
Abstract
Based on my 7 months of ethnographic research with “flying” or mobile female sex workers (FSWs) in the eastern metropolitan city of Kolkata, India, I argue that the human immunodeficiency virus (HIV) prevention programs have a limited outreach and impact within the community because of the fundamental differences in how the nongovernmental organizations (NGOs) staff and flying FSWs perceive the risk of HIV. This article examines flying FSWs perceptions of HIV risk and the NGOs sexual health outreach services. Further, the implications for HIV prevention programs and social work practice are discussed.
Background and Literature Review
Sex work in India occurs in diverse settings, such as brothels, nonbrothel-based settings, and the traditional Devadasi 1 form of sex work. However, most risk-related research remains primarily focused on visible groups within the sex worker population such as brothel-based female sex workers (FSWs; Pardasani, 2005) and the traditional Devadasi form of sex work (widely prevalent in the southern part of India; Blanchard et al., 2005; Orchard, 2007). In addition, while studies report substantial differences in the sex work environments, sociodemographic characteristics, and risk behaviors among diverse groups of sex workers in India (Blanchard et al., 2005; Dandona et al., 2005), the differences in the human immunodeficiency virus (HIV) vulnerability among different types of sex workers related to specific features of their working situations (contexts, routines, and health-seeking practices) remain yet to be explored (Buzdugan, Halli, & Cowan, 2009; Vanwesenbeeck, 2001).
Recent epidemiological studies report mobile or nonbrothel-based FSWs in India to be a group with a high risk of HIV infection, as they report high rates of inconsistent use of condoms with clients or regular partners (Dandona et al., 2005; Halli et al., 2010; Saggurti et al., 2012). Studies have attributed the presence of both intimate-partner violence and client-initiated violence to restrict mobile FSWs ability to negotiate the use of condoms with their clients or intimate partners (Go, Srikrishnan, Parker, et al., 2011; Panchanadeswaran et al., 2008; Ramesh, Ganju, Mahapatra, Mishra, & Saggurti, 2012; Swain, Niranjan, Battala, Verma, & Jain, 2011), heightening their risk of HIV infection. While the issue of violence and inconsistent use of condoms applies to all subgroups of sex workers, the implications for mobile FSWs differ significantly, especially from the point of view of HIV prevention. Unlike women residing in brothels, who operate from a fixed location, enjoy the support of the sex worker collective groups to enforce safer sexual practices, and for whom it is relatively easier to access the HIV prevention programs instituted within their community, the flying FSWs have no fixed place and time of operation and are hesitant to seek membership in support groups or access health services provided through nongovernmental organizations (NGOs) targeted sexual health outreach services as they fear being identified as a sex worker. Instead, the mobile FSWs solicit their clients from varied public places, such as cinema halls, parks, bus stands, railway stations, hotels/lodges, streets, and highways and choose to operate clandestinely by remaining hidden from the public view. Mobility is maintained by them in order to escape the permanent stigma that arises from residing in brothels and maintaining secrecy about their sex work. Scholars have argued that mobile FSWs are more likely to be infected with HIV than brothel-based FSWs, as they are more prone to experiencing sexual exploitation and abuse as a result of their clandestine operations, limited social support, and lack of access to HIV preventive equipment in their frequently changing work environments (Dandona et al., 2005; Ramesh et al., 2012).
Extant scholars have examined several individual, sociocultural, and structural–environmental factors to restrict women’s ability to negotiate the use of condoms with their regular partners, increasing their vulnerability to HIV infection (Bhattacharya, 2004; Gupta & Weiss, 1993; Parker, Easton, & Klein, 2000). For instance, research conducted with 6,648 sex workers in Andhra Pradesh, India, found women’s inconsistent or nonuse of condoms to be associated with low income. They also found low social support, lack of knowledge that HIV can be prevented, family unawareness of sex work, nonparticipation in FSWs’ support groups, and lack of access to condoms as individual factors responsible for women’s increased risk of HIV infection (Dandona et al., 2005). Other researchers have found illiteracy among FSWs to be significantly associated with lower income per client and a greater prevalence of client-initiated violence or police harassment (Blanchard et al., 2005), suggesting that poor literacy skills among women lead to low self-esteem and hinder their ability to negotiate the use of condoms with clients or partners. Another body of research suggests sociocultural norms of gender and sexuality to restrict women’s ability to engage in risk protective behaviors. A study conducted among men and women in the slums of Chennai, India, revealed that while gender norms related to sexuality sanctioned extramarital affairs for men, women were required to be submissive and passive about their sexuality and bodies. Men perceived women’s initiating or negotiating the use of condoms as a sign of infidelity and insubordination. These cultural norms related to sexuality were reported as a major hurdle by women who, despite suspecting the HIV status of their partner was positive, were unable to negotiate the use of condoms with their husbands or even refuse to have sex with them, especially in the case of women who were dependent on men for fulfilling their material and nonmaterial needs (Go, Sethulakshmi, Bentley et al., 2003). In addition, a large body of international research reviewed by Parker, Easton, and Klein (2000) revealed several structural–environmental factors such as economic development, poverty, mobility including migration, seasonal work, and social disruption experienced due to war or political instability, gendered inequalities, and governmental and intergovernmental policies to create conditions for easy transmission of the HIV virus. For instance, studies have examined how gender inequality such as women’s unequal access to productive resources (for instance, land, income, education, and credit), sociocultural norms of sexuality, and unequal power dynamics in intimate-partner relationships to enhance women’s risk of HIV infection (Amaro, 1995; Amaro & Raj, 2000; Gupta, 2004; Zierler & Kreiger, 1997). Similarly, trafficking laws in India, such as Immoral Traffic Prevention Act, 1986, are used by law enforcement authorities to arrest, harass, and abuse women in sex work (Lawyers Collective, 2003; World Health Organization [WHO], 2005), further exacerbating the stigma and discrimination associated with sex work and HIV in India (Mawar, Sahay, Pandit, & Mahajan, 2005) and limiting women’s access to HIV preventive health services.
Despite increasing evidence in research that it is the interplay between individual, sociocultural, structural–environmental factors that enhances women’s vulnerability to HIV infection (Blankenship & Koester, 2002; Bletzer, 2003; Esther-Epele, 2002; Gupta & Weiss, 1993; Rhodes et al., 2012), most HIV prevention programs reaching out to women sex workers in India are focused on the individual-level risk factors, with emphasis on condom promotion and distribution as the HIV risk reduction strategy, ignoring the role sociocultural and economic factors play in determining women’s health-seeking practices. The most common HIV prevention programs in India are the National AIDS Control Program (NACP), implemented by the NGOs with funding received from National AIDS Control Organization (NACO). The main components of the NACP model intervention are HIV/AIDS surveillance; behavioral change through education information and communication; screening, detection, and treatment for sexually transmitted diseases; and condom promotion. While the findings of a Kolkata-based ethnographic study reveal that women in sex work have a holistic view of sexual health that includes physical, social, economic, and mental well-being (Evans & Lambert, 1997), the definition of health within these HIV prevention programs is narrowed to mean sexually transmitted diseases alone, ignoring the emotional and physical health needs of these women. Moreover, the HIV prevention programs reaching out to flying FSWs are modeled on programs designed for brothel-based sex workers. For instance, the Sonagachi Project, a community mobilization HIV prevention program, implemented by the Durbar Mahila Samanwaya Committee, an organization of sex workers working in Kolkata’s red light area of Sonagachi, has been internationally recognized for keeping the rates of HIV infection low among women sex workers (Pardasani, 2005). However, replicating the Sonagachi model of HIV prevention based on identity politics has been a challenge among flying FSWs because women do not identify themselves as a sex worker as they possess multiple, fluid, shifting identities throughout their course of life. Scholars have argued that a community mobilization strategy, although a critical part of HIV prevention, cannot become a substitute for bringing about broader social, political, and economic changes in the structures that are responsible for enhancing the risk of HIV among sex workers (Asthana & Ostovogels, 1996; Pardasani, 2005). Therefore, it is imperative that HIV prevention programs be based on the risk experiences and risk perceptions of women working in diverse sex work settings as they experience different levels of vulnerability for contracting STDS, including HIV/AIDS. For example, while HIV practitioners perceive women sex workers’ practices of engaging in unprotected sex with regular partners to be a risk behavior, women in sex work might perceive this act to be a symbol of trust and intimacy in their relationship. That is, the act of unprotected sex could mean different things to different people depending upon the settings, social networks comprised of interpersonal relationships, sociocultural norms within those settings, and the larger political and economic contexts within which sex work is organized. However, there are no studies till date that have examined risk from the point of view of flying FSWs and their perceptions of the NGOs sexual health outreach projects. This article fills this gap in the literature by examining HIV risk from the point of view flying FSWs and aims at answering the following questions: (a) What do flying sex workers perceive as being risks to their physical, social, and economic well-being? (b) How relevant is the risk of HIV compared to other risks in the lives of these women? and (c) How do they perceive the NGOs sexual health outreach services?
Method
This article draws from the analysis of a larger ethnographic data collected by the author in Kolkata, India, from December 2009 to July 2010 and the author’s work experience as a project manager in a sexual health outreach project for street-based sex workers in Central Kolkata, India, from February 2004 to July 2005. Access to the participants of this study was sought through the sexual health outreach projects of the local NGOs funded by NACO to reach out specifically to this subgroup of sex worker population.
Data Collection Procedure and Tools
For this article, the author relies on the 46 short-life portraits, field notes on the intensive observations of the clinic hours, and the focus group meetings held for “flying” FSWs by the NGOs. A considerable amount of time was spent observing the sexual health outreach services of the NGOs, resulting in informal interactions with a group of three law enforcement authorities, five counselors, two clients, two doctors, and three funding agency representatives, four governing body members of the NGOs, and interactions with common people. Maximum variation sampling approach (Miles & Huberman, 1994) was used to select the 46 short-life portraits informants, as it allows for incorporating the experiences and perspectives of diverse groups, such as women who were illiterate versus literate, recent versus longtime members of the sex industry, young versus old, sex worker support group members versus nonmembers, and from diverse sex work settings. The 46 short-life portraits were collected in the form of contact summary sheets (Miles & Huberman, 1994), which included information on demographic questions (age, marital status, education, brief history of employment, duration of sex work, number of children, membership in organization, organization of sex work [independent, through intermediaries], age of entry in sex work, family background, risk and safety issues faced during work, HIV risk perceptions, and reasons for entry into sex work). The technique of participant observation was used to highlight the intersectional identities of women sex workers and to assess the impact of interlocking systems of oppressions on the lived experiences of these women. The author accompanied the peer educators 2 to the field 3 sites and assisted the NGO staff in carrying out activities like offering counseling services to women and conducting outreach services on the field, which resulted in gaining access to diverse subgroups of flying FSWs. Extensive field notes regarding women’s responses to risks in the solicitation sites and their attitudes toward the outreach activities of the NGOs were maintained throughout field work. The everyday writing of field notes enabled a better understanding of the themes, issues, confusions, and questions that emerged while interacting with women and NGO staff. The short-life interviews were conducted in Bengali and Hindi by the author. The style of interviewing was mostly informal, using more open-ended questions to gain insight about women’s experiences while negotiating health-seeking practices with their clients and their perceptions about HIV risk. The technique of repeated interview methodology (Wax & Shapiro, 1956) was used to gain information in greater depth and also to check for any inconsistencies and fabrications within their narratives as the relationship between respondent and the researcher develops with frequent encounters. Therefore, all 46 short-life portraits included in this study were reinterviewed from 2 to as many as 4 times. Verbal informed consent was taken prior to each formal interview and the participants were explained the purpose of the research and participants were also given the time to seek any clarifications with regard to the research project. Pseudonyms were used to maintain privacy and confidentiality of the participants. This study was approved by the Institutional Review Board of the University of South Carolina, Columbia.
Data Analysis
All audio-taped short-life portraits were translated and then transcribed verbatim into English by the author who speaks Hindi, English, and Bengali fluently, using the qualitative research software, Nvivo 9. The process of translating and transcribing the field observations verbatim into English on the computer on a daily basis enabled the author to keep a check of the “reactive effects” and issues of transference and countertransference that emerged on the field. After the interview transcript was prepared, the copies of the transcript were reviewed for accuracy and appropriate representation of the respondents’ thoughts by listening to the tape and matching it against the transcript and wherever necessary corrections were made. The data were analyzed using Nvivo 9. A line-by-line coding was undertaken. Each transcript was read and coded for prominent themes or domains. These themes were refined or new domains added as new data were analyzed.
Sociodemographic Characteristics of Participants
Of the 46 short-life portraits, 25 participants worked as peer educators in the sexual health outreach projects of NGOs, 14 participants were regular visitors of the NGOs, and 7 women were accessed from the solicitation sites, as they were reluctant to be involved in the NGO activities. Age is a crucial determinant of women’s ability to earn in this industry, as several women expressed that the demand for young women is high in the market, especially in brothels. Therefore, older women face severe competition from their younger counterparts residing in brothels. Most of the women in this study were above the age of 30 and they canvassed a huge area to get their clients. Women above 40 were not sexually active themselves, but earned a living out of the sex industry by arranging new girls for their old clients. Women often used the following phrase to depict their concerns about age: “the older you get, the ‘meter’ goes down.” With regard to marital status, 89% (41) of them had been married before 18; 58% (27) of them got married before the age of 16. However, 56% of the marriages resulted in divorce, separation, or desertion. Seventy-four percent of women had two or more children within the first 3 to 4 years of marriage, which indicates that the social pressures of marriage and motherhood are huge for women in Indian society. Table 1 provides a summary of the selected sociodemographic characteristics, including age, education, marital status, type of sex work settings, number of children, age at marriage, and membership in organization of the flying FSWs.
Sociodemographic Characteristics of the Study Participants.
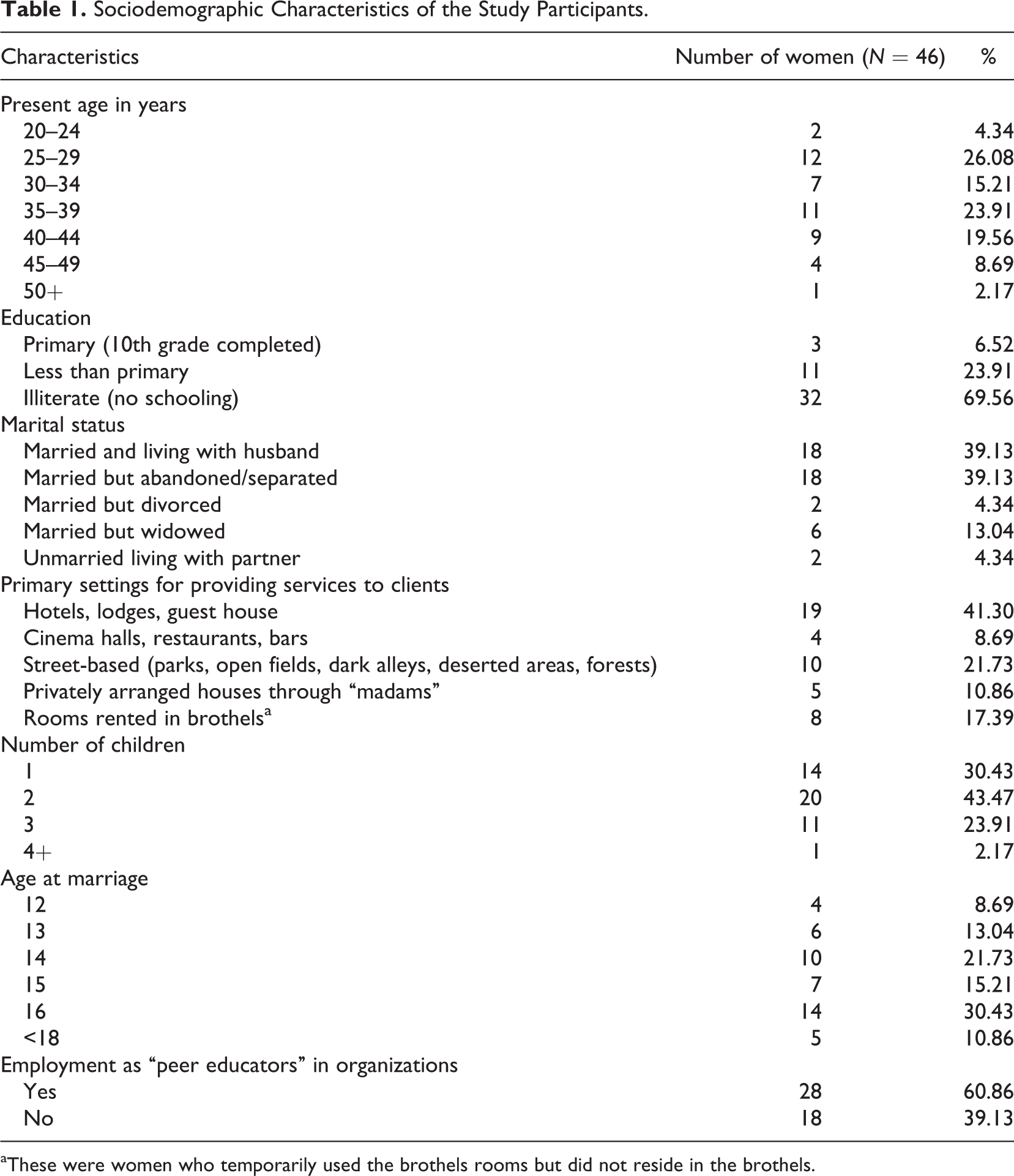
aThese were women who temporarily used the brothels rooms but did not reside in the brothels.
Results
Risks: Multiple, Interrelated, Context Specific
The flying FSWs perceived a wide range of risks to themselves and their families. The risk of HIV was one among many other occupational risks, such as fear of “whore stigma,” risk of police arrests, client-initiated violence, intimate-partner violence, and health-related risks, such as physical, sexual, and mental health problems, including HIV/AIDS. However, the perceived risks or fears of these women varied depending on the physical context of sex work (open fields, jungles, brothels, privately arranged flats, bars, cinema halls), time of work (night vs. day), duration of work (regular, weekly, occasionally), nature of clients (local goons, “party boys” (muscle men), “gaari party” (clients requiring sexual services to be performed in moving vehicles), and socioeconomic background (determined by their caste and class positioning in society). For instance, Madhuri, who arranges customers over the telephone and provides services to them in privately arranged flats or lodges, differentiates her HIV risks and vulnerability from women working from the streets, as she screens her clients by talking to them over the telephone and avoids places patrolled by police or law enforcement authorities: I don’t go to jungles or open fields that I should fear. I go to lodges and he pays for the lodges. I do the work and leave the place. I don’t have anything to fear. I don’t ‘stand’ on the roads. I talk on the phone. I give them (customers) my mobile number. I don’t go together. If I go together then it will create problems, so I never go together. He goes first and then I join him later. This way nobody gets to know. (Madhuri, 28 years)
Similarly, Sheetal, a 25-year-old woman, believes that working in the nights and visiting the solicitation sites regularly can prove to be more dangerous. Therefore, she avoids working in the nights to stay away from trouble: I don’t go to work every day and I am not staying in the nights, so I am not scared. I work in the afternoon. I get scared when it gets dark. Just a few days ago in the lodges where I take people; a boy killed a woman and left her behind in the lodge. The hotel/lodge owner is now in such a problem. He is running pillar to post with court cases and visits to the police stations. The girl had stayed overnight. That’s why I fear staying overnight. The boy killed the girl by suffocating her with a pillow in the night. In the morning, he got out of the room pretending he was brushing his teeth and went away. He never returned. Later, the hotel people found the girl’s dead body in the room.
Women categorized their customers as “bhalo” (good/well mannered) and “nongra” (dirty/ill mannered) and their perceptions of HIV risk differed depending on the type of customers they serviced: I don’t go to problematic places, therefore I face no problems. I only pick ‘good’ customers (she defines good as those who are willing to pay for the service, well-mannered, and polite). I won’t go out with ‘nongra log’ [dirty people]. If those people appear to be good and polite, then only I go out with them …. How come you don’t know about Sonagachi. Raids are so common in this area. Raids are very common in Sonagachi. I avoid those places. (Reema, 40 years)
Similarly, Trishna and Sanchita, who have had experience with providing services to clients in moving vehicles and people holding political offices, contend that “gaari party” and “party people” should be avoided at all cost: The ‘gaari party’ is ‘heavy’ risky. While you are giving service to them, they will take to you deserted place and drop you off there and since you can’t do anything in those places, he will drop you off with no money. (Trishna, 48 years) I went with this man in his car. He took me far away and left me stranded in the midst of nowhere. I had to walk for miles. (Sanchita, 30 years)
Women’s perception of HIV risk also differed depending on the nature of sexual services offered to their clients. For instance, women who operated from bars, cinema halls, and restaurant cabins spoke mostly of offering “hand-jobs” or “oral jobs” did not think they had to do worry about HIV/AIDS: Today, when I leave from this office, I’ll do one or two party and then go home. I work in the bars and hotels. There are many men who do not want to sit alone and just seek your company while they are eating their food, drink, or smoke. So I provide them company and I don’t do the ‘act’ but just a kiss and fondling of private parts. (Meenati, 37 years) I go there (open fields). I will go and sit there for 2 or 3 hours. I go there to do ‘adda’ (socialize) but I don’t do this work (act). I would only do kissing and touching each other private parts. It is only little. I just pull his thing until his ‘thing’ comes out. (Kaya, 38 years)
Risk of “Whore Stigma”
“Whore stigma” defined by Pheterson (1990) as a “social and legal branding of women who are suspected of being or acting like prostitutes” was explicitly discussed by 15 women in their narratives. In general, women were quite aware of the ways in which “whore stigma” operated in society, as they repeatedly made comments like “This is not any work,” “You can’t say to people that you do this,” “It is a matter of ‘prestige’ in society,” “It will be a big shame for me if people get to know about my work,” “There is no respect and social recognition for this type of work,” and “I don’t want a bad record.” The following excerpts illustrate how the “whore stigma” manifests in the everyday life of these women, as it results in severe life-threatening consequences, such as loss of self-respect and “izzat” (honor) in society, marital conflict, violence, endangerment of their children’s future, and police arrests on being identified a “prostitute”: I fear the consequences if people get to know about this work. If someone in the neighborhood gets to know they will drive my family away. I have to be very careful while doing this. Once, it has happened. I was getting down from the car and this person saw me. Later he asked me where I had gone. Then I told him ‘I work in an NGO and for that I need to take people to hospital and I am returning from there.’ I show them the identity card issued by the organization. I was able to put things under cover. I never went there anymore for I knew if they see me again they’ll get suspicious. I am not doing any more ‘party’ (customers) because my sons are growing. If his friends get to see me anywhere then it will be a big shame for me. I fear my sons will abandon me. (Minati, 30 years, peer educator) I am ashamed of what I do, and if my parents get to know this, it will be too painful a truth for them. We stay in a ‘para’ (neighborhood). We will lose the social standing and respect in the community. If they get to know about this, they will drive us out of our house. (Lipika, 27 years)
Several women also reported that women maintained mobility for sex work in order to escape the permanent stigma that arises from working in brothels: No, No. I don’t operate from a fixed place. In one place if you go regularly, will you not find out about my work? If someone sees something or gets to know, then it looks I did work with one man, then 10 others get to know and I get identified as a ‘whore’ then they will harass me. So I have to float around and do this to avoid public harassment. (Payal, 32 years)
Risk of Police Arrests
Eleven women expressed concerns related to police raids, arrests, and harassment. Trupti, a widow who works from hotels or lodges, speaks of the wide discretionary powers exercised by the police authorities in the treatment meted out to women in sex trade: They catch us and then put us in ‘jail’ for a night. Some of them will impose a ‘fine’ with the charge of creating nuisance in public places. There are some who will ask for money and leave us. (Trupti, 40 years)
Whereas, Putul, a 40-year-old illiterate widow, who works in open fields surrounded by bushes, experiences harsher treatment such as physical beatings by police authorities: I was beaten by the police so badly (showing me the body parts in which she got the beatings) that I still have marks of those bruises on my hips and legs. I can’t even talk about my arrest with my family. All my daughters are married. If my son-in-laws and other relatives get to know about
Dharna and Saraswati, who solicit clients from the streets, illustrate how a police raid put their lives in jeopardy: There are few ‘baadi’s’ (houses) where police conduct raids and arrests. That is the only problem. They don’t do it every day. It happens once in a while. You don’t know when it happens. That is what I have in my mind all the time. (Dharna, 25 years) You can’t do anything when raids happen. You got to run for your life. (Saraswati, 35 years, peer educator)
The law enforcement authorities view the solicitation practice of women in public spaces as a “law and order” problem and random operation of raids force women to frequently change their fields of operation, limiting their access to health care and HIV preventive resources. Despite being a government-funded program, the NGOs need to take permission from the law enforcement at all levels of institutional hierarchy, in order to carry out their outreach services in the field. For instance, Kakuli, an outreach supervisor, illustrates how she was interrogated and harassed by police authorities while reaching out to women in the field: I didn’t know I had to inform the police before visiting the ‘field’ (solicitation sites). I was once roaming on the platform along with the peer educators to speak directly with other women, but was stopped and interrogated by the police officers. They said ‘Our head officer wants to meet you in ‘office’. So you got to come with us to the ‘office’. I had to go with them to the ‘office’ and they asked me a few questions. I showed them my ‘ID’ (identity card issued by the organization) and then they left me. What to do their job is to interrogate, so we can’t even blame them. We got to cooperate. (Kakuli, outreach supervisor)
Women who were found possessing a large number of condoms by the police could face arrest on charges of prostitution or trafficking, as made evident from the several narratives of peer educators who face considerable risk on the field making condoms accessible to women: Sunny di, we work on the field with great caution. If someone gets to know that we do all this (sell condoms), they will drive us out of the community with a broomstick. (Swarna, 40 years) We have to be very careful when reaching out to the women in the field. We never take our condom bags. We have to hide our stuff (condom) when interacting with the women. (Naina, 45 years) I sometimes hide condoms in my blouse or carry it in my palm with my mobile so that no one knows I am giving anything to them, otherwise the neighbors would want to know why I come, and what I handed over to the women. (Swarna, 40 years)
Fear of Violence
Women reported experiencing sexual violence in the hands of both nonpaying intimate partners and their paying client. The client-initiated violent acts and behaviors, as described by women in their narratives ranged from minor thefts, verbal abuse and intimidation, threats of harm to family, harassing phone calls, forcefully injecting drugs, physical assault, sexual coercion, and trafficking. The following narratives from Shilpa, Trishna, and Aparna suggest how forced use of drugs and sexual violence restricts women’s ability to negotiate safer sexual practices: While working in this line, I used to work in a ‘bar.’ From there a few boys attacked us. They stopped a car and forcefully got us in that car—we were three and they were seven boys and 1 driver—they forcefully took us. They took us and raped us—they took us to a broken house and then forcefully did it with us. Then they leave us. We were wearing gold ear rings. They took those away. Then we didn’t’ think it was appropriate to tell any of the villagers. We didn’t inform anyone. (Shilpa, 32 years) I went in the night with 2 boys to their flat. I needed money. They looked decent. When I reached their flats, I found five boys were there. They threatened me and asked me to keep quiet. I quietly did ‘it’ with them. Nobody took condoms. It happened four years ago. I just waited for the sun to rise. In the morning, I left. I was given only Rs. 150 ($3) and travel money Rs. 30 (>$1). Even now, I worry if I meet those boys again. (Aparna, 37 years) Once I took a customer. I picked him up from ‘VIP’ road. He drugged me so much, took away my belongings, and left me on the street. I was picked up by Organization A and brought to their center. (Trishna, 48 years)
Similarly, the following narratives illustrate forced sex to be a reality for women within marital relations: My husband forced me to elope with him and coerced me to marry him. He used to beat me up. I have two sons. I didn’t want to have any child from him but I was raped on several occasions. My sons have grown up so he cannot rape me now. (Roma, 41 years) He would come very late in night. I would go to sleep after working all day and he come late in night and would do
Risk of HIV
A culture of silence prevailed when probed with the issue of HIV/AIDS. A typical rehearsed response that women provided when probed about their HIV risk is: “How will I get it? I don’t do “How will I get it when I use ‘cap’ always with my customers?” (Hearing this Saraswati who is a peer educator says “yes, if you know this nothing will ever happen to you.” (Harini, 30 years) This AIDS disease. What does this disease means? We are mingling with several people, now if the boy has this disease and I don’t have this disease, then if this boy comes close to me then the disease will enter my body, or if I have the disease then it will get into the boy’s body. Therefore, we have to use “caps” and do all our work. Tell me, am I not correct about it? I always use condoms and do work or else I won’t do any work. (Dharna, 25 years) How will it happen? (She throws back a question to me). I don’t do it empty. I use “condoms” all the time I do this. If I do two or three work outside, I use condoms. I don’t do empty. How will HIV happen to me? Even by mistake, I will not do it. I won’t get work, I won’t do it. I don’t do it without condoms so how will I get? (repeats again; Madhuri, 28 years) I work with caution (use condoms) so how can I get infected with HIV? (Priti, 39 years)
Quite a few women expressed a fatalistic attitude when probed for their HIV risk: Why will HIV happen? If it happens then it is god’s wish. I use condoms all the time. I work with caution. (Reema, 40 years) Does condom usage give 100% protection against HIV? It is quite possible for the condom to wear and tear and HIV to enter the body. No one can say what will happen. If it is destined to happen, it will happen. (Spoken in a fatalistic and agitated tone; Trupti, 30 years)
Although the women were informed and educated about using condoms and quite eloquently spoke about consistently using condoms with their customers in their one-to-one interviews, they did not seem to have much control in enforcing the use of condoms with their clients in the context of violence and poverty: Just telling me to use condoms will not work. You got to speak with other girls in the ‘market’ too. Clients go with girls who are willing to do without condoms. I will not be able to enforce using condoms if other girls are taking clients without condoms. I can stand the whole day but will have no business. (Shruti, 28 years) I went in the night with 2 boys to their flat. I needed money. They looked decent. When I reached their flats, I found five boys were there. They threatened me and asked me to keep quiet. I quietly did ‘it’ with them. Nobody took condoms. It happened four years ago. I just waited for the sun to rise. In the morning, I left. I was given only Rs. 150 ($3) and travel money Rs. 30 (>$1). Even now, I worry if I meet those boys again. (Aparna, 37 years)
Similarly, women’s lack of complete knowledge about their HIV risk was evident as they could barely articulate the other routes of HIV transmission (anal or oral sex) and connect the use of condoms with other reproductive health problems such as unwanted pregnancy and STDS: I don’t know how No, I don’t know that. I will have to ask ‘didi’ (peer educator). I don’t know. I don’t know how HIV spreads. My ‘didi’ (peer educator) told that if I wash with Dettol (antiseptic) after doing it, then nothing will happen to me. (Payal, 32 years)
Several misperceptions related to HIV/AIDS were also found in the narratives of the women hired as peer educators within the project. For instance, quite a few women did not worry much about HIV/AIDS because they felt going out with selected few customers was not risky in comparison to going out with many customers in a day: I am not like, shakshi (another girl). She is a ‘jaghonno’ (dirty) girl. I also take customer but only a selected few. She goes with any guy who approaches her. (Chulbuli, 28 years) No, I use condoms. Only with people I love, I don’t use condoms but all other work I use condoms, then how will I get AIDS? The fear is not there for I do regular blood check-ups. All my tests are fine. Till now, I have not faced any problem. I don’t mingle with 8 to 10 customers in a day. I mingle with 1 or 2 people and it is the same person. I do with ‘babu Lok’ (people working in government offices). (Priti, 39 years)
Similarly, women also carried the misconception that visiting certain “places” (brothels) and mingling with certain groups puts people at risk of HIV: No fears ‘didi.’ What fears? I don’t stand in bow bazaar or Sonagaachi (brothels). I pick up clients from Raza Bazar. I take Rs. 100 ($2) for 1 shot. (I clarify with her if it is 100 rupees for an hour or 1 shot). I take only known clients, no strangers. Everything is all right with god’s grace. (Meera, 35 years) Gram’ (village) people are very innocent; one can trust them so I offer services to them. (Rose, 40 years)
Quite a few women also spoke about engaging in self-medication practices to treat their sexual health problems, which illustrates that merely informing and educating women about HIV/AIDS does not translate into health-seeking practices: You know ‘tamarind water.’ I know this that if you take one glass of tamarind water right after doing Not now, but I had it earlier. It would itch so bad and would try to wash it with soap plenty of times but still it would itch so badly. My ‘didi’ (peer educator) told me that if you wash up just after doing
Women’s Perception of the NGOs
In the NGOs, where most of the interviews and observations were conducted, the NGO staff comprising of doctors, counselors, and outreach field supervisors, who were mostly members outside of the sex industry, perceived HIV/AIDS to be a sex worker’s disease: This project is to prevent AIDS. It is not for everyone but it is mainly targeted towards ‘prostitute.’ Because those who are ‘prostitutes,’ those who are sex workers, they need to be educated because once they are educated the ‘spreading’ will reduce a lot. The general public is less affected by the virus but the sex workers/prostitutes are mostly carriers as it is through them the disease spreads. If we stop the virus in them, then we can stop the spread of the virus too. (Doctor) It (HIV testing) is not for us, it is for them (peer educators/sex workers). They are the ones who are going about sleeping around with so many people. (Field supervisor) Why would the government focus on sex workers, if everyone could be affected by the disease? It is they who have so many customers, so they are the ones who need these services. (Outreach worker/supervisor)
Clearly, the HIV/AIDS discourse practiced by the NGOs and their negative attitudes and beliefs adversely affect these women in the community. Sanchita, who has been in the sex industry for more than 5 years, illustrates how the HIV/AIDS discourse practiced by the NGO staff has further marginalized and stigmatized their position in the community by ruining their business, as she is suspected by her clients as being a carrier of the disease: Is it true ‘didi’ (sister) that only we can be infected by the HIV disease? Can’t you and other girls who are not in sex work get this disease too? For example, your boyfriend could be cheating on you and he could infect you too? You know this HIV/AIDS talk has really ruined our business. Nowadays customers are very suspicious of us and if we are little bit unwell, they fear that we might have HIV in our bodies. I tell them “You are suspecting me, how do I know that you don’t have it? You too are going out with several women.” (Sanchita, 30 years)
Quite a few women in the sex industry were highly suspicious and distrustful of the HIV prevention messages received by the NGO staff, as it remained solely focused on their sexual health problems arising from unprotected sex with their clients, without taking into consideration their risk of contracting HIV infection through nonmonogamous intimate partners or institutional violence such as police atrocities: I don’t understand their (NGO) messages. I do it with my husband without condoms. Nothing happens to me. He goes to other women in the brothels. (Mou, 28 years, peer educator) I think it is government’s conspiracy to target us and get rid of us. The NGOs are helping them; otherwise they would have come to our rescue during police raids and arrests. What is the point in visiting the NGO when they don’t help us when we are in real need of them. (Trupti, 40 years) HIV/AIDS can happen to a ‘doctor’ or ‘nurse’ too. Am I not right? It can happen when he is seeing a patient and accidently the needle he used to inject the HIV infected patient pricks him too. Nobody knows about their HIV status unless they test themselves, then how do they say that HIV can happen to us only. I don’t believe them. (Swarna, 40 years)
While the peer educators brought issues of poverty, gender inequality, intimate-partner violence, client-initiated violence, stigma, and discrimination associated with sex work and HIV/AIDS to the NGOs, the NGO staff made it a point to reiterate to the peer educators the NACO program guidelines, which prescribes condom promotion and distribution as a sole strategy for preventing HIV risk among sex workers. Quite a few peer educators felt infantilized and humiliated by the organization’s repeated emphasis on condom distribution and promotion, as made evident from the following narratives: They have nothing else to do, other than this (condom demonstration meetings). How many times will they show us the same thing again and again? (Condom demonstration sessions) It is so irritating. (Priti, 39 years, peer educator) We ask them to find us work, but they tell us you do ‘this’ (sex work) and earn your living. This project is for us, but the organization gets to decide how the money is spent and used in the community. We just get paltry salary from the organization. That too, we have to wait months as the funds don’t arrive timely. When we ask the organization to pay our salaries, they tell us you can do ‘this’ and earn your living and we shouldn’t rely on the organization salary. You tell me, does this look fair to you? I’ll ask you to write all ‘bad’ about this organization. (Saraswati, 35 years, peer educator)
The NGO staff’s understanding of HIV/AIDS was driven by biomedical perspective, which assumes that problem of HIV/AIDS can be solved by exclusively focusing on the biology and individual-level factors, therefore the emphasis on screening, detection, and treatment. Based on the intensive hours of observations of the NGOs sexual health outreach projects and the 46 short-life portraits of women, it was made quite clear that this information-based condom promotion and distribution program was having only a limited effect in reaching out to flying FSWs. Several peer educators and the sex workers in the community complained about the NGOs practice of requiring women to identify and register themselves as a sex worker in order to avail the sexual health clinic/outreach services of the organization, as it increased their risk of stigma and discrimination in society from being labeled a sex worker. The comment from Saraswati, a peer educator in the sexual health outreach project, aptly reflects the sentiment of most of the women on the NGOs use of targeted approach to HIV prevention: We are not sex workers. We can be mothers, wives, daughter-in law, sister, and daughter to someone too. We ask the organization for alternative employment opportunities but they ask us to do
Even if women came to the NGOs experiencing rape or sexual violence, there is no provision made within the NACO budget for offering postexposure prophylaxis (PEP) treatment or even emergency contraceptive pills (ECP). The rationale offered by the NGO staff for not making PEP or ECP-related information available to the women was as follows: PEP is not meant for ordinary girls like them. They can’t afford this treatment. Moreover, there is no provision within the NACO budget for PEP treatment or ECP. Therefore, we ask them to get themselves tested for HIV after 3 and 6 months to become aware of their HIV status. (Project manager)
For HIV/AIDS education program to be effective in promoting behavioral changes among this group of sex workers, basic preventive resources such as condoms, PEP, and ECP are made readily accessible to these women in their diverse work settings. It is also evident from the voices of these women in this study that any interventions to address the issue of HIV/AIDS need to begin with a careful consideration of the specific ways in which the risk factors for HIV manifests within the local community, in order to be able to develop an appeal for these programs within the community. For instance, the ongoing stigmatization and “othering” strategies practiced in rural areas are more severe than urban areas.
Discussion
The focus of this article has centered on rendering voice to flying FSWs whose voices are often silenced within the HIV prevention discourse and their health and social needs go unmet. Unlike the epidemiologists and biomedical practitioners who remain focused on women’s HIV risk, the flying FSWs expressed a range of concerns (unemployment, poverty, gender inequality, stigma, discrimination, drugs, alcohol, violence, arrests, marital or family problems) that came in their way of addressing effectively the issue of HIV/AIDs. Therefore, the health risks of women in sex trade “cannot be considered in isolation but must be contextualized as one hazard on a continuum of risks that sex workers engage in and are exposed to” (Sanders, 2004, p. 569). For women in this study, the risk of HIV is, in fact, only one among many occupational risks that they experience on a daily basis. Thus, the imminent risk of HIV is not considered the most serious type of danger to their health because of other prevailing immediate threats to their survival, such as the fear of “whore” stigma, police arrests, violence, and poverty.
Drawing on the notion of intersectionality (Hill Collins, 1999), the findings also suggests that while issues of “whore stigma,” police arrests, and violence and shame apply to all sex workers, the manner in which these issues affect the women vary based on their age, work setting, race, class, marital status, skin color, physical appearance, membership in support groups, and other social categories pertinent to the local context. For instance, an older married woman belonging to a lower class is more vulnerable in the sex industry because they face stiff competition from the young, single women from higher class and therefore succumb to pressures from clients for unprotected sex. Similarly, sex workers who provided services on streets and dark alleys were more prone to experiencing sexual violence, police arrests, and public harassment than flying sex workers who operated from hotels, bars, or restaurants as they came from poor socioeconomic backgrounds. Therefore, the intervention programs reaching to women sex workers include work setting as another dimension of intersectionality, as the individual experiences of the flying FSWs with the intersecting systems of oppressions or “isms” plays out differently across varied work settings.
Implications for HIV Prevention Programs
A number of key issues emerged from the interviews with women and observations of NGOs sexual health outreach projects for consideration in the implementation of HIV prevention programs. First, there is an urgent need for HIV prevention programs to look beyond the individual factors and address the social mechanisms and contextual factors that increase these women’s risk of HIV infection. Most of the flying FSWs were at risk of HIV through their nonmonogamous partners, because initiating use of condoms with their partners conflicted with the requirement for married women to be dutiful to their husbands. Thus, refusing sex to their partners who participated in unprotected sex with other women resulted in more violence inflicted against them. This finding is particularly alarming because most HIV prevention programs lay emphasis on condom promotion and distribution when much of the risk experienced by women stems from male sexual behaviors. Obbo (1993) writes, “HIV transmission—men are the solutions” but still most risk studies continue to be focused on women’s behavior. More detailed studies aimed at understanding issues of masculinity, especially the social and cultural factors that promote behaviors like rape and violence against women, are needed. In order to promote women’s health, there is a need to increase male involvement in the HIV prevention programs, child rearing practices, and also domestic household work.
Based on the results presented here, it is evident that the legalities surrounding sex work in India puts socially and economically marginalized women at increased risk of HIV infection and gender-based violence. While several legal options (decriminalization, legalization, and self-regulation) have been discussed to address the issue of prostitution in India, the author recommends decriminalization of voluntary consensual sex transactions between adults. The decriminalization of voluntary sex between adults will enable women to organize themselves without the fear of police arrests at their work places and also frequently report incidents of violence.
Another important finding of this study was that the use of a targeted approach to HIV prevention based on identity politics further stigmatizes and discriminates these women. The traditional, narrow focus on the sexual behaviors of these women has resulted in a widespread belief that AIDS is a disease of the sex workers or homosexuals engaging in “dirty” work. It leaves unexamined the vulnerability and risk behaviors of individuals outside of the sex trade, putting the blame of HIV infection on the women by referring to them repeatedly in the HIV/AIDS literature as “reservoirs of infections.”
Implication for Social Work Practice
These findings have several implications for social work practice. First, social workers need to view women in sex work as “whole persons, rather than simply as ‘either madonna or whores,’ as vectors of disease, as wombs of procreation, or as ‘empty vessels’ into which the contents of medical information can be poured” (Schoepf, 2004, p. 131). As made evident from the narratives, women possess multiple, fluid, shifting identities throughout their course of life and the identity of sex work, once assigned and spoken in public, strips these women of their other identities, such as mothers, daughter, wives, or sisters, which they consider valuable and worth protecting. In addition, it is important that social workers take into account the heterogeneity among sex worker population, diversity of their risk experiences, and most importantly, focus on the resilience and agency of these women in designing the outreach services for the women.
Footnotes
Acknowledgment
I would like to especially thank Dr. Alice Bee Kasakoff for providing valuable comments and feedback that have helped to strengthen this article. In addition, I would like to thank several other people who have commented on the earlier drafts of this article: Dr. Naomi Farber, Aviral Shrivastava, Ilya Issenin, and Indulata Prasad.
Author’s Note
The views expressed herein are those of the author and do not reflect the policy or position of the funding agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by Fahs-Beck Research and Experimentation at The New York Community Trust and The Walker Institute of International Relations and Area Studies at the University of South Carolina.