
Abstract
Home dialysis (peritoneal dialysis (PD) and home haemodialysis (HHD)) are ideal options for kidney replacement therapy (KRT). Occasionally, because of technique failure, patients are required to transition out of home dialysis, and the most common option tends to be to in-centre HD. There are few published studies on home-to-home transition (PD to HHD or HHD to PD) and dynamics during the transition period. We present a retrospective review of 28 patients who transitioned from a home-to-home dialysis modality at our centre over a 24-year period. We observed a total of 911 home dialysis patients with technique failure (826 PD patients and 85 HHD patients) with only 28 patients (3% of the total with technique failure) having successful home-to-home transition. During the transition period, 11 patients (39%) were hospitalized and 13 patients (46%) required variable periods of in-centre HD. After a median follow-up of 48 months following dialysis modality transition, four patients switched to in-centre HD permanently (home dialysis technique survival of 86% censored for death and kidney transplantation) and four patients died resulting in a patient survival of 86% (censored for switch to in-centre HD and transplantation). In our centre, home-to-home transition is a feasible strategy with comparable patient and technique survival. A significant proportion of patients switching from a home-to-home dialysis modality required variable intervals of hospitalization and in-centre HD during transitions. Future efforts should be directed towards assessment and home dialysis education during the entire process of dialysis transition.
Introduction
The burden of chronic kidney disease is increasing worldwide. 1,2 Home dialysis (peritoneal dialysis (PD) and home haemodialysis (HHD)) are ideal kidney replacement therapy (KRT) options. There is a global drive for a ‘PD first’ model. 3,4 This approach helps to preserve vascular access, minimize cost and may help to preserve residual kidney function. 5 –8 PD technique failure may occur for a variety of reasons, necessitating a switch to hemodialysis. 9,10 Most patients who fail PD or HHD default to in-centre haemodialysis (IHD).
The period of transition between different KRT modalities is challenging and carries risk for morbidity and mortality if not well planned. 11,12 Little has been published about the implementation of a model of transition from a home to a home modality. 13 –16,17 Particular issues such as hospital admissions, the need for in-centre dialysis during transition, training time and vascular access planning are not well-studied and require further research.
In this study, we present 24 years of experience of home-to-home dialysis modality transition in our centre. We hypothesize that home-to-home is not a direct transition and will involve variable periods of in-centre HD during modality change. The objective of this work is to study the dynamics of this period of shift between home modalities and evaluate the need for in-centre HD during transition to optimize future planning of home-to-home transition.
Method
Research Ethics Board and institutional approvals were obtained before initiation of the study (UHN Institutional Approval 19-5163). This is a single-centre retrospective descriptive study including all consecutive patients who switched from PD to HHD or from HHD to PD in the home dialysis units of University Health Network (UHN) during the period of 1 January 1996 to 1 December 2019. All the patients who started training for either PD or HHD then permanently transitioned to the other home modality were included, regardless if they transitioned directly or if they required periods of in-centre HD. Permanent transition was defined as at least 90 days of continuous therapy on the new modality. If patients received kidney transplantation between the first and second home dialysis modality, they were excluded.
Electronic records and paper charts were reviewed to collect baseline data of patient demographics, RRT vintage, sequences of difference KRT modalities and co-morbidities. For the transition period, we analysed the cause of modality failure, periods of intercurrent hospitalization and need for in-centre HD during transition. The outcome measures of the present study were patient and technique survival and rate of hospitalization after starting the second home dialysis modality. Patient survival was censored at the time of loss to follow-up, transplantation, permanent switch to in-centre HD or the end of the follow-up period. Technique failure was defined as a permanent change in dialysis modality.
All data are reported as counts and percentages for categorical variables and median and interquartile ranges for continuous variables.
Results
During the study period, 826 patients had PD technique failure, 24 patients (2.9%) switched to HHD while 802 patients (97.1%) switched to in-centre HD. During the same time period, 85 patients had HHD technique failure, 4 patients (4.7%) switched to PD and 81 patients (95.3%) switched to in-centre HD. The transition did not follow a specific pattern over time. The demographics of the home-to-home transition cohort are shown in Table 1.
Baseline characteristics of patients with home-to-home transition, at time of first home therapy.
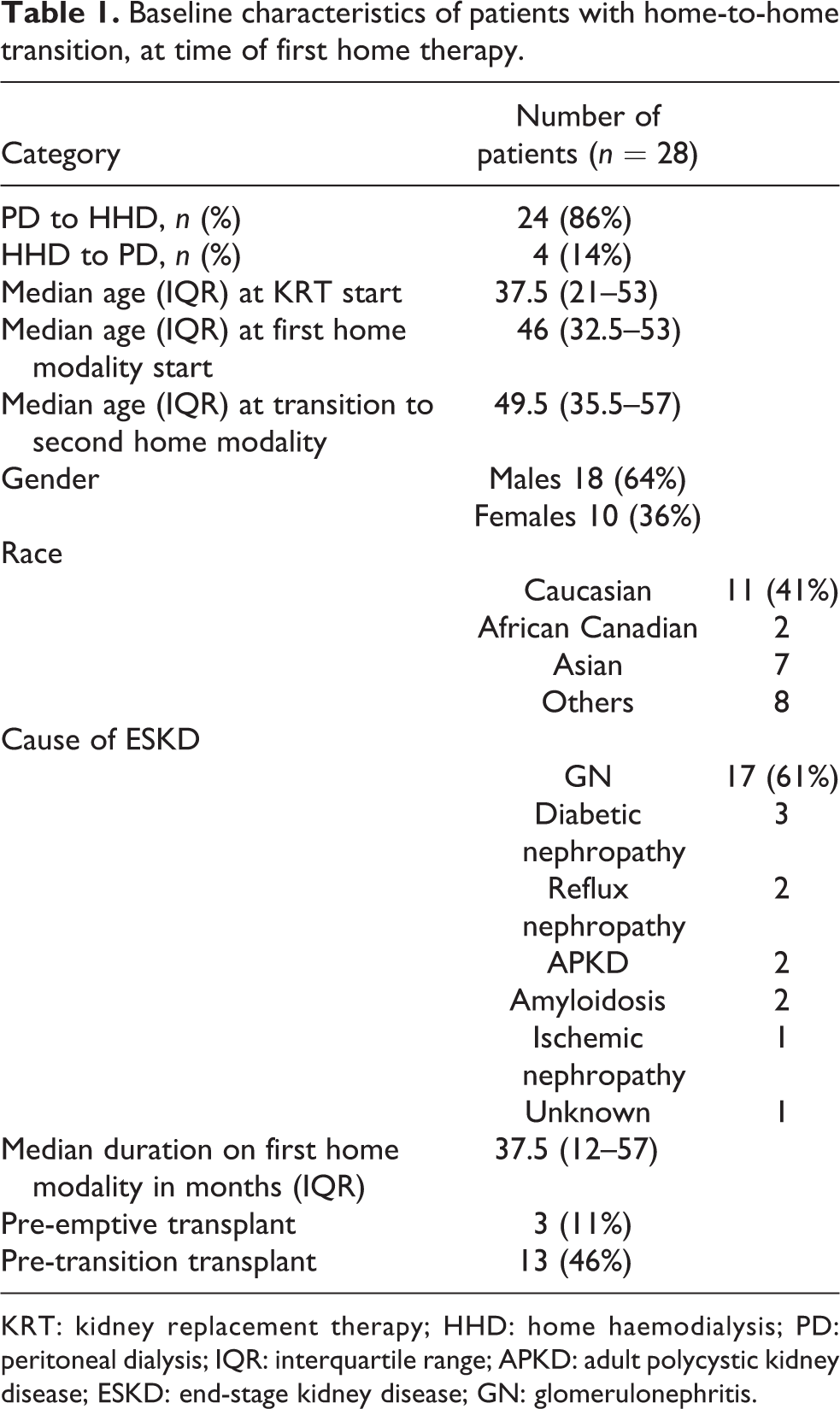
KRT: kidney replacement therapy; HHD: home haemodialysis; PD: peritoneal dialysis; IQR: interquartile range; APKD: adult polycystic kidney disease; ESKD: end-stage kidney disease; GN: glomerulonephritis.
During the transition period, 11 patients (39%) required hospital admission and the median duration of admission was 16.5 days. The causes of hospitalisation included peritonitis (n = 7), ultrafiltration failure (n = 2), mechanical (n= 1) and abdominal surgery (n = 1). A similar number and distribution of patients were noted to require in-centre HD back up; 15 patients (54%) transitioned directly from the first to second home modality while 13 patients (46%) required interim in-centre HD backup. Two of them needed in-centre HD for less than 30 days while 11 patients needed in-centre HD for more than 30 days with a median time of 14 (IQR 6–40) months. The causes of technique failure of the first home dialysis modality and subsequent need for hospitalization and in-centre haemodialysis backup are shown in Table 2.
Causes of technique failure of first dialysis modality and need for subsequent in-centre HD or hospitalization during transition.
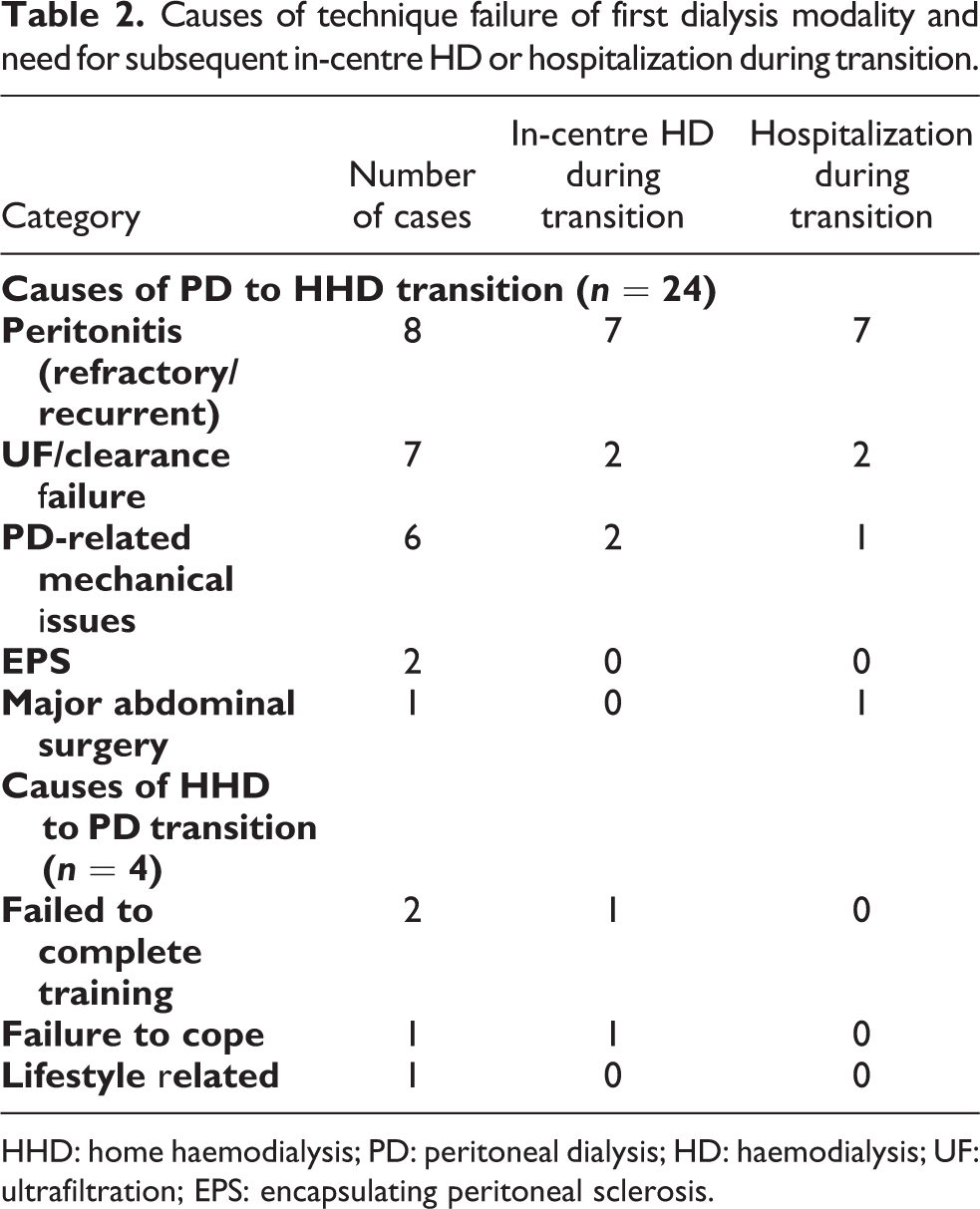
HHD: home haemodialysis; PD: peritoneal dialysis; HD: haemodialysis; UF: ultrafiltration; EPS: encapsulating peritoneal sclerosis.
The median follow-up duration was 48 (24–128) months after transition to the second home dialysis modality. For the PD to HHD group, the mean number of modality training sessions was 29 sessions, receiving an average of 34.3 h of dialysis per week after starting home haemodialysis; 17 patients (71%) started HHD using a tunnelled haemodialysis catheter while 5 patients (21%) had an Arteriovenous fistula and 2 patients (8%) had an AV graft. For the HHD to PD group, the mean number of modality training sessions was 6; all patients had laparoscopic PD catheter insertion. Three patients started on APD and one patient started on CAPD.
At end of follow-up, four patients were permanently transitioned to in-centre HD, due to multiple co-morbidities and failure to cope with home dialysis. Technique survival of the second home modality after home-to-home transition (censored for death and kidney transplantation) was 86%. Patient survival was 86%. Four patients died while on their second home dialysis modality, the cause of death included septic shock (2), cardiogenic shock (1) and respiratory failure (1). Eight patients (29%) had kidney transplantation after home-to-home transition. All of the remaining patients were active on the waiting list for transplantation. During the follow-up period, our cohort had 103 hospitalizations with a rate of 0.74 episode per patient-year.
Discussion
In this descriptive study, we report our centre’s home-to-home dialysis transition experience over a period of 24 years. PD to HHD contributed the majority of cases. Both patient and technique survival were excellent in our cohort. Mean training duration, average hours on dialysis and rate of hospitalization were comparable to other patients in our centre who had been on home dialysis without home-to-home modality transition.
PD to HHD transition has been demonstrated to be a feasible option without any increased risk of patient or technique survival. 17 In a previous registry report, the rate of PD to HHD transition was 2% of PD patients with technique failure, with different centres ranging between 1% and 12% per year. 18 In another report from ANZDATA registry, 5.4% of patients with PD technique failure transitioned to HHD within 180 days of PD cessation. 14 In a retrospective study exploring survival and kidney transplantation difference between HHD and in centre HD after PD technique failure, only 3.8% of the HHD cohort were previously on PD. 19 In our combined cohort, our home-to-home rate was 3% of all home dialysis technique failures which represents a low rate of transition. The reason for this low transition rate is not clear. One barrier for offering direct home-to-home transition is that these patients often develop significant comorbidities or complications after the first home dialysis modality technique failure, which usually necessitates transition to in-centre HD. Their intercurrent illness often results in frailty which may represent a barrier to learn a new home dialysis modality and could explain a missed opportunity for transition. In our cohort, 39% of patients needed hospitalization during their transition and 46% needed in-centre HD for variable durations before starting their second home modality. Our present observation highlights the opportunity for ongoing home dialysis education after the initial period of illness or hospitalization especially during the variable periods of in-centre HD. Potential home to home transition patients should be identified and evaluated periodically during in-centre HD rounds. Ongoing support and home dialysis evaluation and education should be done proactively with an emphasis on ‘home dialysis first’ philosophy.
In summary, home-to-home dialysis transition is feasible and successful with comparable patient and technique survival. Close to half of our cohort required a period of hospitalization and in-centre HD during their transition. We recognize that our study is limited by its observational, retrospective, single-centre design. Future efforts should be made towards offering and supporting the switch to a second home modality during the period of in-centre HD while promoting the notion of an integrated home dialysis system.
Footnotes
Author contributions
My co-authors and I have all contributed to this manuscript and approve of this submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr CT Chan has consulted for Medtronic, Quanta and DaVita Inc. Dr JM Bargman has consulted for or been a member of the Speakers’ Bureau for DaVita Healthcare Partners, Baxter Global, Baxter Canada, GSK and Novartis.
Ethical approval
Institutional research ethics approval was obtained.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.