
Abstract
Background:
In Europe, the number of elderly end-stage kidney disease patients is increasing. Few of those patients receive peritoneal dialysis (PD), as many cannot perform PD autonomously. Assisted PD programmes are available in most European countries, but the percentage of patients receiving assisted PD varies considerably. Hence, we assessed which factors are associated with the availability of an assisted PD programme at a centre level and whether the availability of this programme is associated with proportion of home dialysis patients.
Methods:
An online survey was sent to healthcare professionals of European nephrology units. After selecting one respondent per centre, the associations were explored by χ 2 tests and (ordinal) logistic regression.
Results:
In total, 609 respondents completed the survey. Subsequently, 288 respondents from individual centres were identified; 58% worked in a centre with an assisted PD programme. Factors associated with availability of an assisted PD programme were Western European and Scandinavian countries (OR: 5.73; 95% CI: 3.07–10.68), non-academic centres (OR: 2.01; 95% CI: 1.09–3.72) and centres with a dedicated team for education (OR: 2.87; 95% CI: 1.35–6.11). Most Eastern & Central European respondents reported that the proportion of incident and prevalent home dialysis patients was <10% (72% and 63%), while 27% of Scandinavian respondents reported a proportion of >30% for both incident and prevalent home dialysis patients. Availability of an assisted PD programme was associated with a higher incidence (cumulative OR: 1.91; 95% CI: 1.21–3.01) and prevalence (cumulative OR: 2.81; 95% CI: 1.76–4.47) of patients on home dialysis.
Conclusions:
Assisted PD was more commonly offered among non-academic centres with a dedicated team for education across Europe, especially among Western European and Scandinavian countries where higher incidence and prevalence of home dialysis patients was reported.
Introduction
Since 2001, the number of end-stage kidney disease (ESKD) patients worldwide treated with dialysis has increased from 1 to 2 million and is expected to double again by 2030. 1 –3 The majority of these patients are treated with in-centre haemodialysis (ICHD), 4,5 although treatment with peritoneal dialysis (PD) has many advantages: it can be performed at home, there is no need for a vascular access and patients’ residual kidney function is better preserved. 6,7 These advantages are especially relevant for the increasing number of elderly patients, who form the bulk of ESKD patients. 8,9 However, the percentage of elderly ESKD patients receiving PD is low and varies between 4% and 21% depending on the country. 4,5,8,10,11
If given a choice, many more elderly would like to receive PD, but comorbidity and frailty often limit the possibility to perform self-care PD. 9,12,13 Important conditions that limit self-care PD include decreased strength to lift PD bags, decreased dexterity, decreased vision, anxiety and cognitive impairment. 12,14 Due to these conditions, up to 80% of elderly patients need some degree of assistance while performing PD. 15 –18
The definition of assisted PD varies in literature. 19 In the most liberal way, it is defined as ‘a PD modality performed at the patient’s home with the help of a healthcare technician, a community nurse, a family member, or a partner’. 20 Patients on assisted PD have similar rates of all-cause hospitalisation compared to ICHD patients, and similar or even better rates of peritonitis and technique survival compared to self-care PD patients. 15,21 –23 Assisted PD patients have higher mortality rates compared to self-care PD patients, which can be attributed to a higher comorbidity and frailty. 15,22 However, health-related quality of life is comparable 24 –27 and assisted PD is less expensive than ICHD in most countries depending on reimbursement strategy. 28,29 Furthermore, introduction of assisted PD has been shown to have a positive effect on maintaining the size of a PD programme, 30 which can be important to ensure experience and quality of care.
Assisted PD programmes are available in many countries, but the percentage of patients actually receiving assisted PD varies considerably. 6,11,19,31,32 This variation may be due to differences in clinical background and experience of healthcare professionals, centre characteristics, organisational and financial factors, as shown in studies regarding PD in general. 6,33 –37 However, this has not been specifically investigated for assisted PD so far.
Therefore, we first assessed the factors that are associated with the availability of an assisted PD programme at a centre level, to get insight into the causes of practice variation. Secondly, we investigated the association between the availability of an assisted PD programme and the proportion of incident and prevalent patients on home dialysis (i.e. PD and home haemodialysis (HHD)) at a centre level, to get insight into the influence of availability of assisted PD on the uptake of home dialysis.
Methods
Study design
An online survey was sent to nephrologists (in training), dialysis nurses and administrative heads of nephrology units in Europe. The survey was developed by members of the EuroPD Future Leadership Initiative after two conference meetings in May–June 2019. The members discussed how the care for ESKD patients could be improved by helping nephrology departments with their home dialysis programmes. The following topics were discussed: PD training, urgent start PD, age-related differences in use of PD, remote patient monitoring, organisation of nephrology units, centre size effect and regional collaboration between centres. Subsequently, four topics (impact of urgent start PD, impact of assisted care programmes, impact of access placement policy and impact of centre size) were selected through a three-step Delphi round. 38 During a final meeting in October 2019, questions were formulated for each topic after conducting a narrative literature review. The final survey consisted of 56 questions (Appendix 1).
The open survey was developed in SurveyMonkey and mailed to all EuroPD members for distribution across Europe via their colleagues and their national and regional nephrology societies. Participation was voluntary and anonymous. Respondents could submit the survey between 11 December 2019 and 15 January 2020. The survey was approved by the Ethical Committee of the Ghent University Hospital (EC 2019/1972).
Statistical analysis
Descriptive statistics were used for the professional background, centre type and country of employment of all respondents. The countries were classified into European regions: Eastern & Central Europe, Western Europe, Scandinavia and the Mediterranean. 39 Ukraine and the Russian Federation were added to the Eastern & Central European region.
Generally, the policy regarding the availability of an assisted PD programme is determined at a centre level. To perform analyses at a centre level, one respondent per centre was selected by comparing respondents based on the following characteristics: country, region, centre type and size, and the proportion of incident and prevalent ESKD patients on a home-based therapy. If there were several respondents per centre, the respondent with the largest experience was chosen for the analyses.
For the analysis of the availability of an assisted PD programme at a centre level, the answers to the question ‘Does your unit provide a structured programme for assisted PD?’ were converted from a 5-point Likert scale into a dichotomous variable (scores 1 to 3: no, scores 4 and 5: yes). In addition, answers regarding the following variables were grouped into categories: centre type (non-academic vs academic), likelihood that chronic kidney disease (CKD) patients would receive education on kidney function/kidney failure/PD/HHD/ICHD (6-point Likert scale converted into a dichotomous variable), reimbursement of PD as compared to ICHD (8 categories converted into 4) and the proportion of incident and prevalent home dialysis patients (<10%, 10–20%, 20–30%, >30%).
The univariable association between employment regions, centre characteristics and organisational factors (independent variables) on the one hand and the availability of an assisted PD programme at a centre level (dependent variable) on the other hand was explored by logistic regression. For categorical variables, the first category was used as a reference. In addition, a multivariable analysis was done to explore which variables were truly independent.
Subsequently, descriptive statistics were used to present an overview of financial factors: the profitability of PD (i.e. difference between reimbursement and disposable costs) and the impact of the distribution between kidney replacement (KRT) modalities (i.e. PD, HHD, ICHD, kidney transplantation) on the income of nephrologists for centres with and without an assisted PD programme. The univariable association between profitability of PD and the impact of the distribution between KRT modalities on nephrologists’ income (independent variables) on the one hand and the availability of an assisted PD programme at a centre level (dependent variable) on the other hand was also explored by logistic regression.
Finally, the univariable association between the availability of an assisted PD programme (independent variable) and the proportion of incident and prevalent home dialysis patients (defined as both PD and HHD) at a centre level (dependent variable) was analysed by a χ 2 test. In addition, ordinal logistic regression (logistic regression with proportion of incident and prevalent home dialysis patients as outcome) was performed to adjust for centre type, centre size (i.e. total number of dialysis patients), the presence of a dedicated team for education and European region (multivariable association). The five categories of the variable ‘presence of a dedicated team for education’ were transformed into a dichotomous variable. Answers ‘no’ and ‘do not know’ were indicated as ‘no’, while ‘yes, less than 1 fulltime equivalent’, ‘yes, 1 fulltime equivalent’ and ‘yes, 2 or more full time equivalents’ were indicated as ‘yes’. Ordinal logistic regression gives a cumulative odds ratio (OR) that indicates the probability of being in a higher category compared to the previous category.
All statistical analyses were performed with SPSS Statistics version 25 (SPPS, Chicago, Illinois, USA).
Results
Characteristics of respondents
In total, 609 respondents completed the online survey. Fifty-three percent of the respondents were nephrologists with more than 10 years of experience (Online Supplemental Table S1). Forty-nine percent of the respondents worked in a non-academic centre and half of the respondents worked in Western Europe (Online Supplemental Tables S1 and S2).
After completing the aforementioned selection procedure, 295 respondents from individual centres were identified (Online Supplemental Tables S1 and S2). Data on the availability of an assisted PD programme were missing in seven respondents, thus the following analyses were conducted with 288 respondents.
Centre characteristics and organisational factors associated with the availability of an assisted PD programme
Of the 288 respondents, 167 (58%) worked in a centre with an assisted PD programme. The association between employment regions, centre characteristics and organisational factors on the one hand and the availability of an assisted PD programme on the other hand is presented in Table 1. Compared to the Eastern & Central European region, respondents from Western Europe and Scandinavia indicated significantly more often that an assisted PD programme was available (Table 1). Compared to the Eastern & Central European and Mediterranean regions combined, respondents from Western European and Scandinavian regions combined also indicated significantly more often that an assisted PD programme was available (crude OR: 7.11; 95% CI: 4.91–10.29).
Association between employment regions, centre characteristics and organisational factors with the availability of an assisted PD programme.a
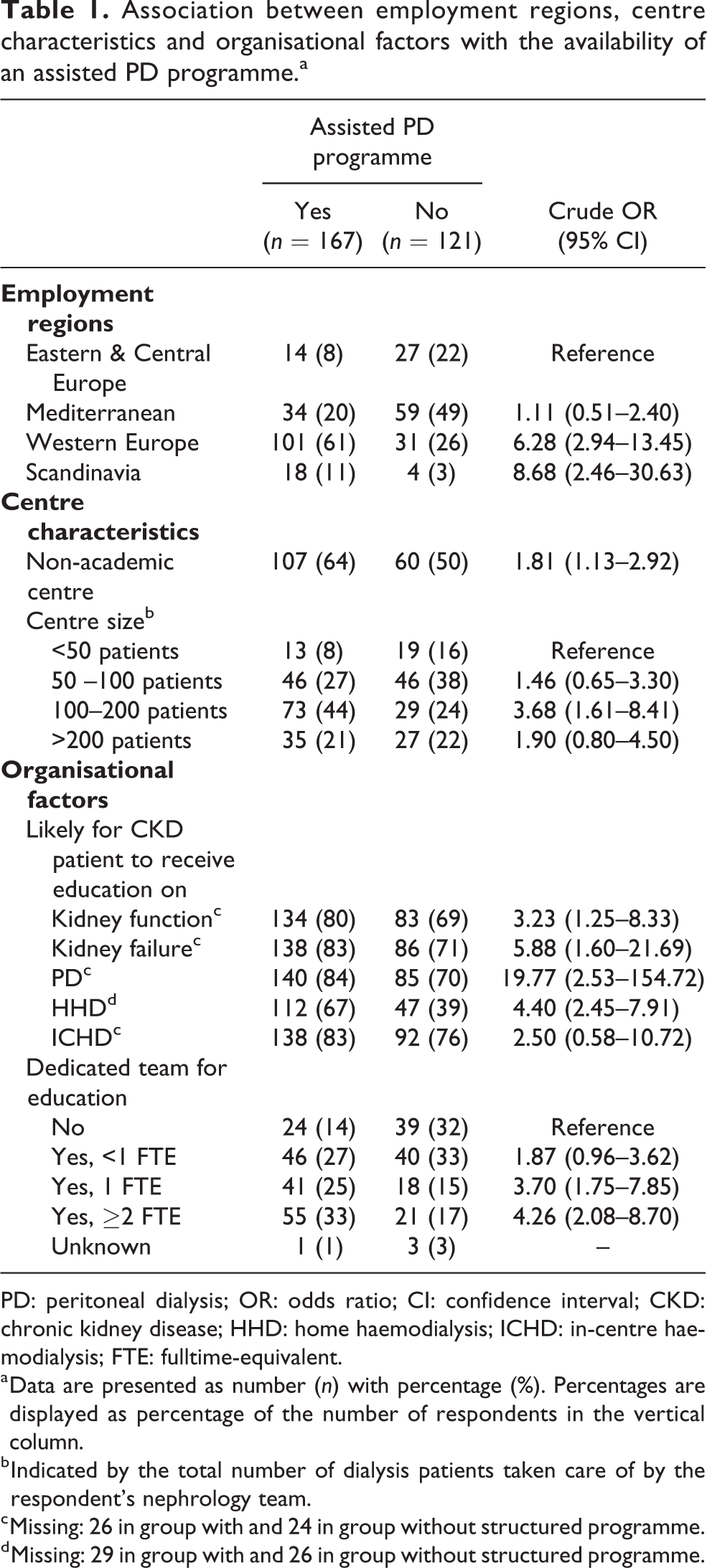
PD: peritoneal dialysis; OR: odds ratio; CI: confidence interval; CKD: chronic kidney disease; HHD: home haemodialysis; ICHD: in-centre haemodialysis; FTE: fulltime-equivalent.
a Data are presented as number (n) with percentage (%). Percentages are displayed as percentage of the number of respondents in the vertical column.
b Indicated by the total number of dialysis patients taken care of by the respondent’s nephrology team.
c Missing: 26 in group with and 24 in group without structured programme.
d Missing: 29 in group with and 26 in group without structured programme.
Regarding centre characteristics, non-academic centres and centres with 100–200 dialysis patients significantly more often had an assisted PD programme (Table 1). Compared to centres with <100 patients (i.e. centres with <50 and 50–100 patients combined), centres with >100 dialysis patients (i.e. centres with 100–200 and >200 patients combined) also significantly more often had an assisted PD programme (crude OR: 2.13; 95% CI: 1.32–3.43).
Regarding organisational factors, centres that provided education to CKD patients on kidney function, kidney failure, PD and HHD significantly more often had an assisted PD programme (Table 1). Education to CKD patients on PD had the strongest association with an OR of 19.77 (95% CI: 2.53–154.72). Also, centres with a dedicated team for education significantly more often had an assisted PD programme, with an increasing OR if more fulltime-equivalent was available.
In the multivariable analysis, only centre size was no longer an independent predictor for the presence of an assisted PD programme (OR: 1.44; 95% CI: 0.78–2.67), while Western European and Scandinavian regions (OR: 5.73; 95% CI: 3.07–10.68), non-academic centres (OR: 2.01; 95% CI: 1.09–3.72), education on PD (OR: 9.04; 95% CI: 1.07–76.18) and a dedicated team for education (OR: 2.87; 95% CI: 1.35–6.11) remained independent predictors.
Financial factors associated with the availability of an assisted PD programme
The association between profitability of PD and the impact of the distribution between KRT modalities on nephrologists’ income on the one hand and the availability of an assisted PD programme on the other hand is presented in Table 2. Thirty percent of all respondents indicated that they did not know what the profitability of PD was in their centre. In addition, there was no association between profitability of PD and the availability of an assisted PD programme.
Association between financial factors and the availability of an assisted PD programme.a
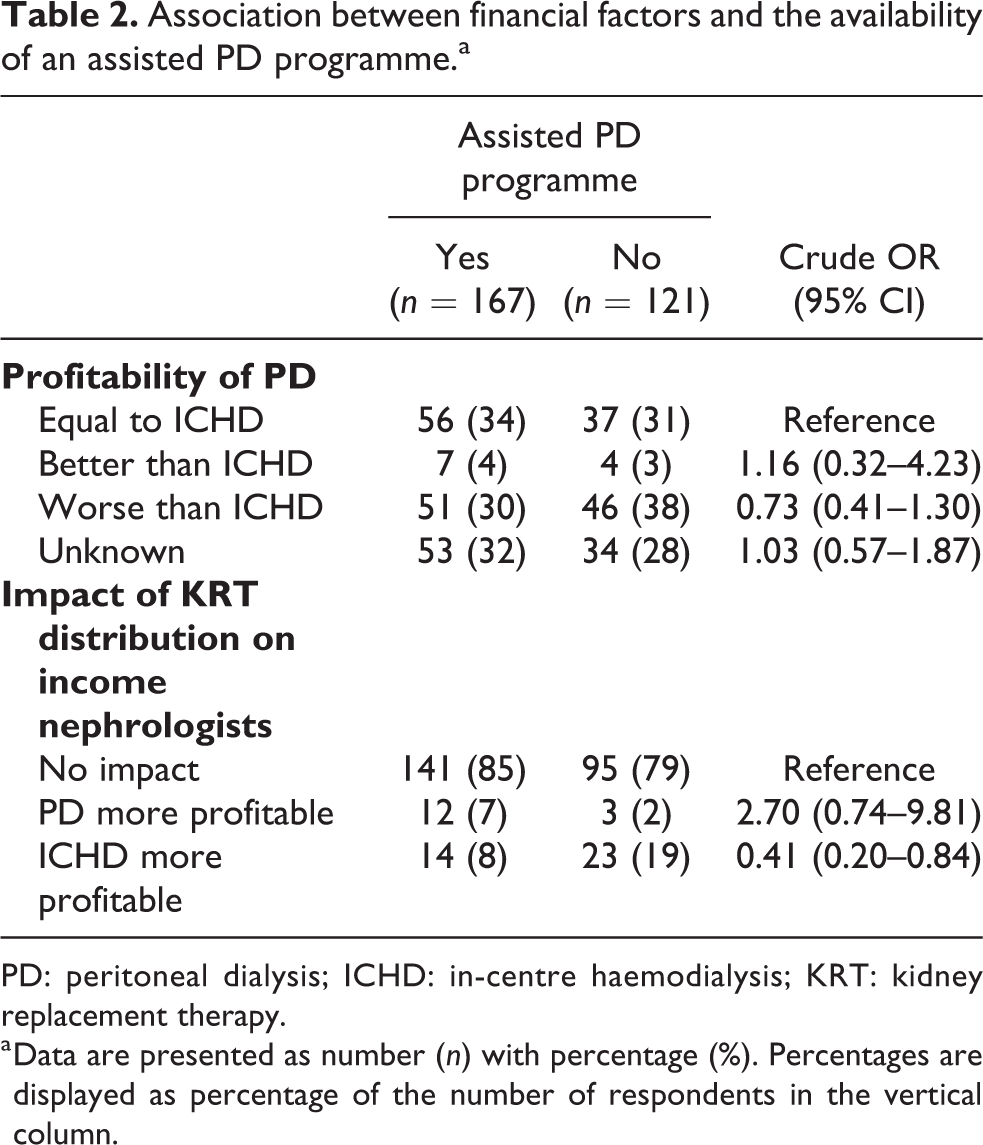
PD: peritoneal dialysis; ICHD: in-centre haemodialysis; KRT: kidney replacement therapy.
a Data are presented as number (n) with percentage (%). Percentages are displayed as percentage of the number of respondents in the vertical column.
Regarding the distribution between KRT modalities, 82% of all respondents indicated that it did not affect the income of nephrologists. Respondents from centres with an assisted PD programme reported this slightly more often than respondents from centres without such a programme, 85% versus 79%, respectively. In centres where ICHD is more profitable, an assisted PD programme was less often available compared to centres where the distribution between KRT modalities has no impact on income (OR: 0.41; 95% CI: 0.20–0.84).
Proportion of ESKD patients on a home dialysis modality
The proportion of incident ESKD patients on a home dialysis modality is depicted in Figure 1. Of all respondents, 39% indicated that the incidence in their centre was <10%, while only 11% indicated that the incidence was >30%. When focusing on the incidence according to region, a much higher percentage (72%) of respondents from Eastern & Central Europe indicated that the incidence in their centre was <10%, while only 9% indicated that the incidence was >30%. For Scandinavia, an incidence >30% was indicated by 27% of respondents.
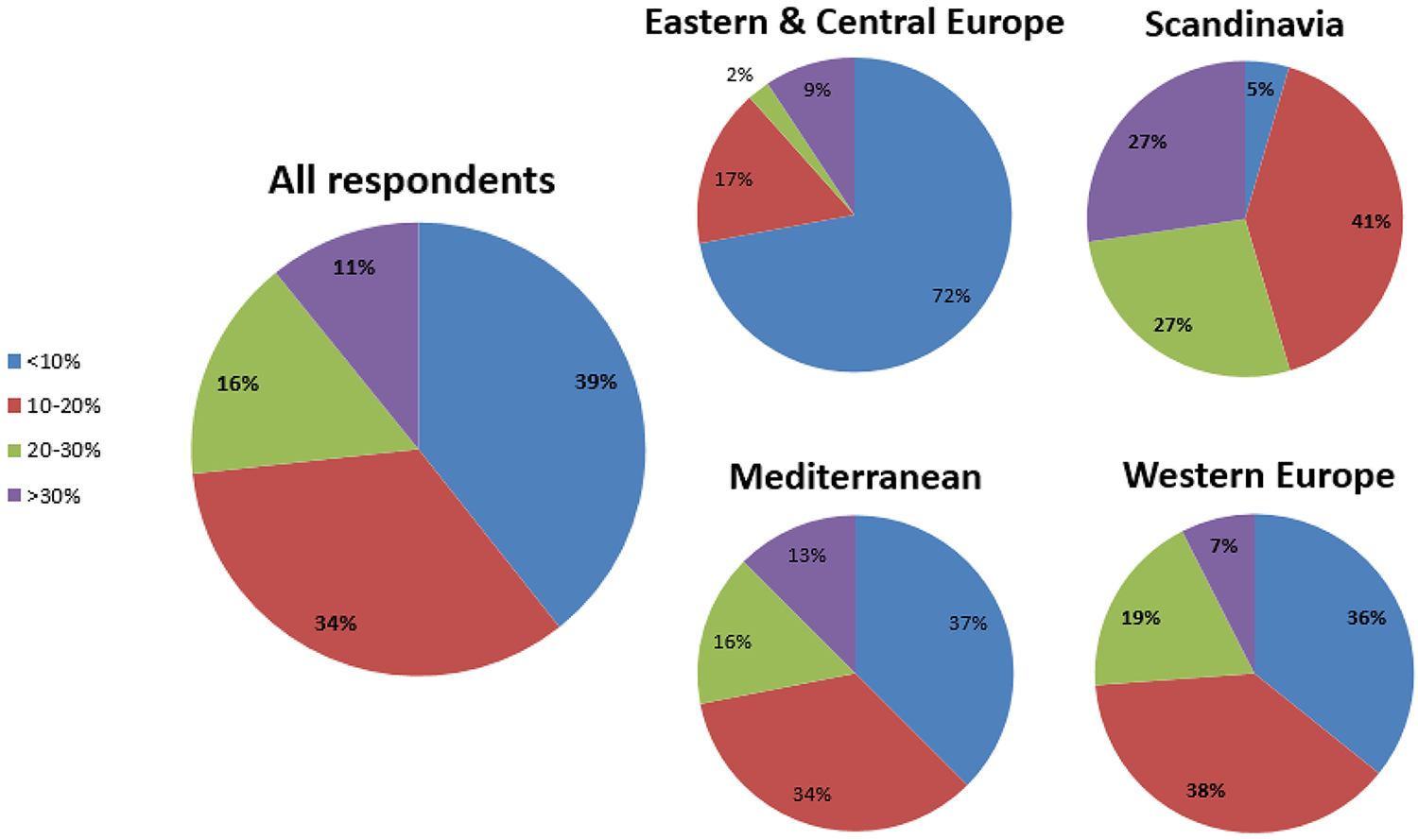
Proportion of incident ESKD patients on home dialysis according to region.
The proportion of prevalent ESKD patients on a home dialysis modality is depicted in Figure 2. Of all respondents, 31% indicated that the prevalence was <10% and 12% indicated that the prevalence was >30%. When focusing on the regions, a much higher percentage (63%) of respondents from Eastern & Central Europe indicated that the prevalence was <10%, while only 14% indicated that the prevalence was >30%. Again, Scandinavia had the highest percentage (27%) of respondents indicating that the prevalence was >30%.
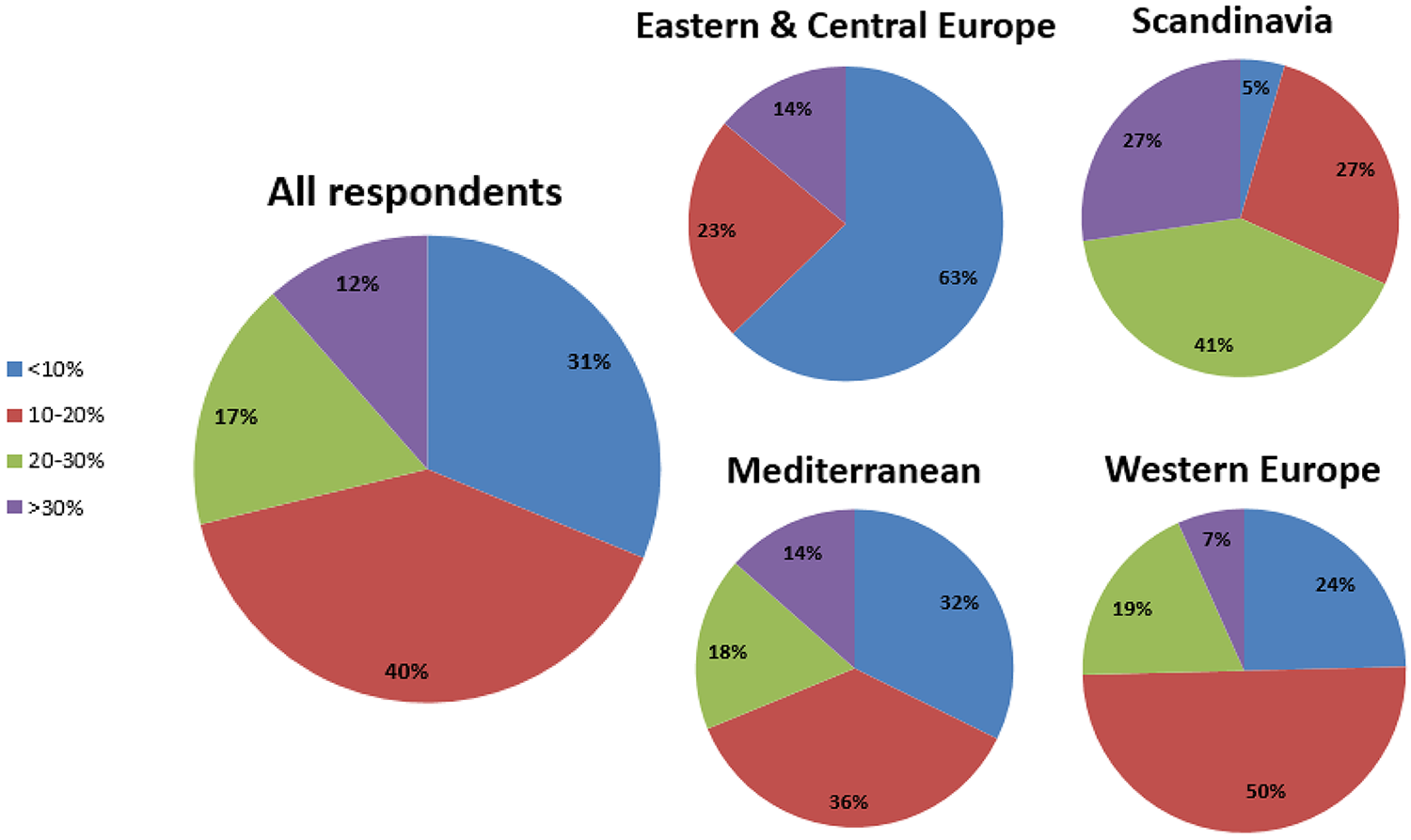
Proportion of prevalent ESKD patients on home dialysis according to region.
Association between the availability of an assisted PD programme and proportion of home dialysis
The proportions of incident and prevalent patients on a home dialysis modality, according to the availability of an assisted PD programme, are depicted in Figure 3. A χ 2 test of independence showed a significant association between the availability of an assisted PD programme and an increasing proportion of incident as well as prevalent ESKD patients on a home dialysis modality (p ≤ 0.001). This association persisted in an ordinal logistic regression analysis, taking into account centre type, size, presence of a dedicated team for education and European region. With this analysis, the cumulative OR for the association between the availability of an assisted PD programme and proportion of incident ESKD patients on a home dialysis modality was 2.22 (95% CI: 1.38–3.57). The cumulative OR for the association between the availability of an assisted PD programme and proportion of prevalent ESKD patients was 3.29 (95% CI: 2.03–5.33).
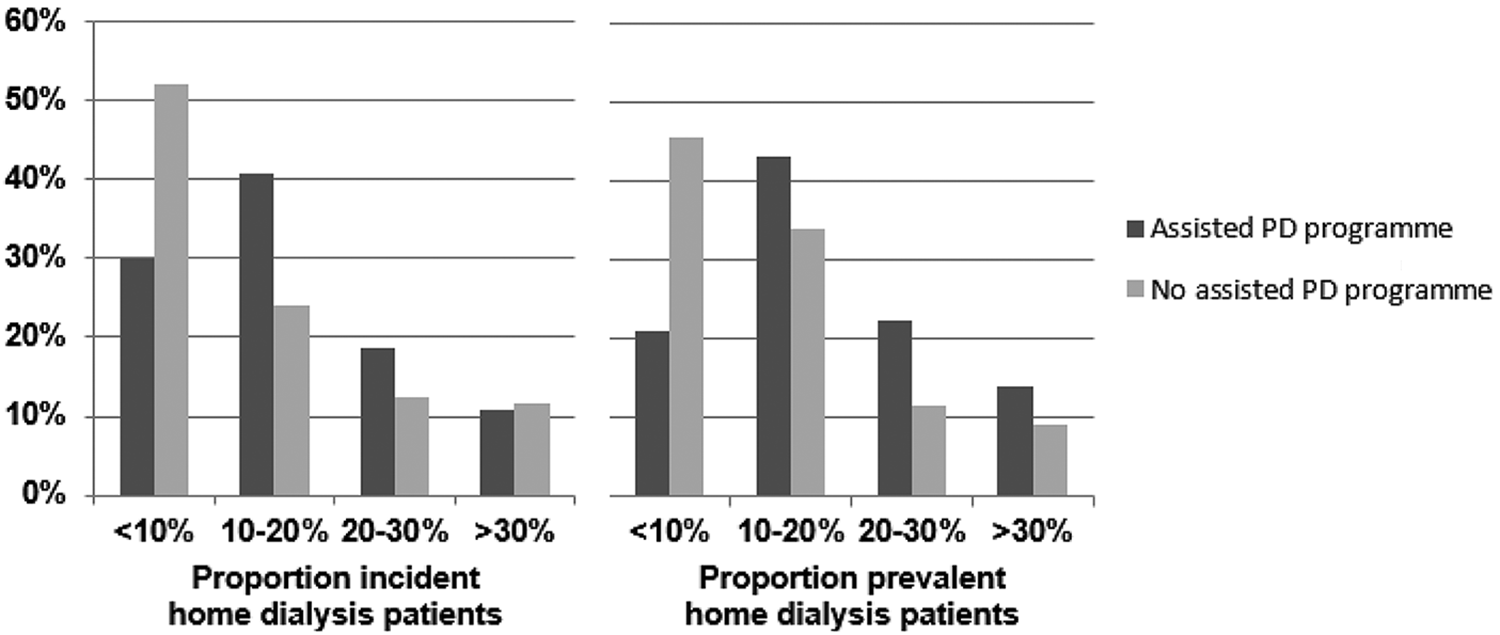
Availability of an assisted PD programme and proportion of patients on a home dialysis modality.
Discussion
Our study among healthcare professionals from European nephrological units shows that assisted PD programmes are significantly more often available in Western Europe and Scandinavia. In addition, we show that assisted PD programmes are more often available in non-academic centres and centres with a dedicated team for education. Also, there seems to be a relationship with reimbursement strategy and impact on the nephrologist’s income since a larger proportion of respondents without an assisted PD programme indicated that ICHD is more profitable. Finally, having an assisted PD programme is associated with a higher incidence and prevalence of patients on a home dialysis modality.
This is the first study to investigate variations in centre characteristics, organisational and financial factors, and their effect on the availability of an assisted PD programme across Europe. Only one previous study has investigated the effect of variations in some of the abovementioned factors, but this was a study on home dialysis in general (i.e. PD and haemodialysis combined) conducted in a single country. This study consisted of a survey among 286 German nephrologists and concluded that centres with assisted home dialysis had more experienced physicians and more prevalent dialysis patients. 40
Although we cannot prove causal relationships, our study can provide guidance on what is needed to treat more patients with assisted PD. While a factor such as centre type cannot be influenced, the positive effect of organisational factors, as a reflection of dedication, seems to be relevant. Indeed, lack of staff, expertise, motivation and patient education are reported barriers that play a role in the uptake of PD. 36,40 –43 A Chinese–German study stated that ‘a timely pre-dialysis education, implementation of a structured model for care, education and training of helping staff, and constantly monitoring of quality parameters is necessary’ to promote assisted PD. 44 So, to treat more patients with assisted PD in Europe, it seems appropriate to invest in a dedicated team of healthcare professionals who provide adequate education and support patients on assisted PD.
Our study also suggests that reimbursement might play a role in the uptake of assisted PD programmes. Numerous European studies have indicated that low reimbursement for PD is an important barrier for PD utilisation, 36,40,41 although assisted PD has shown to be a cost-effective treatment for frail elderly patients. 31 The fact that appropriate reimbursement, besides experience with PD, influences the number of patients on assisted PD is illustrated by a study comparing the assisted PD experiences of Canada and the United States. 11 In Canada, physicians have sufficient experience with PD, reimbursement is equal for PD and ICHD and assisted PD programmes are available, while in the United States, experience with PD is limited, reimbursement for PD is less than for ICHD and assisted PD programmes are not available. As a result, the percentage of incident patients older than 65 years who receive PD is 21% in Canada, while this is only 7% in the United States. 11 Also, two French studies showed that the implementation of assisted PD at a single centre increased the use of PD in incident patients from 21% to more than 40% 45 and that availability of assisted PD was associated with an 1.78 times increased rate of PD initiation, with elderly patients benefitting most. 30
Our study has some limitations. First, there may have been self-selection bias, as healthcare professionals with an assisted PD programme could have been more likely to respond to the survey. However, still centres without an assisted PD programme were relatively well represented in our study. Second, there may have been a recall bias, for example regarding PD profitability. Thirty percent of the respondents in our study did not know what the profitability of PD was in their centre, while 32% indicated that the profitability of PD was equal to ICHD, which probably obscures underappreciated differences; indeed, health economics are complex and likely to be poorly understood. Third, the dichotomisation and categorisation of the response options may also have led to bias. Finally, no analysis could be performed regarding the individuals who facilitated assisted PD, caregivers or family members for example, which could have influenced reimbursement. In addition, reimbursement may also be influenced by geographic location; however, we were unable to perform that analysis due to a limited number of respondents per country. However, this is the first study providing valuable information on practice variation and factors associated with the availability of an assisted PD programme across Europe.
In conclusion, assisted PD programmes are significantly more often available in Western Europe and Scandinavia, in non-academic centres and centres with a dedicated team for education. Importantly, assisted PD programmes are associated with a higher incidence and prevalence of patients on home dialysis. Further research should focus more on (the differences in) reimbursement policies for assisted PD per country.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211049882 - Assisted peritoneal dialysis across Europe: Practice variation and factors associated with availability
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211049882 for Assisted peritoneal dialysis across Europe: Practice variation and factors associated with availability by Anita van Eck van der Sluijs, Brigit C van Jaarsveld, Jennifer Allen, Karmela Altabas, Clémence Béchade, Anna A Bonenkamp, Felix Burkhalter, Anne-Lorraine Clause, Richard W Corbett, Friedo W Dekker, Gabriele Eden, Karlien François, Helga Gudmundsdottir, Ulrika Hahn Lundström, Louis de Laforcade, Mark Lambie, Heike Martin, Jernej Pajek, Vincenzo Panuccio, Silvia Ros-Ruiz, Dominik Steubl, Almudena Vega, Ewa Wojtaszek, Simon J Davies, Wim Van Biesen and Alferso C Abrahams in Peritoneal Dialysis International
Footnotes
Author notes
JA, KA, CB, FB, A-LC, RWC, GE, KF, HG, UHL, LL, ML, HM, JP, VP, SR-R, DS, AV, EW, SJD, WVB and ACA are members of the EuroPD Future Leadership Initiative.
Acknowledgements
The authors would like to thank all healthcare professionals from nephrological units across Europe who completed the survey.
Author contributions
JA, KA, CB, FB, A-LC, RWC, GE, KF, HG, UHL, LL, ML, HM, JP, VP, SR-R, DS, AV, EW, SJD, WVB and ACA developed and distributed the survey; WVB collected the data; AES, AAB, BCJ, FWD and ACA analysed and interpreted the data; AES, BCJ, SJD, WVB and ACA wrote the first version of the paper and revised the paper; all authors critically edited the manuscript and approved the final version.
Declaration of conflicting interests
AES has received speaker honoraria from Baxter Healthcare. WVB has received travel funding and speaker honoraria from Fresenius Medical Care and Baxter Healthcare at several occasions. He is the vice president of EuroPD, which is sponsored by Baxter Healthcare and Fresenius Medical Care. ACA has received speaker honoraria from Fresenius Medical Care and Baxter Healthcare. All other authors declare to have no conflicts of interest. The results in this article have not been published previously in whole or part.
Ethical approval
Ethical Committee of the Ghent University Hospital (EC 2019/1972).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Informed consent to participate
Not applicable
Informed consent to publish
Not applicable
Trial registration
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.