
Abstract
High plasma level of P-selectin is associated with the development of venous thromboembolism (VTE). Furthermore, supplementation of vitamin D could decrease thrombotic events. Hence, this study was designed to examine whether the administration of vitamin D can influence the plasma level of P-selectin in patients with VTE. In the randomized controlled trial, 60 patients with confirmed acute deep vein thrombosis and/or pulmonary embolism (PE) were randomized into the intervention (n = 20) and control (n = 40) groups. The intervention arm was given an intramuscular single dose of 300 000 IU vitamin D3. Plasma level of 25-hydroxy vitamin D, P-selectin, and high-sensitive C-reactive protein (hs-CRP) was measured at baseline and 4 weeks after. The plasma level of P-selectin (95% confidence interval = −5.99 to −1.63, P = .022) and hs-CRP (P = .024) significantly declined in vitamin D-treated group, while only hs-CRP was significantly decreased in the control group (P = .011). However, the magnitude of these reductions was not statistically significant. This study could not support the potential benefit of the high-dose vitamin D on plasma level of P-selectin and hs-CRP in patients with VTE.
Introduction
Vitamin D deficiency is a common worldwide problem with a frequency about 30% to 50%. 1 Recent data have indicated that the low level of vitamin D is associated with increased risk of cardiovascular diseases (CVDs) and mortality. 2
It has been shown that the low level of vitamin D is linked to the development of venous thromboembolism (VTE). 3,4 As well, administration of vitamin D has reduced the thrombotic events in patients with cancer. 5 Antithrombotic activity of vitamin D is mainly due to inhibition of tissue factor (TF) and upregulation of interleukin 10 (IL-10). 6 –8
P-selectin, a cell adhesion protein, is located in the α granules of platelets and Weibel-Palade bodies of endothelial cells. 9,10 After platelet activation, soluble form of P-selectin (sP-selectin) distributes in circulation and binds to its receptor P-selectin specific ligand 1 and increases TF and IL-8 and starts the coagulation cascade. 9 –11 According to the literature, plasma level of sP-selectin is linked to the incidence of VTE. 10,12 –15 Some data have also shown the resolution of thrombosis with P-selectin inhibitors 16 –18 and suggested P-selectin as a novel target of therapeutic intervention in the treatment of VTE. 11,13
High-sensitive C-reactive protein (hs-CRP), an acute phase reactant protein, elevates in inflammatory conditions. 19,20 There are conflicting data about the relationship between hs-CRP concentration and thrombosis formation. 19 –21 However, data indicated hs-CRP levels could be implicated as a marker of treatment response in the cases of VTE. 21
Despite our knowledge about the association between vitamin D deficiency and CVD, data are still limited about the impact of vitamin D supplementation in the management of VTE. Therefore, this study was performed to evaluate the impact of vitamin D on the plasma levels of P-selectin (as a new target of therapeutic intervention) and hs-CRP (as a target of treatment response and inflammation) in patients with VTE.
Materials and Methods
Study Design and Population
To examine the study hypothesis, a prospective, randomized, controlled trial was performed in Tehran Heart Center on patients with acute VTE from the summer of 2012 to January 2013.
All consented patients aged 18 years and older with confirmed acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE) were entered. The exclusion criteria included coexistence of autoimmune and inflammatory diseases, pregnancy, malignancy, existence of any infectious, hepatic, and renal diseases, sarcoidosis, history of vitamin D supplementation, use of immunosuppressant, and immunomodulator medications.
The sample size was determined to be at least 19 patients in each group regarding a statistical power of 80% (1-β = 0.8) and an α error of 5% (α = .05). As this study is the first one in patients with VTE as well as the lack of similar studies, we used mean ± standard deviation (SD) values of P-selectin in the study of Assimon et al 22 that investigated the potential vascular benefit of vitamin D on hemodialysis patients. To improve the study power, the sample size in the control group was determined to be 2-fold more than the intervention group (40:20).
All patients were randomized (using the computer generated random number list) into the groups of intervention (n = 20) and control (n = 40). The intervention group received a single dose of 300 000 international units (IUs) of vitamin D3 intramuscularly immediately after confirmation and followed up for a 4-week period. All patients received standard treatment of VTE. A data collecting form was designed by the investigators in order to record patients’ information, including patients’ demographic data, such as sex, age, weight, height, body mass index, past medical history, drug history, laboratory data, and positive family history for CVD.
Ethics
The study was approved by the ethics committee of the university and then registered in the International Clinical Trials Registry Platform, World Health Organization (ID: IRCT201112068307N1) as well as conducted according to the Declaration of Helsinki.
Blood Sampling
Blood samples were obtained following diagnosis of acute DVT or PE before starting any medications and subsequently after 4 weeks. All samples were drawn into 3.2% sodium citrated tubes and then were spun at 1500× rpm for 10 minutes, at room temperature. The plasma was drawn off and aliquotted into 1-mL microtubes and then frozen and stored at −25°C for quantification of the 25-hydroxyvitamin D, 25(OH)D, P-selectin, and hs-CRP levels.
Measurement of Plasma 25(OH)D, Soluble P-selectin, and hs-CRP
Plasma level of 25(OH)D was determined by DiaSorin radioimmunoassay method. Enzyme-linked immunosorbent assay was carried out for quantitative detection of human plasma P-selectin level and hs-CRP. The quantities were reported in ng/mL for 25(OH)D and sP-selectin and mg/dL for hs-CRP.
The 25(OH)D levels of under 20 ng/mL were regarded as vitamin D deficiency, concentrations between
Statistical Analysis
Data analysis was carried out using SPSS version 16.0 (SPSS Inc, Chicago, Illinois, 2007). Kolmogorov-Smirnov test was performed to determine whether data had a normal distribution. Paired t test and Wilcoxon test were employed to compare the means within the groups before and after intervention. Mann-Whitney and independent sample t test were used to assess the means in different groups. Chi-square and Fisher’s exact tests were also applied for frequency analysis. The continuous data were presented as mean ± SD. P values less than .05 were regarded as significant.
Results
Baseline Patient Characteristics
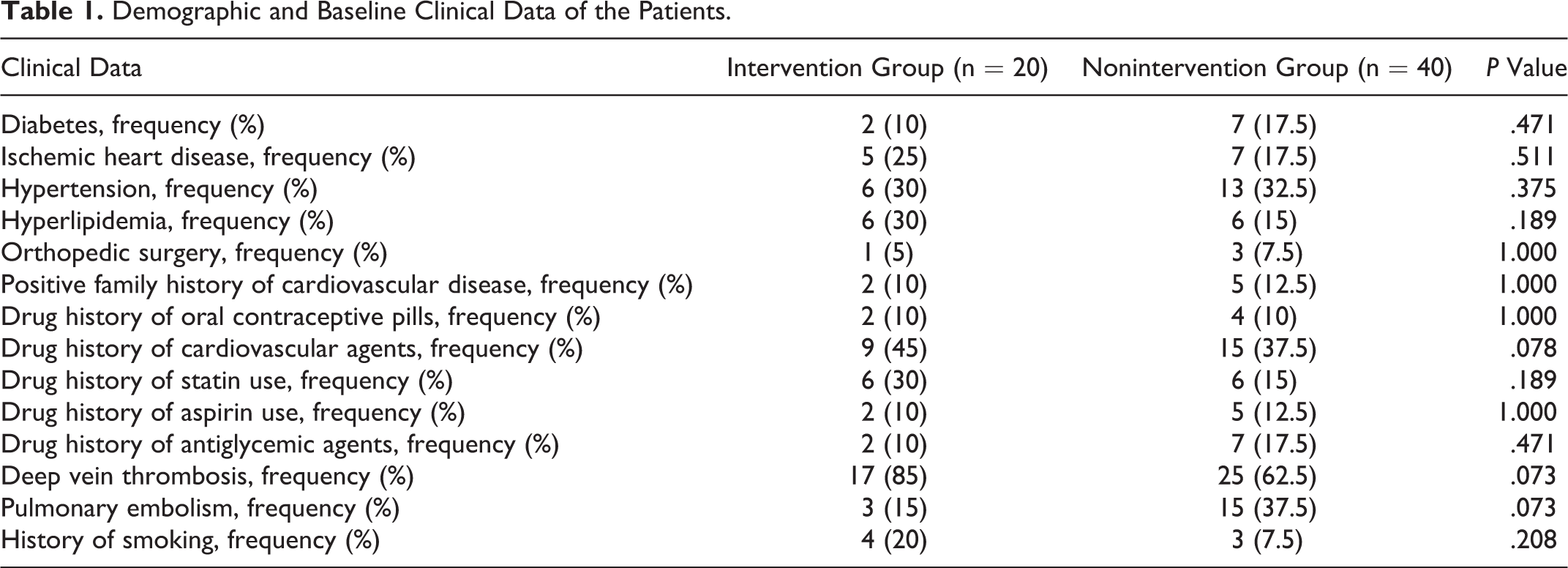
Among 70 potential participants who were screened for eligibility, a total of 60 patients including 36 (60%) males and 24 (40%) females with the diagnosis of acute DVT (n = 42) and PE (n = 18) were enrolled (Figure 1). The mean age of the patients was 53.2 ± 17.3 (mean ± SD) years. The baseline 25(OH)D level of participants was 19.2 ± 12.3 ng/mL. Vitamin D deficiency and insufficiency were detected in 65% (n = 39) and 20% (n = 12) of patients, respectively, as well as 15% (n = 9) had normal levels of vitamin D. The mean baseline plasma level of P-selectin and hs-CRP was 163 ± 57.3 ng/mL and 29.7 ± 38 mg/dL, respectively. Demographics and clinical data in 2 groups were not statistically different (Table 1). Anticoagulation-related data were also the same regarding the statistic tests as shown in Table 2.
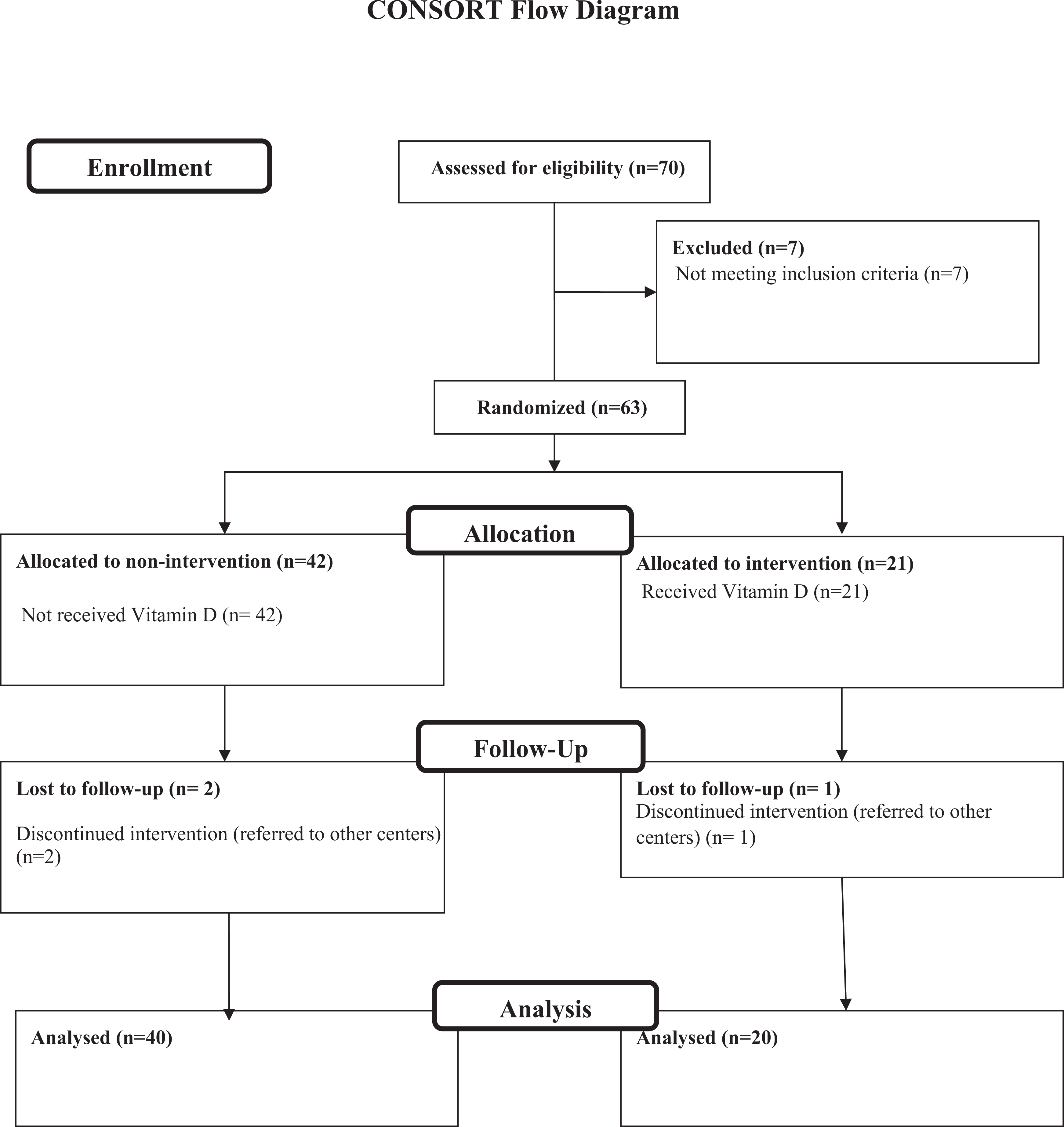
Flow diagram of the study.
Demographic and Baseline Clinical Data of the Patients.
Anticoagulation Data and Indexes.
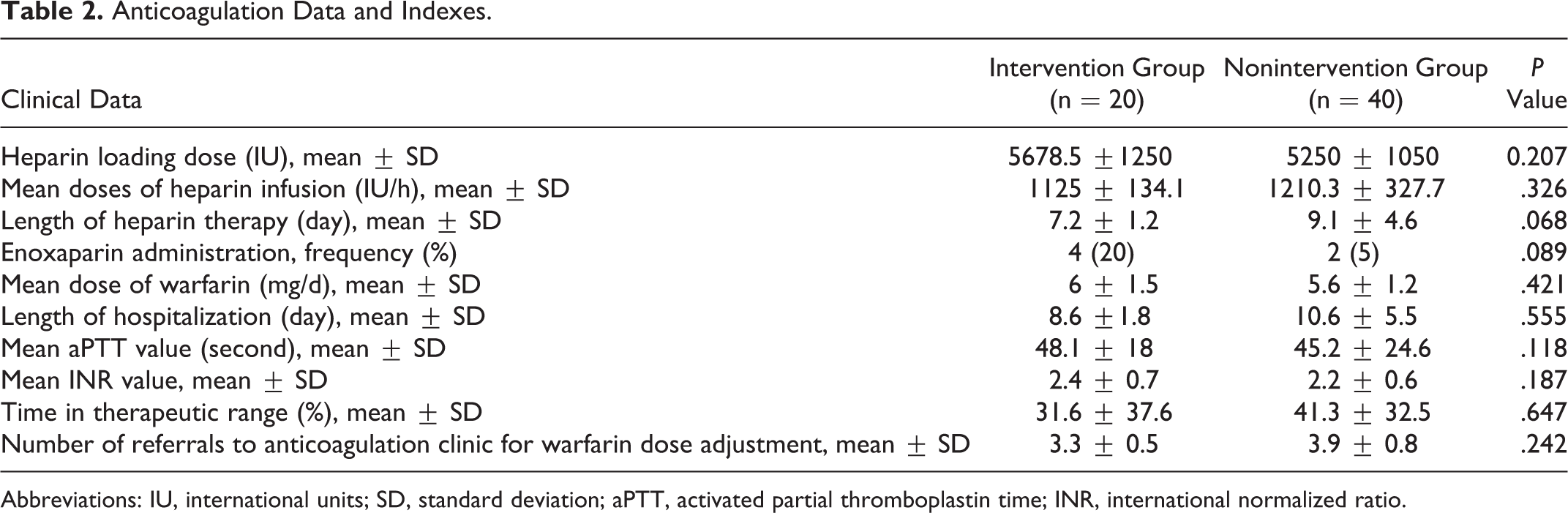
Abbreviations: IU, international units; SD, standard deviation; aPTT, activated partial thromboplastin time; INR, international normalized ratio.
Baseline Levels of 25(OH)D, P-Selectin, and hs-CRP in Groups
The baseline level of 25(OH)D was 16.9 ± 11.6 and 20.1 ± 12.4 ng/mL in the intervention and control groups, respectively (95% confidence interval [CI] = 10.1-3.7, P = .355). As well, the baseline level of P-selectin was 167.5 ± 57 and 162.1 ± 58.1 ng/mL (95% CI = −27.1 to 37.7, P = .744), and hs-CRP level was 43.6 ± 39.7 and 25.8 ± 40.8 mg/dL in the intervention and control groups, respectively (P = .013, Wilcoxon singed rank test).
Levels of 25(OH) D, P-Selectin and hs-CRP After Intervention in 2 Groups
After administration of vitamin D, the level of 25(OH)D significantly increased in the intervention arm to 20.7 ± 14.1 ng/mL (95% CI:−5.99 to −1.63, P = .007). While in the control group the level of 25(OH)D did not significantly change (20.2 ± 12.5 ng/mL; 95% CI = −1.56 to 1.39, P = .925). No case of vitamin D toxicity was detected in both the groups.
In the intervention group, the level of P-selectin significantly decreased to 132.6 ± 36.9 ng/mL (95% CI = 10.66-59.1, P = .022), whereas this reduction in the control group was not significant (144.5 ± 56.6; 95% CI = 1.82-33.5, P = .068).
Although the amount of reduction in P-selectin (delta P-selectin) in the vitamin D-treated group was higher than the control group, it was not statistically significant when compared with the control group (34.8 ± 62.5 vs 17.7 ± 55.4; P = .296; Table 3).
The level of hs-CRP was significantly declined in both groups of intervention and control to 18.2 ± 21.1 and 10.9 ± 23.7 mg/dL, respectively. However, the amount of this reduction (delta hs-CRP) was not statistically significant when compared to the control group (P = .225; Table 3). The level of baseline 25(OH)D, P-selectin, and hs-CRP was not significantly different among males and females as well as patients with DVT or PE.
25-Hydroxy Vitamin D, P-Selectin, and hs-CRP Levels Before and After Intervention.
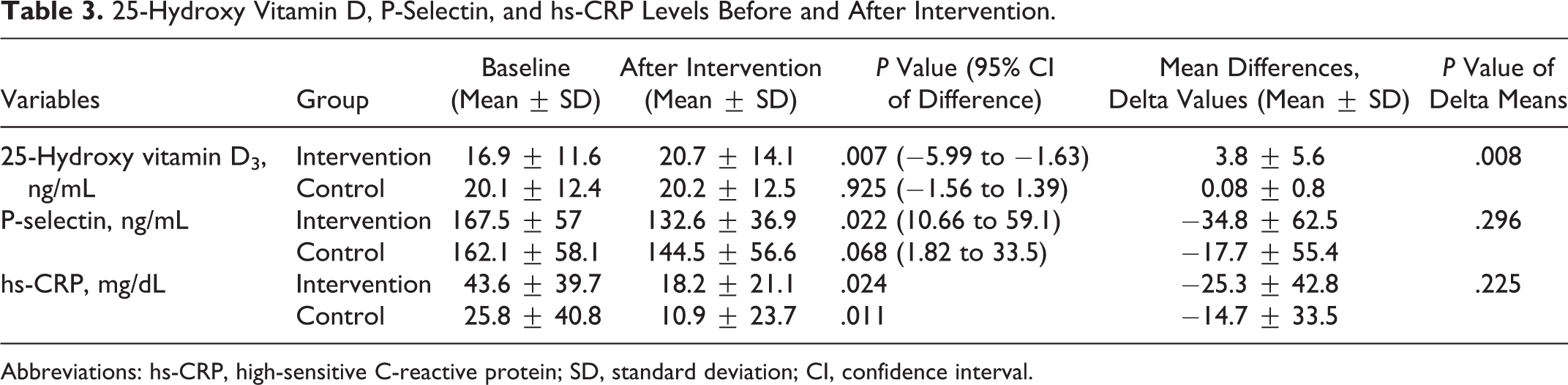
Abbreviations: hs-CRP, high-sensitive C-reactive protein; SD, standard deviation; CI, confidence interval.
Clinical Outcome
Regarding to clinical outcome in 1-month follow-up, 1 patient was hospitalized again in the intervention group. In the control group, 2 were admitted again, and 1 case of minor bleeding was detected with warfarin.
Discussion
Concerning the association between vitamin D deficiency and the development of thrombosis and this point that the thrombus resolution could be enhanced by reduction in P-selectin, this study was performed to investigate whether vitamin D supplementation could influence the plasma level of P-selectin in patients with VTE. To the best of our knowledge, this prospective, randomized controlled trial is the first investigation of vitamin D supplementation on P-selectin level in patients with VTE. In the present study, we could not show the significant reduction in P-selectin by the administration of single dose of 300 000 IU vitamin D. In our previous study, we also could not find any significant correlation between vitamin D and P-selectin and hs-CRP levels in patients with VTE. 23
In the present study, the rate of vitamin D deficiency was recognized in 65% of patients. This finding is compatible with the other studies, which described a low level of vitamin D in patients with thrombosis. 3,4
The relationship between CRP level and development of VTE has been well summarized by Fox and Kahn systematic review. 21 They concluded that CRP could not be used as an appropriate factor for prediction and diagnosis of VTE. This is due to the relatively low positive and negative predictive values of CRP in this condition as well as the potential lethal nature of VTE that requires the tests with about 100% accuracy. However, CRP could be a best indicator of treatment response in case of VTE. 21 In our study, a significant reduction in hs-CRP was seen in both groups. Although the amount of this reduction was more in the intervention group, it was not significant. Anticoagulation therapy and consequent reduction in thrombosis and inflammation may partially justify this observation. Therefore, our study could not support the additional benefit of vitamin D plus anticoagulation therapy in the reduction in CRP in case of VTE.
Several studies have described the role of P-selectin in the development of VTE. A prospective cohort study of patients with cancer showed that the high level of P-selectin is linked with the incidence of VTE (hazard ratio = 2.6, 95% CI, 1.4-4.9, P = .003). 12
Accordingly, Ramacciotti et al 14 in a prospective study on patients with DVT showed that P-selectin could be implicated as a biomarker of thrombosis with the high sensitivity and specificity when combined with Wells criteria (P-selectin cut-point ≥ 90 ng/mL and Wells scores ≥ 2). Recently, a meta-analysis of 11 studies showed that P-selectin significantly increases in patients with VTE (odds ratio [OR] = 2.89, 95% CI = 2.31-3.61, P < .001) or with DVT only (OR = 2.64, 95% CI = 1.95-3.56, P < .001). 15
It has also been shown that the reduction in P-selectin level could improve the resolution of thrombosis. In this regard, Myers et al 16 in a mouse ligation model of venous thrombosis showed that the oral administration of P-selectin inhibitor (PSI-697) produces a significant reduction in thrombosis burden. The other study in baboon model of DVT indicated the prophylactic role of P-selectin inhibitor PSI-421 in resolution of thrombosis. 17 Also, Ramacciotti et al 18 in a meta-analysis of animal models of thrombosis suggested that inhibition of P-selectin may result in thrombosis resolution without need to expansion of bleeding time as well as without more complications.
Furthermore, reduction in P-selectin previously has been reported by some medications. A number of studies significantly described a lower level of P-selectin in statin-treated individuals with coronary artery disease. 24,25 The significant reduction in P-selectin by a 7-day therapy with heparin was also reported in patients with vascular thrombotic diseases. 26 Moreover, smoking could influence the plasma level of P-selectin. 27 The significant reduction in P-selectin by ergocalciferol was reported in a pilot study of Assimon et al. 22 They investigated ergocalciferol on 40 hemodialysis patients receiving active form of vitamin D. However, the effect size of this reduction was not identified in their study.
Antithrombotic activity of vitamin D has been described by several studies. Remarkably, in a placebo-controlled randomized trial on patients with prostate cancer, high-dose calcitriol therapy independently reduced thrombotic events (2 versus 11 events). 5 Lindqvist et al 3 in a study on 29 000 Swedish individuals suggested “D-lightful” theory. They showed that the risk of thrombosis increases by 50% during the winter in comparison to the other seasons. They concluded that an adequate sun exposure (ultraviolet B radiation) could reduce the risk of venous thrombosis by production of vitamin D and improving the level of anti-inflammatory and antithrombotic cytokines as well as enhancing the anticoagulant properties.
As mentioned earlier, the main suggested mechanisms for antithrombotic activity of vitamin D include “upregulation of thrombomodulin” 7,28 and “down-regulation of TF.” 7 Furthermore, data have indicated that vitamin D increases the level of anti-inflammatory cytokine IL-10 with antithrombotic activity. 6,9
Interestingly, McInnes et al 29 in a double-blind, placebo-controlled study examined the impact of IL-10 in patients with psoriatic arthritis and showed a significant reduction in plasma P-selectin by a 28-day therapy with IL-10. Moreover, Zingarelli et al 30 showed a significant increase in expression of P-selectin in IL-10–deficient mice in comparison to its wild types. Therefore, it may be speculated that vitamin D may reduce P-selectin through the upregulation of IL-10.
Taken together, despite the possible mechanisms regarding the reduction in P-selectin by the supplementation of vitamin D, our study could not support this hypothesis.
The results of this study can be partially justified by some reasons. First, based on the literature, time to plasma peak of 25(OH)D after intramuscular injection of high-dose vitamin D3 is about 2 to 4 months that is longer than our study period. 31,32 However, data have indicated that the single dose of vitamin D3 could increase the level of 25(OH)D to the level of above 30 ng/mL (vitamin D sufficiency) in a less than 1-month period. 31 Second, in our study, despite the significant increase in 25(OH)D level from 16.9 ± 11.6 ng/mL to 20.7 ± 14.1 ng/mL after injection of 300 000 IU vitamin D3, it remained in the range of insufficiency. Hence, this level of 25(OH)D may not be effective for reduction in P-selectin. Third, this pilot study is the first one, which was designed to investigate the effect of high-dose vitamin D on P-selectin as a marker of thrombosis as well as included small sample size. As a result, larger studies with higher doses and longer duration may show better potential benefit of vitamin D3 supplementation on plasma level of P-selectin in patients with VTE.
Limitations
This study included some limitations. First, intramuscular administration of vitamin D made us unable to use the placebo in the control group. Second, the study had partially a small sample size. Third, we had cost and time limitations and could not follow up the patients more than 1 month as well as regarding the clinical significance.
In conclusion, this study could not support the potential benefit of the high-dose vitamin D on plasma level of P-selectin and hs-CRP in patients with VTE. Therefore, our study showed that vitamin D plus anticoagulants did not have a greater effect than anticoagulants alone in the case of VTE. Further studies are recommended to investigate the effect of vitamin D on plasma level of P-selectin in patients with VTE, especially with respect to the clinical significance.
Footnotes
Acknowledgments
This work is the result of a PhD student thesis and we would like to thank the office of Vice-Chancellor for Research of Tehran University of Medical Sciences for supporting of the study (grant number: 91-02-33-18319). The authors would also like to express their deep appreciation to laboratory, emergency room, and clinic of warfarin stuffs of Tehran Heart Center who sincerely accompanied us for doing this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.