
Abstract
Background:
People treated with home dialysis report social and emotional isolation, fear of catastrophic events and concern about being a burden. There is a paucity of research exploring psychological well-being among consumers dialysing at home. We aimed to explore the psychological health issues related to home dialysis, and how these issues may impact on sustaining home-based treatment.
Methods:
We conducted a qualitative interview study with 36 consumers. We included patients with experience of home dialysis and caregivers. Thirteen participants had experienced peritoneal dialysis, seven home haemodialysis, seven had experienced both and nine caregivers. Data were analysed inductively to generate themes and a conceptual framework.
Results:
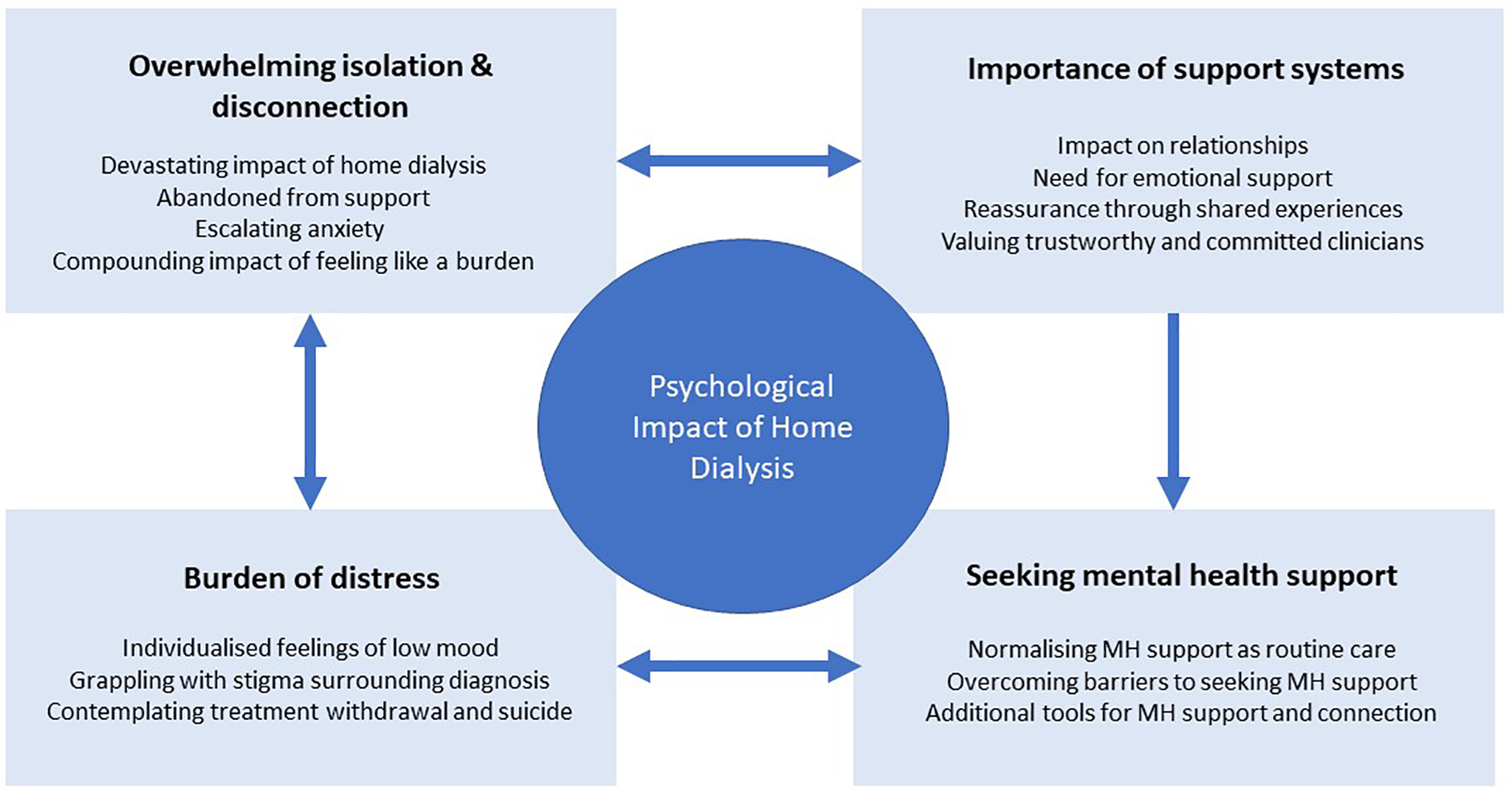
We identified four themes and subthemes: overwhelming isolation and disconnection (devastating isolation of home dialysis; abandoned from support; escalating anxiety; compounding impact of feeling like a burden); importance of support systems (impact on relationships; need for emotional support; reassurance through shared experiences; valuing trustworthy and committed clinicians); burden of distress (individualised feelings of low mood; grappling with stigma surrounding diagnosis; contemplating treatment withdrawal and suicide); seeking mental health support (normalising mental health support as a distinct entity in dialysis care; overcoming barriers to seeking mental health support; additional tools for mental health support and connection).
Conclusion:
Consumers may experience intense psychological distress during home-based dialysis care. Increasing clinician and health services literacy about the management of psychological impacts of home-based dialysis may improve consumer safety, quality of life and sustainability of home treatment.
Keywords
Introduction
Home-based dialysis is promoted globally to alleviate demand for, and costs of, facility-based dialysis care. Home dialysis prevalence varies across health systems from 71% of dialysis patients in Hong Kong to 14% in the United States, 1 in part due to practice norms, clinical infrastructure and service design and healthcare funding and reimbursements. 2
One-third of people treated with long-term dialysis experience depressive symptoms, 3 and many report severe psychological distress. 3,4 Anxiety is also common among those treated with dialysis. 5 Both anxiety and depression are associated with reduced quality of life. 6 Although patients doing home dialysis report freedom to maintain employment and improved flexibility and quality of life, they also experience social and emotional isolation, fear of catastrophic events and concern about being a burden to their family. 7,8
In the recently published ‘Kidney Disease: Improving Global Outcomes (KDIGO) Home Dialysis Controversies Conference’, it was identified that emotional preparedness and support is as important as educational preparedness for those looking to dialyse at home. 2 Despite this, however, there is little research that explores and documents the severity and impacts of home dialysis on psychological health and family and physical health. Providing safe and effective patient-centred care is a pillar of healthcare quality requiring understanding of all aspects of the consumer experience. Understanding these specific factors may be fundamental to providing high-quality care that supports patients’ confidence and agency to choose and sustain home dialysis. 9
Psychological and somatic effects of depression and stress can lead to the development of several complications in patients with kidney disease including lower quality of life and motivation to self-care, increased hospitalisation rates and increased cardiovascular risk and mortality. 10,11 We therefore conducted a qualitative interview study with consumers (patients and caregivers) to explore consumer psychological values, perspectives and experiences related to home dialysis.
Methods
We conducted an in-depth interview study according to the Consolidated criteria for REporting Qualitative research (COREQ) 12 and the consolidated criteria for strengthening reporting of health research involving indigenous peoples (CONSIDER) statement. 13
Participant recruitment and selection
We recruited consumers who are currently or have previously utilised home dialysis therapies. We invited consumers to participate via established peak patient support/advocacy groups (Kidney Health New Zealand [KHNZ] and the Auckland Dialysis Kidney Society) and dialysis services in Te Whatu Ora (the national health service of New Zealand) in Canterbury and the Hawke’s Bay. Participants were purposively sampled to include diverse demographic characteristics (age, sex and geographical remoteness) and modality of home dialysis (peritoneal dialysis and home haemodialysis). Of those who initially enquired about participation or were invited into the study, nine were not interviewed (one due to time constraints, three declined and the remainder were not able to be further contacted).
Two researchers conducted in-depth interviews until data saturation occurred. Data saturation was confirmed by regular discussion of the research team during the interview and recruitment process, and six further interviews were conducted to ensure diversity of age, sex and rurality. Participant recruitment began, and interviews were conducted between 16 March and 1 November 2022. The study was approved by the Eastern Institute of Technology Research and Ethics Committee (EA08260721). The participating hospital sites provided locality authorisation.
Design and setting
Due to restrictions and safety concerns related to the SARS-CoV2 pandemic, most interviews were conducted using videoconferencing or by telephone, based on participants’ preferences. The interview schedule contained open-ended questions exploring the participants’ psychological experiences of home dialysis (item S1).
Two authors conducted the interviews (RH and SH). Both are female and experienced and trained in qualitative research. RH is a social science researcher with formal training in clinical psychology. SH is a kidney nurse specialist with considerable previous experience in qualitative interviewing and home dialysis care. CW is an indigenous nephrologist and researcher who was involved in study design, conduct analysis and reporting. Initial interviews were conducted by RH and SH together to increase consistency of interviewing. The majority of the interviews were conducted by RH. All interviews were conducted in English. Interpreters and cultural support workers were offered to all participants but were not requested.
Interview length varied from 37 min to 132 min. Field notes were taken during each interview. All interviews were recorded and transcribed verbatim. Member checking of transcripts and draft themes was offered to participants to enable review and revision of the interpretation of findings. Of the eight participants who requested this, two replied with additional comments to add to transcripts and confirmed draft themes.
Data analysis
Transcribed interviews were imported into NVivo (QSR International Pty Ltd, version 11) and analysed using thematic analysis. 11,12 RCW developed a list of initial codes, then SCP trialled the codes on two transcripts, they then compared the application of coding and clarified before developing a codebook. The codebook was also discussed with the two interviewers, and consensus on the coding application was achieved. RCW and SCP then independently coded all transcripts, meeting regularly to discuss emerging patterns. Together, RCW and SP developed a preliminary thematic framework, which was reviewed and discussed by all other authors. The coding schema was refined through iterative discussions among all authors. CW provided indigenous cultural oversight during study conduct.
Results
Thirty-six consumers participated (aged from 24 years to 70+ years), including nine caregivers/partners. Table 1 provides the demographic characteristics of the 27 patient participants. Six couples were interviewed together, and an additional three people were interviewed on behalf of their partners who had experienced home dialysis. Of these three patient partners, one had dementia and two did not want to be interviewed. Twenty participants identified as female and 16 as male. Of the 27 patients interviewed, 13 had experienced peritoneal dialysis, 7 home haemodialysis and 7 had experienced both. Of the caregivers/partners interviewed, seven were female and two male, the average age was 60 and five of the nine were currently in paid employment. Four participants were interviewed face to face, 15 via videoconferencing and 7 via telephone.
Patient participant characteristics.
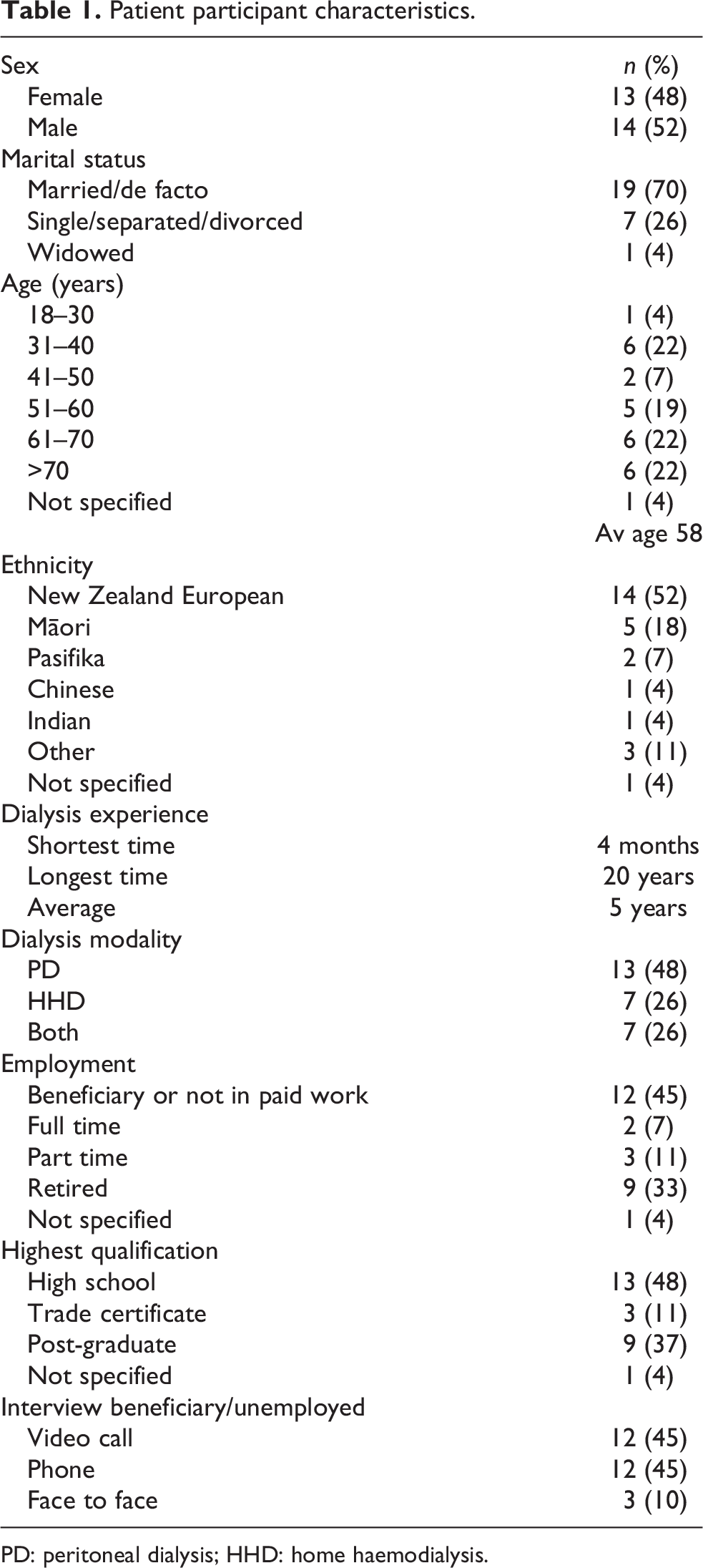
PD: peritoneal dialysis; HHD: home haemodialysis.
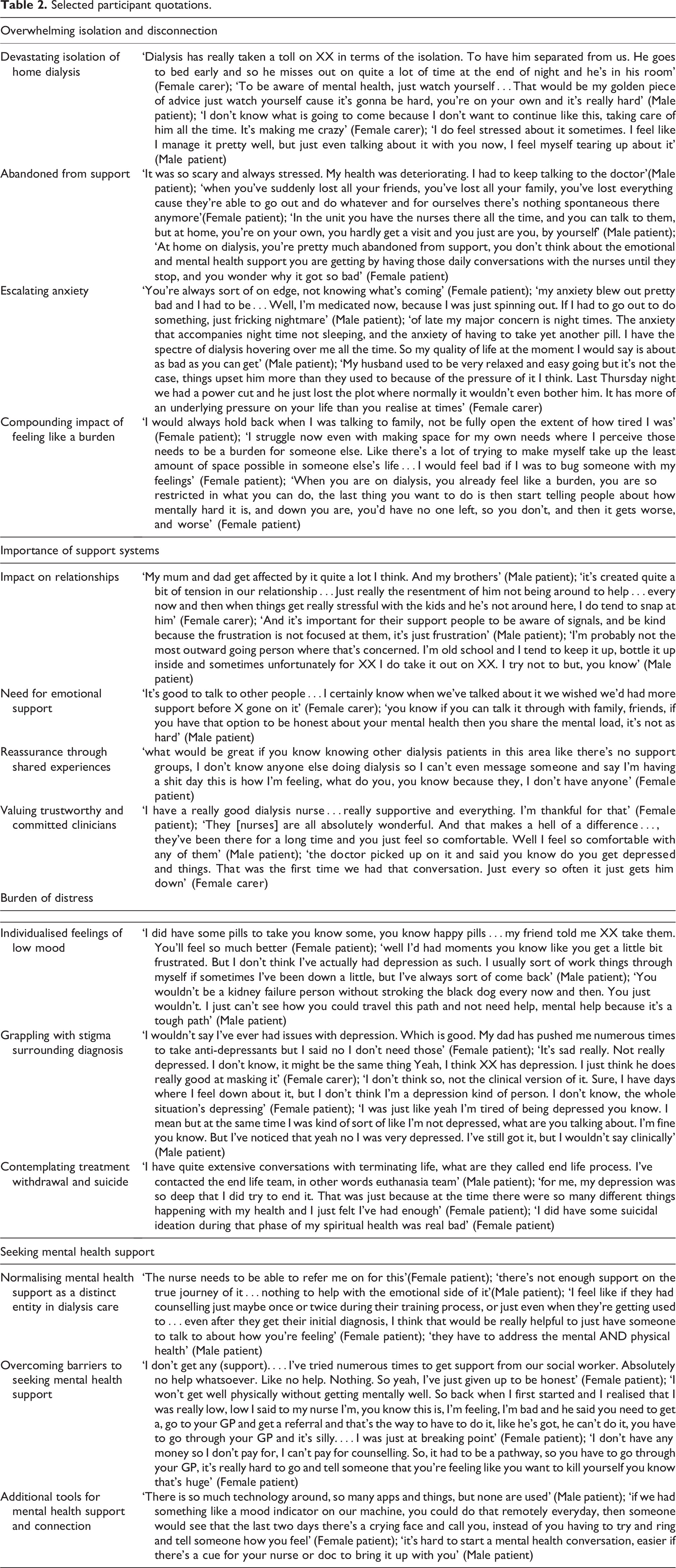
Four themes and related subthemes were identified: overwhelming isolation and disconnection (devastating isolation of home dialysis; abandoned from support; escalating anxiety; compounding impact of feeling like a burden); importance of support systems (impact on relationships; need for emotional support; reassurance through shared experiences; valuing trustworthy and committed clinicians); burden of distress (individualised feelings of low mood; grappling with stigma surrounding diagnosis; contemplating treatment withdrawal and suicide); seeking mental health support (normalising mental health support as a distinct entity in dialysis care; overcoming barriers of seeking mental health support; additional tools for mental health support and connection). These themes are shown within a conceptual framework (Figure 1). All themes and subthemes were discussed by both patients and caregivers/partners. Although caregivers did not discuss their own burden of distress, they did describe those of their partner. Themes and subthemes therefore represent both patients and caregivers, and if there were findings specific to either group, it is stated. Selected participant quotations representing each subtheme are detailed in Table 2.
Participants identified the overwhelming isolation and disconnection arising from dialysis treatment at home. This isolation was exacerbated by feeling abandoned by clinical staff and support systems, which in turn led to escalating and poorly controlled anxiety. Patients felt like a burden to family and carers and avoided discussing their psychological concerns. Unsupported and unspoken psychological distress further strained their support systems and directly impacted trust within their close relationships. Consumers additionally lost trust in their healthcare professionals and felt neglected by the health system. Conversely, support systems were central to emotional support and included peer support and trusted clinicians. Psychological experiences were sometimes constant and unrelenting and also could be a variable leading patients to doubt whether they had a problem or needed support. The burden of psychological and emotional distress was so severe that many patients contemplated ending their life or withdrawing from treatment. Stigma prevented patients from seeking mental health care and delivery of psychological care to dialysis patients was poor.
Selected participant quotations.
Overwhelming isolation and disconnection
Devastating isolation of home dialysis
Patients described an overwhelming sense of isolation on home dialysis. For some, this was based on being confined within their home. Caregivers also often felt left out from ‘normal activities’ and restricted in their social connections. Disconnection further exacerbated anxiety and ‘dark thoughts’ (participant 10). For those who had also experienced facility haemodialysis, the contrast of this with home dialysis and having no one to talk to while on dialysis was unrelenting. Participants who had been on home dialysis during Covid-19 discussed how periods of restrictions and lockdowns compounded their isolation from family, friends and peers, ‘the hardest part I think for me was “cause it was during Covid…” cause I wasn’t there to go and talk to some of the patients because of Covid and restrictions’ (participant 25).
Abandoned from support
Many participants felt abandoned by family, friends and healthcare staff, describing ‘being forgotten’ (participant 24) over time. Some felt that because others didn’t understand the emotional toll of home dialysis, it was difficult to talk about their emotions and ask for support, and when they did talk about their experiences, their friendships became strained and they ‘lost contact’ (participant 26a). Some participants discussed Covid-19 restrictions as further exacerbating this feeling of being abandoned as restrictions limited nurses and other supports from visiting them at home, ‘obviously with Covid there hasn’t been much of that calling in lately’ (participant 13).
Escalating anxiety
Home dialysis created ‘a lot of those little doubts and anxieties’ (participant 8). As this anxiety was not addressed, it escalated resulting in feeling ‘stressed about everything and always on edge’ (participant 5). This often resulted in a change in personality and how this ‘underlying pressure’ (participant 18) impacted their lives. For some, anxiety also resulted in panic attacks or out of character outbursts of anger ‘he’d get angry and start throwing things around that he could reach’ (participant 15a).
Compounding impact of feeling like a burden
Many patients felt guilty of being a burden to their friends, family and partner. This resulted in them not ‘making space for my own needs’ (participant 22). They felt home dialysis was ‘putting a lot of pressure on other people’ (participant 23a), and they didn’t want to add to this by being an emotional burden. In contrast, the caregivers being interviewed felt upset that their (patient) partner wasn’t being open about their emotions.
Importance of support systems
Impact on relationships
Home dialysis caused tension in relationships. For some caregivers, they resented their partner being on dialysis because they were unable to contribute to parenting or social activities. Dialysis at home also resulted in changed roles within relationships and reduced intimacy ‘he has his own room and I have my own room. Obviously, that’s affected our relationship’ (carer 10b).
Need for emotional support
The importance of having family to ‘share the mental load’ (participant 19) was a key factor in dealing with the psychological impacts of home dialysis. Many described the need for emotional support and to have someone ‘being there’ (participant 8). Some described how discussing their feelings with someone they were already close to was better than seeing a trained professional. ‘I don’t really need to talk to someone external about it. We just deal with it together’ (carer 10b).
Reassurance through shared experiences
Patients found peer support from other people on dialysis who they could relate to, be honest with and reciprocate support. Those who didn’t have peer support discussed how this would have provided them with reassurance and help to normalise their feelings. ‘I would have just loved for somebody in my age group say, that went through the same thing that rang me up and said hey you’re going to be okay’ (participant 6).
Valuing trustworthy and committed clinicians
Many participants felt supported by a trusting relationship with their dialysis nurse or doctor. They could talk openly with them about their emotional and mental health and seek appropriate support when needed. Many appreciated their clinician knowing them so well that they initiated a conversation about the patient’s mental health having deteriorated: ‘With my consultant, he reached out to mental health for me, and I got an acute team to sort me out’ (participant 12).
Burden of distress
Individualised feelings of low mood
Participants openly discussed their struggles with low mood and their experience that feeling low was normal and acceptable. Many described ‘a sliding scale’ (participant 20) of mood, where certain challenges and changes led to a lower mood, while some days were better.
Grappling with stigma surrounding diagnosis
Patients described being on a spectrum of sadness and debated within themselves about whether sadness or ‘down’ days were normal considering the ‘situation’s depressing’ (participant 13a) or whether they were clinically depressed. Some didn’t consider themselves depressed as they hadn’t received a clinical assessment and been given a diagnosis. ‘I don’t think I’ve had depression. But yes, I get depressed, but no, I don’t have depression’ (participant 13a). Others also discussed that their family members considered them depressed and needing antidepressants, but they themselves knew that this would be a passing phase. Others found it difficult that other people didn’t ‘see’ that they were depressed even when they told them.
Contemplating treatment withdrawal and suicide
Several patients discussed that they had seriously contemplating ending their lives. Some had discussed suicidal thoughts openly with their medical team and sought help for this, understanding that they needed immediate help. Others had ‘quite extensive conversations about terminating life, I’ve contacted the end-of-life team, in other words euthanasia team’ (participant 16).
Seeking mental health support
Normalising mental health support as a distinct entity in dialysis care
Participants felt mental health support was not valued the same as physical support. Those who had tried to access mental health support had given up asking as they had ‘tried numerous times.…Absolutely no help whatsoever’ (participant 11). Wait times were perceived as too long, and during this delay, there was no ‘platform where I feel I can voice out my concerns’ (participant 1). They felt frustrated that the system did not ‘work for the patient’ (participant 5), as they then had to tell more than one person that they weren’t coping and ‘it’s really hard to go and tell someone that you’re feeling like you want to kill yourself’ (participant 5).
Overcoming barriers to seeking mental health support
The stigma of seeking counselling or mental health support created challenges, particularly as there was a lack of understanding within their families and communities about depression and anxiety. For some, this meant that they were ‘putting on a happy face’ (participant 10b). For others who were diagnosed with depression, they spoke of how this was not acknowledged or validated by others ‘it’s really hard for people to see that when you don’t present as someone who’s literally on the edge of topping yourself’ (participant 20). For some seeking mental health support made them feel like they were ‘weak’ or ‘crazy’ (participant 19).
Additional tools for mental health support and connection
Telemedicine, information technology or digital apps were seen as potential ways to improve access to mental health support for home patients. Tools such as these would enable contact with health services for ‘a question or a worry or a concern that can be answered. You know just in a quick message would be so, so good’ (participant 11). Others saw potential in being able to report quickly and easily a ‘mood indicator’ (participant 17) so that it helped clinical staff to monitor changes in mood. There was also a perceived benefit in being able to reach out and ‘remain anonymous’ (participant 1).
Discussion
This in-depth interview study with consumers experiencing home-based dialysis identified overwhelming isolation and disconnection arising from dialysis treatment at home. This isolation was exacerbated by feeling abandoned by clinical staff and support systems, which in turn led to escalating and poorly controlled anxiety. Patients felt like a burden and avoided discussing their psychological concerns. Unsupported and unspoken psychological distress further strained their support systems and directly impacted trust within their close relationships.
Conversely, support systems of family and friends were central to emotional support. Patients also received reassurance through connecting with peers with kidney disease, which enabled their experiences to be validated and enabled them to offer reciprocated care. They particularly valued clinicians whom they could trust and who identified their mental health needs spontaneously and routinely. The psychological experiences were sometimes a constant and unrelenting struggle, and also could be variable and changing often, leading patients to doubt whether they had a problem or needed support. The burden of psychological and emotional distress was so severe that many patients contemplated ending their life or withdrawing from treatment. Stigma prevented patients from seeking mental health care, and delivery of psychological care to dialysis patients was poor. Patients wanted mental health care to be routinely provided in dialysis services and also remotely accessible and non-judgemental.
In this study, consumers reported that clinicians who routinely considered the psychological aspects of home dialysis provided consumers with early access to care, identified symptoms promptly, discussed and treated symptoms and provided early referral to additional services. Other studies have also associated strong clinician support with enabling effective management of distress 14 and continuity of care and good clinician communication with enabling smooth transitions between health providers. 15 Similarly, research in cancer care has demonstrated that poor clinician communication was associated with high levels of psychological distress for consumers. 16 Likewise, enhanced and routinely delivered psychosocial support can significantly reduce caregiver burden and anxiety. 17 This emphasises the importance of clinician literacy and effective communication related to psychological well-being, which has been effective in advanced care planning in kidney patients 18 and similarly may have benefits in identifying and supporting consumer mental health for home dialysis.
Our study also identified the stigma of a mental health diagnosis for patients and the challenges this added to seeking and accessing mental health support. To limit the requirement for consumers to access care in the context of stigma and poorly designed services, these consumer-based perspectives indicate that delivering mental health services routinely in home dialysis care is recommended, particularly given the high prevalence of both depression and anxiety in this group of patients. 3 Similar studies of patients and caregivers of those receiving facility dialysis have also identified the huge hidden burden of depressive symptoms and depressive illness in patients with CKD 19 and the lack of support services. 20 Training staff to support patients dialysing at home in psychological care is important, particularly given that patients in our study preferred talking to trusted clinical staff over specialty mental health clinicians who they didn’t know. In a previous study, brief low-intensity psychological therapy delivered in partnership with nurses already involved in the patients’ care, reduced depression. 21
The experiences of patients and caregivers in our study support the implementation and evaluation of routine mental health support for consumers of home dialysis, particularly among those at risk of low adherence, suicidality and withdrawal from care. Given the feelings of isolation and abandonment discussed by participants, increasing nursing support and home contacts may be an important quality improvement for home dialysis care. Other studies in cancer care have identified patients perceive nurses as their primary point of contact for health-related issues and emotional support. 15 Participants in our study identified solutions to increase support and mental health well-being in the form of peer support. Peer support is already identified in research as important in supporting patients on home dialysis. 22 –26 Alternative models of care that support patient well-being on home dialysis include community home dialysis where patients reported positive effects of ‘home’ dialysis in a community environment on their emotional and psychological well-being. 22
The strengths of this study include interviewing a diverse range of consumers at a national level and member checking of transcripts by participants. Participants were offered the opportunity to review both their transcripts and the final interpretation of findings.
A limitation of the study may be the self-identification of participants. Although generalisability is not recognised as a limitation of qualitative studies, it could be postulated that New Zealand might be different from other health jurisdictions in that services, accessibility of psychological support may be more accessible in other countries, and access to mental health services may be different across regional areas and between units. We also only interviewed consumers, and there may be additional benefits to understanding clinician viewpoints on this topic. Our study was conducted over the time of Covid-19 social restrictions, and these may have exacerbated feelings of isolation and loneliness for participants.
In conclusion, consumers may experience intense psychological distress during home-based dialysis care. Increasing clinician and health services literacy about the management of psychological impacts of home-based dialysis may improve consumer safety, quality of life and sustainability of home treatment.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608231202899 - Consumer values, perspectives and experiences of psychological health when living with dialysis at home: An in-depth interview study
Supplemental Material, sj-docx-1-ptd-10.1177_08968608231202899 for Consumer values, perspectives and experiences of psychological health when living with dialysis at home: An in-depth interview study by Rachael C Walker, Curtis Walker, Annie Reynolds, Rachel Haselden, Sandra Hay and Suetonia C Palmer in Peritoneal Dialysis International
Supplemental material
Supplemental Material, sj-docx-2-ptd-10.1177_08968608231202899 - Consumer values, perspectives and experiences of psychological health when living with dialysis at home: An in-depth interview study
Supplemental Material, sj-docx-2-ptd-10.1177_08968608231202899 for Consumer values, perspectives and experiences of psychological health when living with dialysis at home: An in-depth interview study by Rachael C Walker, Curtis Walker, Annie Reynolds, Rachel Haselden, Sandra Hay and Suetonia C Palmer in Peritoneal Dialysis International
Footnotes
Acknowledgements
The authors are sincerely grateful to all patient and caregiver participants; Kidney Health NZ; Auckland Dialysis Kidney Society; and Te Whatu Ora – Canterbury and Hawke’s Bay.
Author contributions
Research idea and study design: RCW, SCP, CW; data acquisition: RCW, SH, RH; data analysis/interpretation: RCW, SCP, CW, SH, RH, AR. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. RCW has previously received funding from Baxter Healthcare, Health Research Council and Lotteries Health New Zealand which do not pose a financial conflict of interest with respect to this work. SCP has received funding from Heath Research Council and Lotteries Health New Zealand, which does not pose a financial conflict of interest with respect to this work. The remaining authors declare that they have no relevant financial interests.
Ethical approval
The study was approved by the Eastern Institute of Technology Research and Ethics Committee (EA08260721).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Lotteries Health Research Fund, New Zealand. The funder had no role in the study design; data collection, analysis and reporting; or decision to submit this manuscript for publication.
Informed consent to participate
All participants provided written informed consent to participate in this study.
Informed consent to publish
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.