
Abstract
Background:
Disparities in home dialysis uptake across England suggest inequity and unexplained variation in access. We surveyed staff at all English kidney centres to identify patterns in service organisation/delivery and explore correlations with home therapy uptake, as part of a larger study (‘Inter-CEPt’), which aims to identify potentially modifiable factors to address observed variations.
Methods:
Between June and September 2022, staff working at English kidney centres were surveyed and individual responses combined into one centre-level response per question using predetermined data aggregation rules. Descriptive analysis described centre practices and their correlation with home dialysis uptake (proportion of new home dialysis starters) using 2019 UK Renal Registry 12-month home dialysis incidence data.
Results:
In total, 180 responses were received (50/51 centres, 98.0%). Despite varied organisation of home dialysis services, most components of service delivery and practice had minimal or weak correlations with home dialysis uptake apart from offering assisted peritoneal dialysis and ‘promoting flexible decision-making about dialysis modality’. Moderate to strong correlations were identified between home dialysis uptake and centres reporting supportive clinical leadership (correlation 0.32, 95% Confidence Interval (CI): 0.05–0.55), an organisational culture that values trying new initiatives (0.57, 95% CI: 0.34–0.73); support for reflective practice (0.38, 95% CI: 0.11–0.60), facilitating research engagement (0.39, 95% CI: 0.13–0.61) and promoting continuous quality improvement (0.29, 95% CI: 0.01–0.53).
Conclusions:
Uptake of home dialysis is likely to be driven by organisational culture, leadership and staff attitudes, which provide a supportive clinical environment within which specific components of service organisation and delivery can be effective.
Background
Home dialysis is associated with multiple potential benefits for patients, including the potential for improved quality of life, 1 greater satisfaction with treatment, 2,3 equivalent survival to in-centre dialysis 4 and potential cost savings to services. 5,6 Consequently, there is an increasing focus on improving access to home dialysis in England, driven by clinical guidelines, 7 the National Kidney Federation 8 and the GIRFT (Getting It Right First Time) initiative, 9 which recommended that at least 20% of the prevalent dialysis population at each kidney centre should be peritoneal dialysis (PD) or home haemodialysis (HHD). Increasing engagement with home dialysis is also one of the identified priorities for the Renal Services Transformation Programme. Despite this, rates of home dialysis uptake remain low. There are substantial variations in uptake by ethnicity 10 and socio-economic status 11 in England, a trend reflected internationally. 12 There are also large differences between kidney centres (centre variation) in the overall uptake of home therapies. In 2021, the proportion of incident kidney replacement therapy (KRT) patients initiating PD ranged from 8.2% to 45.5% by centre in England (mean 21.7%) and from 0% to 6.8% for HHD (mean 0.7%; home therapies mean 22.4%). 13 The same variations are evident in the prevalent KRT population, with the proportion of patients on PD by centre ranging from 6.0% to 25.9% (mean 13.4%) and from 0% to 14.4% for HHD (mean 4.7%; home therapies mean 18.1%). 13 Around one-third of centres (16 out of 49) currently meet the 20% target for prevalent home dialysis use. Current data on PD and HHD uptake therefore demonstrate unexplained variation in access to home dialysis across England, which is a recognised contributor to kidney health equalities. 14
Numerous factors can affect home dialysis uptake. For patients, uptake may be influenced by the organisation of pre-dialysis education, communications with healthcare professionals, personal support systems, personal views/priorities and the availability of ongoing psychosocial support. 15,16 At the centre level, home dialysis uptake may be affected by staff training/capacity, 17 institutional culture 18 and the relative cost of in-centre versus home therapies. 6 Centre-level performance is also influenced by policy factors, local resources, centre volume, transplantation rates and transfer rates from home to in-centre haemodialysis. 19 Given this complexity, understanding the drivers of unexplained variation between centres requires an in-depth exploration of cultural, service and organisational factors operating at the centre level and how these may affect engagement with home dialysis. The Inter-CEPt study, 20 funded by the UK National Institute for Health and Care Research, used a mixed methods approach to investigating the organisational and cultural factors that contribute to centre variation in home dialysis uptake in England, in order to identify potentially modifiable factors that could address this variation. Informed by earlier work within this programme, we report a cross-sectional survey of staff at all English kidney centres (n = 51) which aimed to identify patterns in centre practice and home dialysis service organisation and explore correlations with home dialysis uptake at the centre level.
Methods
In this article, survey methods are reported using the CROSS checklist for reporting of survey studies. 21
Survey development
The survey was developed using multiple methods. First, a review of the literature on dialysis provision identified key points in the patient journey at which dialysis modality may be discussed, alongside known factors that may affect home dialysis choice. Three members of the research team (JF, ML and SJD) are clinicians who work in centres offering home dialysis, so survey development drew on their knowledge about the delivery of kidney services in England to identify additional areas of questioning. Our patient representative (DC) and Patient Advisory Group (PAG), which comprised a diverse group of eight individuals with lived experience of chronic kidney disease and dialysis, also had direct input into defining the relevant issues for inclusion in the survey through dedicated meetings. Further to this, we incorporated the findings from a focused ethnographic study of the centre-level factors that may affect home dialysis uptake which formed the initial phase of the Inter-CEPt study. This was undertaken in four kidney centres across England with above-average home dialysis uptake and included participant observation of patient consultations and interviews with patients and kidney unit staff. Once a long list of candidate survey questions had been compiled, this was refined by all authors through iterative discussion, in order to derive the final list of survey questions, their specific wording and the most appropriate order in which questions should be asked. The draft survey was reviewed for relevance by our independent study oversight committee (which included kidney clinicians and methodological experts) and was reviewed for comprehension and readability by the PAG. The survey was not piloted prior to administration.
Survey design and administration
The survey was disseminated using the JISC Online Surveys tool (https://www.onlinesurveys.ac.uk) and comprised 78 questions across 12 sections covering key aspects of kidney service organisation and delivery including pre-dialysis education, training, support for dialysis modality choice, clinical leadership, finance and commissioning/service planning (Table 1; full survey available in Online Supplementary Material). Survey questions required dichotomous answers, selection of one or more options from a list or five-point Likert scale responses assessing respondent agreement with statements about specific aspects of service organisation/delivery.
Survey sections and examples of content covered by section.
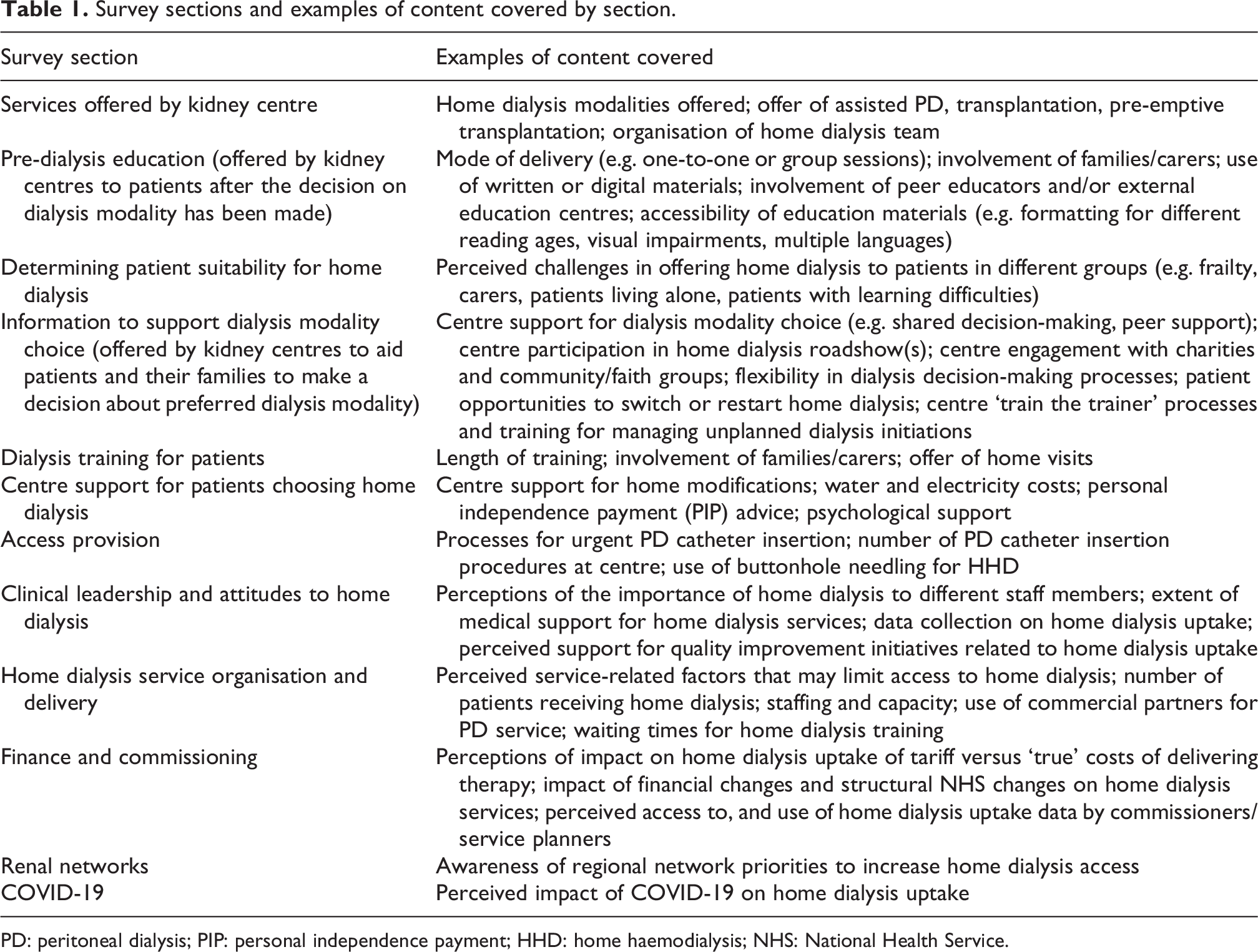
PD: peritoneal dialysis; PIP: personal independence payment; HHD: home haemodialysis; NHS: National Health Service.
The survey target population included all staff involved in providing home dialysis services at each kidney centre in England including centre managers, clinical directors/clinical leads (individuals with responsibility for the entire kidney centre), PD and HHD lead physicians and nurses (consultant physicians and nurses who lead the PD or HHD elements of the kidney centre service) and Advanced Kidney Care (AKC) clinic staff. There was no purposeful sampling of individuals across roles, as we sought to obtain responses from individuals in multiple roles from each centre to ensure a range of expertise and perspectives was represented and to minimise non-response. The survey opened in June 2022, with a secure survey weblink and covering email sent to clinical leads at each kidney centre in England (n = 51) for onward dissemination to all relevant staff at their centre. To minimise respondent burden, the survey was designed so that staff from each relevant role within a centre saw only the questions relevant to their role once they had indicated this. Surveys took up to 25 min to complete depending on staff role, and respondents received a £25 voucher to thank them for their time. This along with the requirement to record their kidney centre and specific role prevented multiple completion of the survey by the same individual. No personal data were collected beyond centre and role to ensure respondent anonymity. A reminder email/weblink was sent to clinical leads after 4 weeks if there had been no response from their centre or if responses had been received from limited staff roles. The survey closed in September 2022.
Data analysis
Individual-level responses were combined into a single centre-level response for each survey question using predetermined, pragmatic rules for data aggregation. For example, if a survey question had been answered by a single individual at a centre, their response was used as the centre response for that question. Where multiple individuals had responded to a dichotomous or option selection question from the same centre, the modal response was taken (e.g. if three respondents indicated that their centre offered peer support and one respondent said that peer support was not offered (or selected the ‘not sure’ option), that centre would be recorded as offering peer support). Where multiple individuals had responded but there was no unique modal response, the answer given by the most relevant staff role was taken (e.g. nurse responses for clinical questions prioritised over responses from centre managers). In the case of Likert scale questions, responses were converted into a scale from 0 to 100 and an aggregate mean ‘agreement’ score calculated so that answers from all staff could contribute to the centre response (e.g. ‘strongly disagree’ = 0; ‘disagree’ = 25; ‘neither agree nor disagree’ = 50; ‘agree’ = 75; ‘strongly agree’ = 100. If four individuals had answered the question, one of whom disagreed, one agreed and two strongly agreed, the mean ‘agreement score’ for this question would be 25 + 75 + 100 + 100/4 = 75 out of 100).
Data were analysed descriptively to characterise how home dialysis services were organised and delivered by responding kidney centres. Centre practice was also explored through comparison of proportion tests (categorical variables) and pairwise Pearson correlations (continuous variables) between specific aspects of practice and home dialysis uptake by centre. Uptake for each centre was determined using UK Renal Registry (UKRR) incidence data reporting the proportion of patients who started home dialysis (PD and HHD) within 12 months of KRT initiation using data from the most recent complete year available at the time (2019). 22 This outcome was chosen to accommodate late presenters and to allow for the fact that in many centres, the required time for commencing HHD necessitates an initial period of in-centre haemodialysis. Clinical leads and specific staff members in individual centres were recontacted by email and asked for ad hoc responses to questions with non-response from their centre. Non-responder analysis used independent t-tests to compare mean uptake of home dialysis at kidney centres who responded to each survey question against mean uptake at centres that did not respond. This assessed whether there were systematic differences in home dialysis uptake between centres according to non-response data for each survey question. Statistical analyses were performed using SPSS version 29 (2022; IBM Corp, Armonk, New York, USA).
Ethical approval and consent to participate
Ethical approval was obtained from the Wales Research Ethics Committee (Ref 20/WA/0249) on 18th September 2020. Formal consent to participate in the survey was indicated by all respondents via an embedded consent form and agreement to participate. Potential respondents who did not answer the mandatory consent questions at the start of the survey were unable to proceed any further.
Results
Responses
A total of 180 responses were received from 50 of the 51 English kidney centres (98.0%). Of the 180 individual responses, nurses responded in the greatest numbers (n = 58; 32.2%), followed by AKC clinic staff (n = 41; 22.8%), clinical leads (n = 37; 20.6%), physicians (n = 35; 19.4%) and centre managers (n = 9; 5.0%). There were between 1 and 10 responses from each centre (mean 3.5), and between 1 and 7 staff roles represented at each centre (mean 3.2). The proportion of survey questions with a response from each centre ranged from 22.4% to 100% (mean 72.3%). Non-responder analysis showed no systematic difference in the proportion of patients using home therapies between responding and non-responding centres for each survey question.
Kidney centre organisation
Eighteen centres described themselves as a transplant centre (36.0%). All responding centres offered PD, and all but one offered HHD. Eighty-four per cent of responding centres (42/50) offered assisted PD, and 17/32 responding centres reported that their home dialysis team was organised as separate for PD and HHD rather than combined. Having one individual as a combined lead for PD/HHD was associated with significantly lower home dialysis rates (combined lead 24.3%; separate organisation 32.9%; p = 0.031). Centres offering assisted PD had significantly higher home dialysis uptake than those that did not offer assisted PD (26.5% vs. 15.6%; p = 0.007). All responding centres offering assisted PD did so for frail elderly patients; 94.3% (n = 33) offered assisted start PD and 91.4% (n = 33) offered it as respite. Most centres reported using commercial partners to deliver assisted PD services (71.4%; n = 25), whereas 10 centres offered services in-house (28.6%). There was no association between mode of assisted PD delivery and home dialysis uptake.
Pre-dialysis education organisation/delivery
Table 2 describes the proportion of centres that reported offering specific support in the way that pre-dialysis education was organised and delivered. Percentages relate to the proportion of centres that answered a given survey question. All responding centres offered written materials and one-to-one sessions with a healthcare professional as part of pre-dialysis education for the person with kidney failure. Patient education at home was offered by 72% of responding centres. Peer educators (44.0% of centres) and external education centres (32.0%) were used least frequently. All responding centres allowed families/carers to attend consultations where dialysis modality was discussed. Less than half of centres offered family/carer specific education sessions (38.5%), family/carer specific information materials (45.8%) or family/carer peer support (20.0%). Most responding centres used interpreters (92.0%) and/or reviewed written resources for accessibility (84.0%). More than half of centres gave opportunities for peer support (61.9%) and/or had written materials available in multiple languages (63.6%). Less common was having written resources formatted for visual impairments (45.5%), different reading ages (33.3%) or video/DVD resources with captions (17.4%) or in multiple languages (8.3%).
Organisation and delivery of pre-dialysis education.
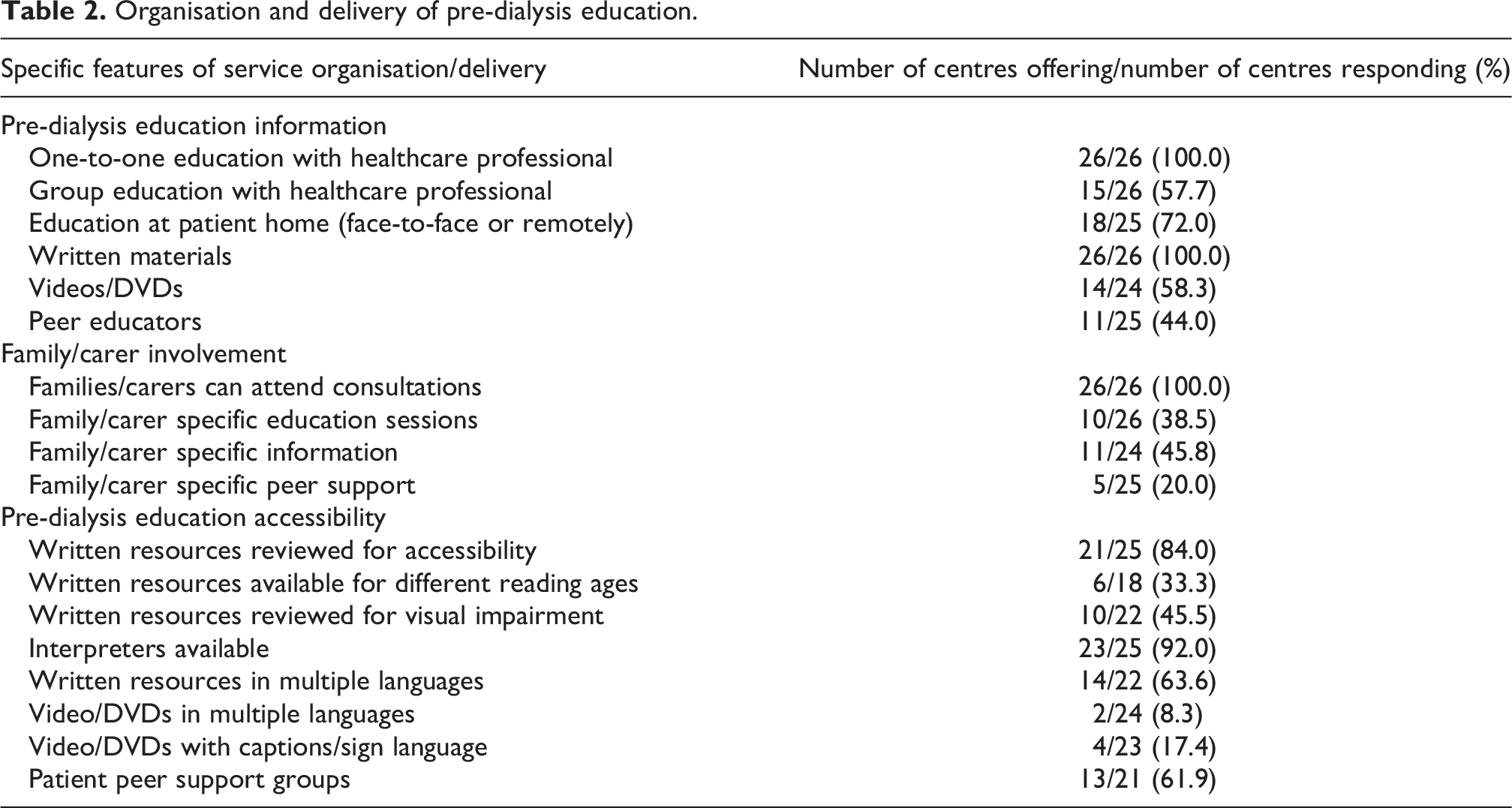
There was no correlation between home dialysis uptake (proportion of incident dialysis starters at each centre treated with PD/HHD at 12 months) and the presence or absence of any aspects of pre-dialysis education organisation/delivery listed above.
Centre support for dialysis modality choice
Table 3 shows the proportion of responding centres that reported offering specific support for patients in making choices about their preferred dialysis modality. Clinical props were used by all centres. Engagement with kidney charities (96.0%) and using information from external sources (96.0%) were also widely reported. Least commonly used were peer support (73.1%) and tools for shared decision-making (65.4%). Signposting and support/advice was commonly reported by responding centres, with advice for working age patients, advice on Personal Independence Payment claims, council tax reduction, support with water and electricity costs and/or priority services registration offered by 86% or more of the 50 centres who answered this question. Access to a renal psychologist (60.0% of centres), support with home modifications for home dialysis (58.0%) and access to social care support (50.0%) were reported least frequently. Sixteen kidney centres had hosted a home dialysis roadshow since 2016 (32.0%). Finally, there were high levels of agreement from respondents that their centre offered flexibility to patients in the dialysis decision-making process along with opportunities to switch modality or restart home dialysis under specific circumstances.
Centre support for dialysis modality choice.
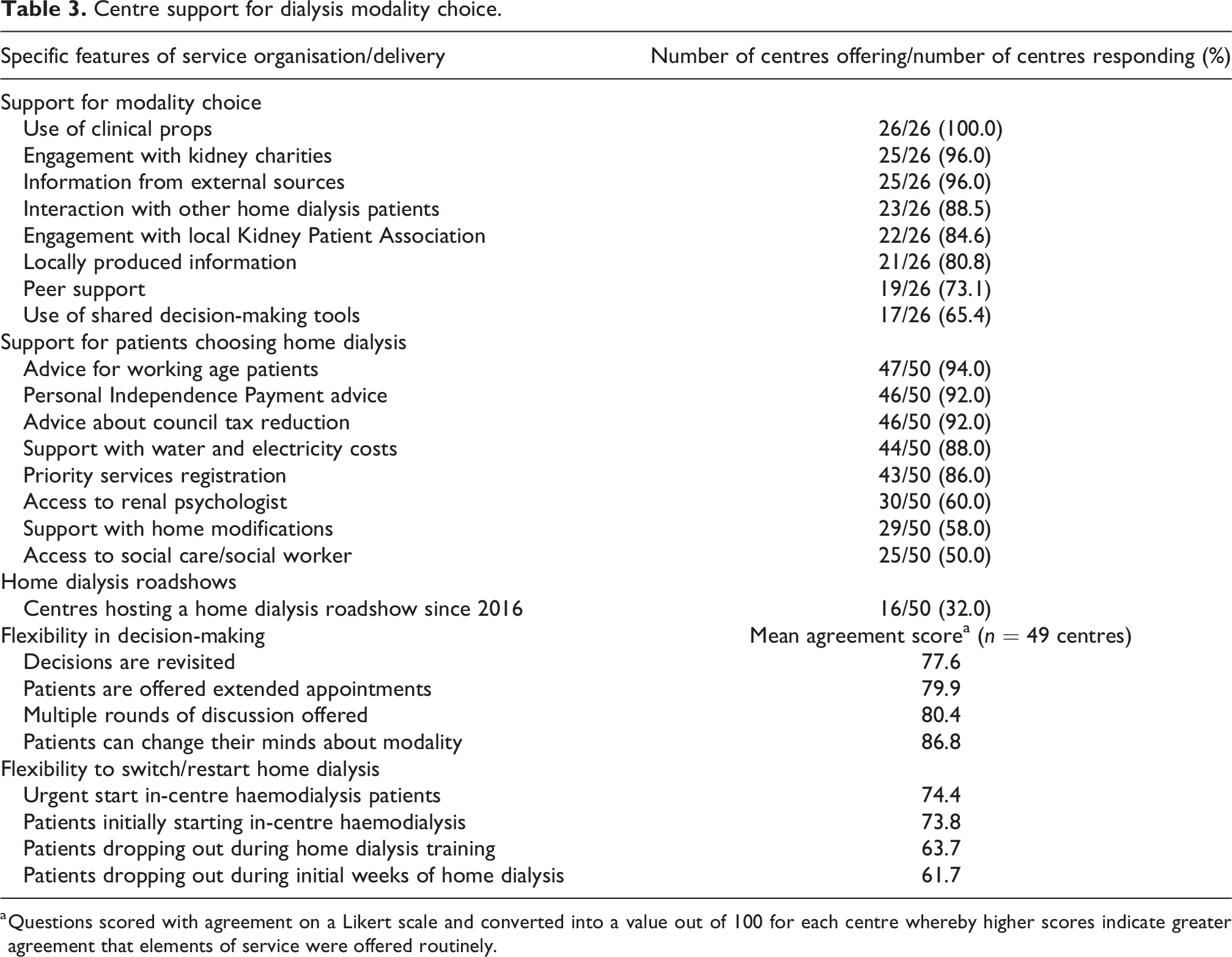
a Questions scored with agreement on a Likert scale and converted into a value out of 100 for each centre whereby higher scores indicate greater agreement that elements of service were offered routinely.
In relation to centre support for dialysis modality choice, there was no correlation between home dialysis uptake and the presence or absence of specific aspects of service organisation/delivery. However, higher agreement scores in relation to giving patients the opportunity to ‘restart home dialysis if they dropped out in the initial weeks of treatment’ were moderately correlated with higher home dialysis uptake (correlation coefficient 0.32, 95% CI: 0.04–0.56).
Length of dialysis training and access provision
The median length of PD training duration was 3 days (n = 32 centres, IQR 3–5, range 1–14). There was a weak negative correlation between length of training and PD uptake (i.e. a higher proportion of patients on PD was seen in centres with shorter training length (coefficient: −0.31, −0.59 to 0.04). The median length of HHD training was 6 weeks (n = 33 centres, median 4 to 8, range 2 to 14). There was a weak correlation between HHD uptake and training length (0.20, 95% CI: −0.16 to 0.51). In terms of catheter/vascular access, there was no difference in PD uptake between centres that reported having a medical pathway for PD catheter insertion (57.1%; n = 28) and those that did not (42.9%; n = 21). For HHD, there was no difference in uptake between centres who reported a low rate (<20%) of using buttonhole needling for vascular access (mean uptake 4.6%, 17 centres), compared to centres that reported a high rate (80%+) (mean uptake 4.9%, 8 centres).
Clinical leadership and staff attitudes to home dialysis
There were a number of moderate to strong correlations between centre home dialysis uptake and staff attitudes to clinical leadership, quality improvement (QI) and the perceived influence of finance/commissioning on home therapies engagement (n = 50 centres) (Table 4). The perceived strength of clinical leadership was positively correlated with home dialysis uptake (i.e. the more important home dialysis was thought to be for clinical leads, the greater the home dialysis uptake by a centre (correlation coefficient 0.32, 95% CI: 0.05–0.55)).
Correlations between centre staff attitudes to home therapies and home dialysis uptake.
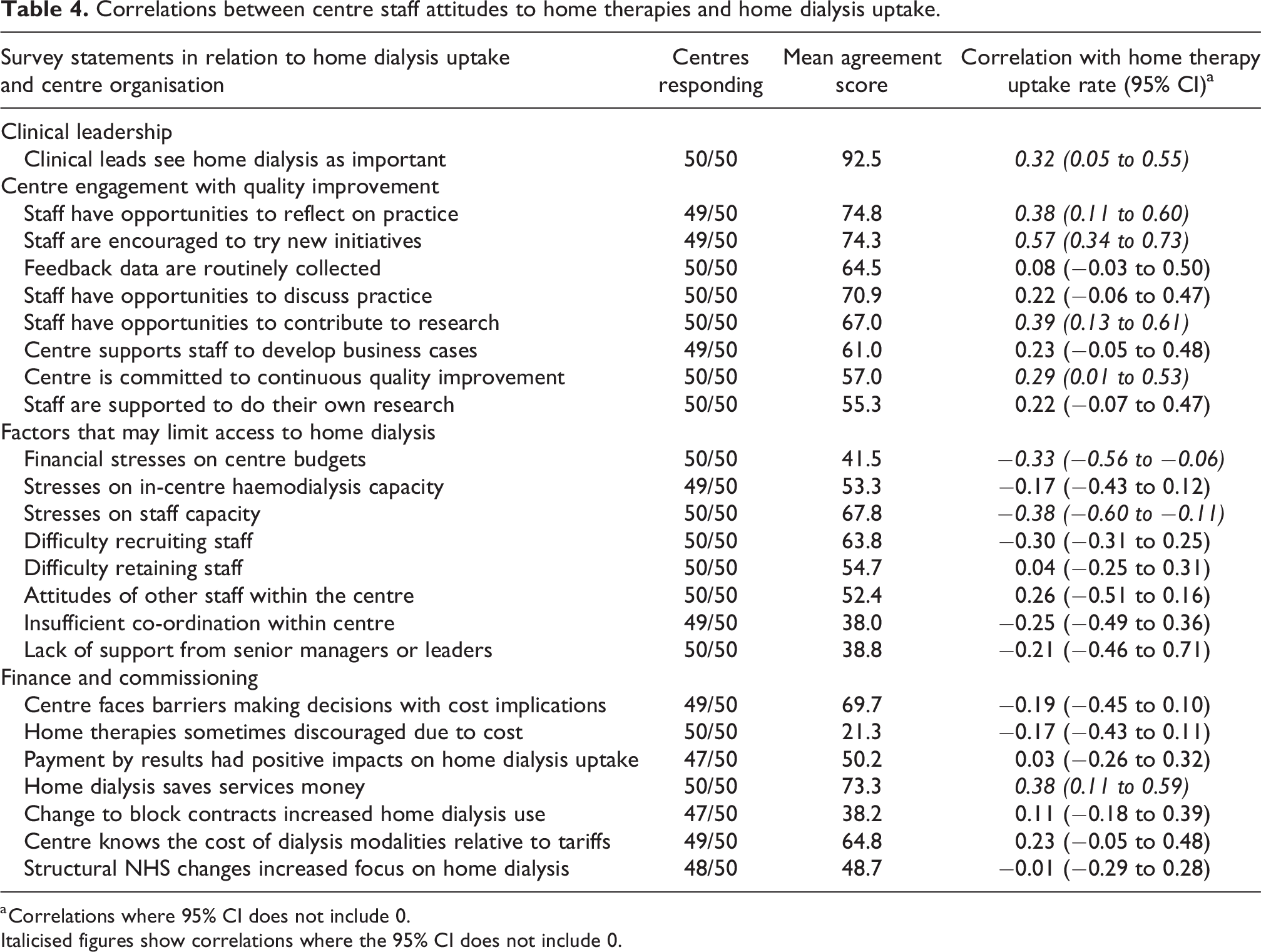
a Correlations where 95% CI does not include 0.
Italicised figures show correlations where the 95% CI does not include 0.
The strength of centre engagement with key elements of continuous QI also showed moderate to strong correlations with higher home dialysis uptake: uptake was higher in centres where staff reported being given opportunities to reflect on practice (0.38, 95% CI: 0.11–0.60); encouraged to try new initiatives (0.57, 95% CI: 0.34–0.73), where there are opportunities for staff to participate in research (0.39, 95% CI: 0.13–0.61) and where the centre had a perceived commitment to continuous QI (0.29, 95% CI: 0.01–0.53). All of these elements of centre organisation and engagement with QI were correlated (strong to very strong correlations) with each other (Table 5), with the exception of clinical leadership.
Cross-correlation matrix between discrete elements of centre practice relating to quality improvement and clinical leadership.
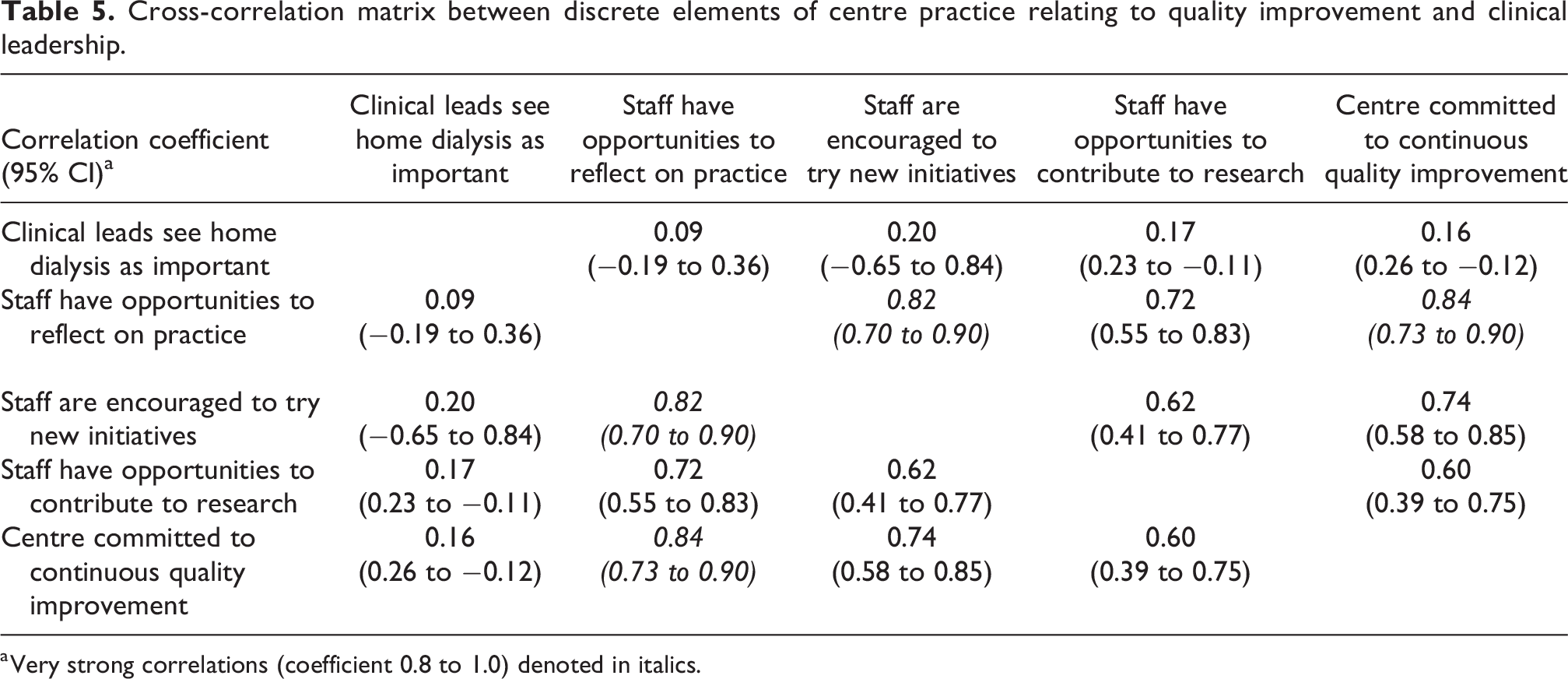
a Very strong correlations (coefficient 0.8 to 1.0) denoted in italics.
Home dialysis uptake was also higher in centres that perceived home dialysis to be cost saving (0.38, 95% CI: 0.11–0.59). Financial stresses on centre budgets (−0.33, 95% CI: −0.56 to −0.06) and perceived stresses on staff capacity (−0.38, 95% CI: −0.60 to −0.11) were both negatively correlated with home dialysis uptake.
Discussion
This national survey is, to our knowledge, the first to assess multiple elements of kidney centre practice in relation to home dialysis service organisation and delivery in England and to explore associations with home dialysis uptake at the centre level.
Survey data showed substantial variation in centre practice in the organisation and delivery of pre-dialysis education, centre support for dialysis modality choice, engagement with charities/community groups, use of peer support and support/advice offered to patients choosing home dialysis. Many kidney centres followed good practice in helping patients make decisions about dialysis modality, including the promotion of equity and accessibility by using interpreters, providing information in multiple languages and engaging with charities and local Kidney Patient Associations. However, only two aspects of practice/service delivery were associated with home dialysis uptake. The first was an association between the offer of assisted PD and higher home dialysis uptake. In the United Kingdom, assisted PD is funded by an additional NHS tariff to support its delivery, with services usually delivered by healthcare assistants, either employed directly by NHS Trusts to provide an ‘in-house’ assisted PD service, or via private commercial companies where in-house provision is not offered. Numerous studies have argued that assisted PD provision is essential to facilitate home dialysis access for older patients or those with comorbidities. 23 –25 Our data showed that the offer of assisted PD was widespread in England (42/50 centres), which supports the argument that offering assisted PD may contribute to significantly higher uptake at the centre level, although uncertainties remain about the cost-effectiveness of this. 26 The only other service-related factor significantly correlated with home dialysis uptake was the promotion of flexibility in dialysis decision-making, specifically in relation to the regular reviewing/revisiting of decisions about dialysis modality with patients.
Whilst barriers to home dialysis use are known to be multi-level including a lack of appropriately trained staff, 27 limited funding to increase the home therapy offer 28 and the influence of wider policy factors, 29,30 our survey data suggest that, in contrast to the paucity of service-related factors associated with home dialysis engagement, uptake is most likely to be influenced by a kidney centre’s clinical leadership and organisational culture. The concept of organisational culture is difficult to define, 31 but centres in which staff reported strong clinical leadership in relation to home therapy support, and which valued trying new initiatives, staff research participation, reflective practice and engagement with continuous QI were likely to have significantly higher home dialysis uptake than centres where these factors were less frequently reported. With the exception of clinical leadership, which appeared to be associated with home dialysis uptake independently of other cultural factors, aspects of organisational culture were strongly correlated with each other, providing additional evidence that having a supportive and positive centre culture is a key driver of home dialysis engagement at the centre level.
These findings suggest that any intervention designed to increase centre engagement with home dialysis should (at least in part) target the culture of kidney staff teams. 32 It is likely that receptive institutional cultures and supportive clinical leadership can combine to provide a supportive clinical environment within which specific components of service organisation and delivery can be deployed effectively to facilitate home dialysis uptake. 33,34 Whilst other work has explored the determinants of organisational culture in kidney centres and their potential impact on centre support for home dialysis, 35 this work has been largely qualitative and has not assessed associations with home dialysis uptake. Understanding organisational culture in kidney centres has been highlighted as a research priority in relation to home dialysis uptake, 19 and our data underline the importance of this. The potential role of strategic direction and leadership also reflects themes identified by GIRFT and other initiatives. 9,19,36 Subsequent analyses for the Inter-CEPt study (to be reported separately) will link the survey findings to UKRR individual-level patient outcome data to quantify how different factors may influence home dialysis uptake in the context of alternative treatment and related clinical outcomes and to identify candidate modifiable factors for an intervention bundle to address unexplained variation in home dialysis uptake between kidney centres.
Strengths and limitations
The depth of our analysis was limited by the nature of the survey data. For example, because some survey questions were only posed to staff performing specific roles, if these staff members did not respond to the survey from a given centre, this led to non-response. However, non-responder analysis for each survey question showed no systematic difference in home dialysis uptake between centres with missing data and those without. We also sought to minimise non-response by recontacting clinical leads and key staff members at specific kidney centres for additional answers to fill important gaps.
Our analysis was descriptive, and we could not adjust for potential confounding factors on home dialysis uptake at the centre level. Consequently, where associations were not found, this does not necessarily mean that a given aspect of practice was unimportant in potentially affecting home dialysis uptake. There is also a risk of measurement error when using pragmatic approaches to resolve apparently contradictory responses from multiple staff at a kidney centre in order to derive a single ‘centre response’. Contradictory responses may be due to social desirability bias, with some respondents overstating the extent of good practice at their centre, or those with negative views being less willing to express these. There may also be variations in practice across the same kidney centre if it covers a broad geographical area and encompasses diverse patient profiles. This may impact on the degree to which we were able to find concordance of views and practice within some kidney centres and may also hide trends linked to regional clustering, particularly in relation to the importance of ‘external’ influences on home dialysis uptake such as the regional kidney networks. These issues will be explored further in subsequent analyses.
Conclusions
Unexplained centre-level variation in access to home therapies is a recognised contributor to kidney health inequalities in England. Our survey shows that it is likely that positive centre engagement with home therapies is driven primarily by organisational culture, leadership and staff attitudes towards home dialysis. These factors combine to provide a supportive clinical environment within which specific components of service organisation and delivery are more likely to be effective in facilitating home therapy uptake at the centre level.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241232200 - Centre variation in home dialysis uptake: A survey of kidney centre practice in relation to home dialysis organisation and delivery in England
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241232200 for Centre variation in home dialysis uptake: A survey of kidney centre practice in relation to home dialysis organisation and delivery in England by Sarah Damery, Mark Lambie, Iestyn Williams, David Coyle, James Fotheringham, Ivonne Solis-Trapala, Kerry Allen, Jessica Potts, Lisa Dikomitis and Simon J Davies in Peritoneal Dialysis International
Supplemental material
Supplemental Material, sj-docx-2-ptd-10.1177_08968608241232200 - Centre variation in home dialysis uptake: A survey of kidney centre practice in relation to home dialysis organisation and delivery in England
Supplemental Material, sj-docx-2-ptd-10.1177_08968608241232200 for Centre variation in home dialysis uptake: A survey of kidney centre practice in relation to home dialysis organisation and delivery in England by Sarah Damery, Mark Lambie, Iestyn Williams, David Coyle, James Fotheringham, Ivonne Solis-Trapala, Kerry Allen, Jessica Potts, Lisa Dikomitis and Simon J Davies in Peritoneal Dialysis International
Footnotes
Acknowledgements
The authors would like to thank Fiona Loud (chair) and members of the study Oversight Committee for their generous support. The authors also thank the members of the Inter-CEPt Patient Advisory Group (PAG) for their input to and engagement with the study.
Author contributions
SD, ML, IW, KA, DC, IST, JF, LD and SJD are all co-applicants on the original funding application and conceived/developed the study. All authors contributed to the finalisation of the research protocol and ongoing execution of the research. DC is lead for Patient and Public Involvement and Engagement. ML, SJD and SD developed the initial draft of the survey, which was administered by SD with support from ML and SJD. SD performed survey data cleaning and data analysis. SD wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SJD (Chief Investigator) receives research funding and is on an Advisory Board for Baxter Healthcare and research funding from Fresenius Medical Care (both companies deliver dialysis treatments, including home dialysis). ML has received research funding from Baxter Healthcare and speaker honoraria from Baxter Healthcare and Fresenius Medical Care. JF has speaker honoraria from Fresenius Medical Care and Novartis and conducts research funded by the National Institute for Health Research, Kidney Research UK, the Health Foundation, Vifor Pharma and Boehringer Ingelheim into kidney disease.
Data availability
The data supporting the results of this study are available from the corresponding author on reasonable request.
Ethical approval
Ethical approval for this study was obtained from the Wales Research Ethics Committee (Ref 20/WA/0249) on 18th September 2020.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the UK National Institute for Health and Care Research (NIHR) Health Services & Delivery Research (HSDR) Programme (project reference 128364). The study sponsor (Keele University) and funder had no role in the study design, in the collection, analysis and interpretation of data, in the writing of this manuscript and in the decision to submit the manuscript for publication.
Informed consent to participate
Formal consent to participate in the survey was indicated by all respondents via an embedded consent form and agreement to participate. Potential respondents who did not answer the mandatory consent questions at the start of the survey were unable to proceed any further.
Informed consent to publish
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.