomatic, symptomatic, and control groups were compared (Table 3), there was a meaningful difference in asymptomatic and symptomatic groups compared with the control group (p < 0.05). There was no significant difference between asymptomatic group and symptomatic group (p > 0.05).
Comparison of asymptomatic, symptomatic, and control groups according to NT-proBNP, troponin I, and Hs-CRP levels.

NT-proBNP: N-terminal pro-hormone brain natriuretic peptide; Hs-CRP: high-sensitivity C-reactive protein; min: minimum; max: maximum.
aComparison of acyanotic group with cyanotic group.
b p < 0.05.
cComparison of cyanotic group with control group.
dComparison of acyanotic group with control group.
e p > 0.05.
When groups were compared for the positivity ratio of TnI, in 26 of the 50 patients (52%) with acyanotic CHD, in 6 of the 16 patients (37.5%) with cyanotic CHD, and in 2 of the 38 control group patients (5.2%), TnI was found to be positive (> 0.001 pg/ml). According to this TnI positivity ratio, acyanotic and cyanotic groups were statistically significantly higher than the control group (p < 0.05). However, TnI positivity ratio in acyanotic CHD group was higher than cyanotic CHD group, but it was not statistically meaningful (p > 0.05; Table 4). TnI was positive in 34 of the 66 patients in the patient (cyanotic + acyanotic) group, and 2 of the 38 patients in control group (> 0.001 pg/ml). According to this, in comparison with the control group, positivity ratio of TnI in the patient group was statistically significant (p < 0.05; Table 4).
Comparison of the rate of troponin I positivity in groups.

a p > 0.05: comparison of acyanotic group with cyanotic group.
b p < 0.05: comparison of syanotic group with control group.
c p < 0.05: comparison of patient group with control group.
d p < 0.05: comparison of acyanotic group with control group.
When the data of patients with ASD and VSD, which are the most frequently seen CHDs, were evaluated, the average age of patients with ASD was 3.47 ± 3.72; and patients with VSD was 2.53 ± 3.23. There was no statistical difference with respect to age between ASD and VSD groups. Age values of ASD and VSD are shown in Table 5. When ASD and VSD groups were compared with respect to NT-proBNP, TnI, and Hs-CRP levels, no statistically significant differences were found (Table 6).
The comparison of ASD and VSD groups with regard to age.

ASD: atrial septal defect; VSD: ventricular septal defect; min: minimum; max: maximum.
The comparison of ASD and VSD groups with regard to NT-proBNP, troponin I, and Hs-CRP.a

ASD: atrial septal defect; VSD: ventricular septal defect; NT-proBNP: N-terminal prohormone brain natriuretic peptide; Hs-CRP: high-sensitivity C-reactive protein.
Discussion
CHDs cover structural or functional anomalies developed in the cardiovascular system prior to birth. 10 Its frequency is known as 6–8 in every 1000 live births. 11 When distribution of CHDs is investigated within itself, VSD is the most common with a ratio of 25–30%. With a ratio of 5–7%, Fallot tetralogy is known as the most frequently observed cyanotic CHD after 1 year of age. Large artery transposition is the most frequent cyanotic lesion during the newborn period. 12 –14 When 10 patients with Fallot tetralogy and 3 with endocardial cushion defects were excluded from the 66 patients with CHDs, in 27 patients (40%) along with isolated or other congenital heart anomalies, VSD was most frequently observed. Fallot tetralogy was present in 10 (62.5%) of the 16 cyanotic group patients, and it was the most frequently seen disease. These findings are in concert with the literature.
Natriuretic peptides regulate blood pressure, electrolyte balance, and liquid volume. B-type natriuretic peptides are members of this family. Fundamentally, they are synthesized by cardiac myositis against increased wall stress, and after being secreted as prohormones, they differentiate as BNP and NT-proBNP. 15 In this study, in order to see its prognostic importance in children with CHD diagnosis, NT-proBNP levels, which, when compared to other methods, are inexpensive, faster, and does not require skilled workers, were evaluated. Since in a study, where plasma BNP levels were evaluated in children and newborns with CHDs, the BNP levels were shown to be higher during newborn period compared to other childhood stages, we did not include children younger than 3 months into our study. 16 In a large study by Cowley et al. on 96 children with CHD, plasma BNP levels of patients administered with cardiac catheterization for diagnosis and treatment purposes were measured, and at the end of the study, the researchers have noted that for patients receiving treatment attempts for CHD, repeated BNP measurements could be important in the treatment and follow-up of children. In the same study, 3 and in a study conducted by Nagaya et al., 17 asymptomatic patients with isolated ASD was shown to have normal BNP levels. In a study conducted by Özhan et al. on 35 patients, the relation between shunt amount and BNP was investigated in 9 patients with VSD and 26 patients with ASD. To determine shunt amount, pulmonary blood flow (Q p)/systematic blood flow (Q s) ratios were calculated. Results show that as the amount of shunt increases (Q p/Q s over 1.5), BNP levels also increases. 18 In a study conducted on 55 premature babies by Holmstrom et al. in patients with a high shunt amount and patent ductus arteriosus (PDA) diagnosis, increased BNP and NT-proatrial natriuretic peptide (ANP) levels were reported. 19 In another study conducted by Kazancı et al., BNP levels were found to be low in the control group with no left–right shunt, and in patients with left–right shunts and PDA diagnosis, BNP levels were found to be high. 20 Mueller et al. 21 have shown that in early diagnosis of heart failure in adult patients with symptomatic and asymptomatic heart diseases, NT-proBNP levels are more specific than BNP. Hammerer-Lercher et al. 22 reported in detecting children with asymptomatic heart diseases with no heart failure findings NT-proBNP is a useful predictor. The study by Kevin O. Maher et al. has shown that it can be a predictor that can be helpful to emergency department personnel as a diagnosis marker in the evaluation of critical newborn patients with congenital or acquired heart diseases. 23 In this study conducted on 38 healthy controls and 50 acyanotic and 16 cyanotic children with CHD, we found the serum NT-proBNP levels in the healthy control group significantly higher compared to both cyanotic and acyanotic groups. In the study, 23 of the 66 patients were symptomatic, and in this group NT-proBNP was significantly higher compared to both asymptomatic and the control groups. Therefore, our results support the idea that NT-proBNP can be a predictor that can be used in detecting children symptomatic or asymptomatic structural cardiac problems.
Experiments and clinical studies investigating the relationship of hypoxia and BNP show that short-term ischemia and hypoxia episodes rapidly increase the BNP secretion for cardiac tissue. 24,25 The study by Hopkins et al. on adult patients with cyanotic CHD has shown that hypoxia is a direct stimulant for BNP secretion from cardiac myocytes. In this study following the measurement with a method based on calculation of total body liquid volume, in spite of reduced body liquid in adults with cyanotic CHDs, compared with acyonatic patients detected that BNP levels were markedly elevated. 26 In our study, we detected meaningful elevated plasma NT-proBNP levels in the cyanotic congenital disease group compared to both healthy controls and acyonatic patient group (p < 0.05). As the study was conducted in heterogeneous patient group with respect to clinical diagnosis, this result, while confirming that chronic hypoxia has a stimulating effect on BNP, will be beneficial to repeat this in a wider patient series where other factors that can affect BNP secretion are eliminated. In a study conducted by Hatice A. Demirol, 27 serum NT-proBNP levels were measured in 20 patients with VSD diagnosis and 20 patients with ASD diagnosis aged between 15 days and 16 years. Serum NT-proBNP levels of 20 patients with no chronic diseases were measured as the control group. As a result of this study, serum NT-proBNP levels of VSD group and ASD group were compared and statistically significant difference was not found. However, when the serum NT-proBNP levels of VSD and ASD group were compared with the control group, a statistically significant difference was found. As a result in children with CHD, NT-proBNP levels were found to be higher compared with the control group. Of the total patients included in the study, 10 were diagnosed with isolated ASD and 19 with isolated VSD. When serum NT-proBNP levels of VSD group and ASD group were statistically compared, there were no significant differences (p > 0.05). At the same time there were statistical differences in TnI and Hs-CRP levels between the groups (p > 0.05).
While in the past, CRP was only a parameter useful in diagnosing tissue damage and inflammation; in recent years, it has also been in used in diagnosing cardiovascular diseases. In studies on adults, presence of a direct association between atherosclerotic cardiovascular diseases, diabetes, chronic heart failure, and serum Hs-CRP concentrations have been shown. In some studies, Hs-CRP elevation have been shown in obese children and adolescents and patients with a history of Kawasaki disease; however, in literature, we have only come across a study by Hideshi Tomita et al. on its clinical importance in CHDs. In the study by Hideshi Tomita et al., 8 conducted on 70 children with CHD, the Hs-CRP and BNP levels in relation to hypoxia was found to be significantly higher than control group and also a positive correlation between Hs-CRP and BNP in relation to hypoxia was found. 8 In our study, Hs-CRP levels in cyanotic and acyanotic groups were found to statistically significantly higher than those in the control group. Additionally, it was also found to be statistically significantly higher in symptomatic and asymptomatic groups than the control group. There was no statistically significant difference between cyanotic and acyanotic groups or symptomatic and asymptomatic groups. In the cyanotic group, a positive correlation was found between Hs-CRP and NT-proBNP levels (r = 0.623, p < 0.01), but the positive correlation in the acyanotic group was not statistically meaningful (r = 0.224, p > 0.05). While Hs-CRP level in relation with hypoxia was expected to be higher; in our study, a meaningful difference compared with the acyanotic group was not found. However, there was meaningful difference in those with disease compared with the control group.
Tns are structural proteins regulating the relation between actin and myosin in skeletal muscle and cardiac myocytes. Its subgroups are TnI, TnT, and TnC. TnI inhibits actin–myosin interaction by binding to actin. TnT binds to tropomyosine and TnC binds to calcium in the Tn complex. Because TnT and TnI are coded by different genes in skeletal muscle and heart muscle, they have different amino acid sequences. Therefore, cTnT and cTnI can be measured rapidly and accurately both quantitatively and qualitatively. On the other hand, since TnC is exactly the same as its isoform in smooth muscle, it does not have a cardiac specificity. Among these, TnI, under normal circumstances, either cannot be detected in serum or detected in very low levels without myocardial damage; however, in conditions causing myocardial damage such as acute myocardial infarction, acute myocarditis, obtuse cardiac trauma, it is very specific in showing cardiac damage. 28 In literature, while there are studies on serum TnT levels in CHD, we could find none on serum TnI. In the study by Ryoji Taniguchi et al., which was conducted in a series of 190 patients with chronic heart failure, serum TnT and BNP concentrations were measured simultaneously. In this study, the 190 patients comprised of 41 with dilated cardiomyopathy, 53 with valvular or KKH, 16 with hypertensive heart disease, 40 with ischemic heart disease, 22 with hypertensive cardiomyopathy, and 18 with other diseases. In a study of 11 patients with valvular or congenital heart disease, serum TnT concentrations were calculated over 0.01 ng/ml. 29 In our study, we measured TnI levels. In our study, ccTn concentration ratios at >0.001 pg/ml were found to be 6/16 (37.5%) in cyanotic patient group, 26/50 (52%) acyonatic patient group, and 2/38 (2.4%) in control group. According to these results, ccTnI levels in patients with KKH were significantly higher when compared with the control group. This result can be interpreted as TnI secretion into blood as a result of myocardial cell damage associated with hypoxia caused by the defect in KKH. Compared to acyanotic patients, the heart muscle of cyanotic patients is exposed to more hypoxia, higher TnI levels were expected in cyanotic patients compared to acyonatic patients. However, in our study, there was no meaningful difference between cyanotic and acyanotic patients. Also, in our study, while there was no difference between symptomatic and asymptomatic groups, compared with the control groups, there were meaningful differences in both groups.
Additionally, in a study performed by Eindhoven et al., the authors evaluated the clinical utility of BNP in patients with CHD. They executed a PubMed literature search and included 49 articles that focused on complex congenital heart defects such as tetralogy of Fallot, systemic right ventricle, and univentricular hearts, and they extracted data on BNP measurements and cardiac function parameters. Finally, they concluded that this review showed an overall increase in BNP values in complex CHD, although differences between types of congenital heart anomaly were present. As BNP values differed widely, conclusions for individual patients should be drawn with caution. These results were also appropriate with our findings. 30
As a result, the fact that TnI concentrations were significantly higher in the patient groups compared with control groups suggests that in the future it could be an important cardiac predictor in the diagnosis and follow-up of children with CHD, if it is supported with new studies; and significantly higher NT-proBNP levels in patient group compared with controls as well as in cyanotic group compared with acyanotic group suggests that these levels can be a noninvasive, fast serological predictor in the diagnosis and prognosis of children with CHD, and also we believe that Hs-CRP levels can be used in diagnosing these children.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.