
Abstract
Climate change, biodiversity loss, and pollution are disrupting earth’s biophysical systems, with adverse effects on local and global human health. Planetary health describes the inextricable link between human health and the health of earth’s biophysical systems. There is urgent need for a stronger focus on planetary health among healthcare systems and radiology departments. Medical imaging is a substantial contributor to climate change, responsible for 0.8% to 1% of global greenhouse gas emissions. As demands for medical imaging continue to grow, so will the need for radiologists to provide leadership in environmentally sustainable medical imaging. Mitigation strategies targeting overall reductions in environmental impact are pivotal including reducing the energy consumption of medical imaging equipment and establishing a circular supply chain to reduce unnecessary waste. In addition, radiology departments will need to focus on adaptative measures which build resiliency to the impacts of climate change, some of which will be unavoidable. This review aims to define planetary healthcare in the context of radiology and provide a framework within which to consider specific actions to reduce the environmental footprint of medically necessary medical imaging.
Introduction to Planetary Health and Radiology
Planetary health is a holistic systems view of the world, which conveys the inextricable link between the health of our planet and the health of human civilization (Figure 1). 1 While global health focuses on human health on a global scale, planetary health considers the health of humans in relation to the health of all living ecosystems and nonliving planetary biophysical processes.
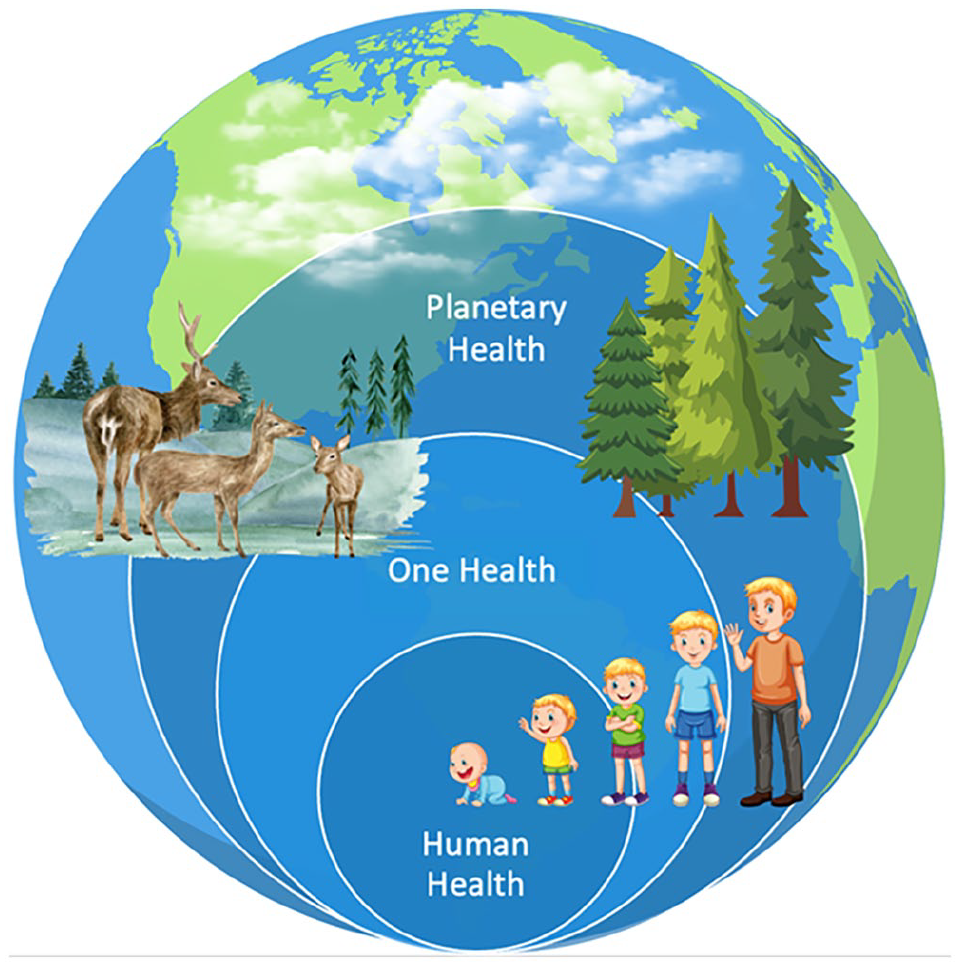
Planetary health.
Three interrelated issues caused by human activities are threatening the future of humanity and our planet, collectively a “triple planetary crisis”: climate change, biodiversity loss, and pollution. 2 Climate change refers to the long-term shifts in temperature and weather pattern primarily due to burning of fossil fuels, leading to increased atmospheric carbon dioxide (CO2) and other greenhouse gases (GHG’s). 3 Biodiversity loss describes human caused destruction of the living world, leading to the reduction or extinction of the planet’s living organisms contributing to food insecurity, reduced access to potable water, and the destruction of ecosystems. 2 Air pollution is one of the largest risk factors for premature death and disability, with the World Health Organization (WHO) estimating that 90% of people worldwide breathe air that exceeds WHO pollution guideline limits. 4 Globally, an estimated 7 million deaths per year are attributable to air pollution, with a recent report estimating that polluted air is associated with 15 300 premature deaths annually in Canada.4,5 Addressing the drivers of the triple planetary crisis, including reduction of burning fossil fuels, is a win-win for local and global health and mitigation of climate change. 6
The risks of inaction are becoming clearer. Global climate change is presenting record-breaking threats to human well-being and survival. 7 Direct impacts to human health and the ability of health systems to provide care occur due to extreme weather events and altered regional weather patterns. Hurricanes, flooding, and extreme heat events lead to physical injury, heat related illness, altered patterns of infectious and vector borne disease and adverse impacts on mental health.8,9 Alteration in the Earth’s biophysical systems indirectly impacts human health through reduced access to potable water, food insecurity, population displacement and migration, and interpersonal/international violence. 8 Between 2030 and 2050, an estimated 250 000 annual deaths are expected as a consequence of climate change from malnutrition, malaria, diarrhea, and heat stress. 10 Direct and indirect impacts on human health disproportionately affect low-income countries and disadvantaged and Indigenous communities within wealthy nations. 11
Healthcare is a leading contributor to climate change. A 2018 report found that Canadian healthcare was responsible for 33 million tons of CO2e annually, representing almost 5% of total national GHG emissions. 12 This is on par with the global environmental burden of healthcare, estimated to be responsible for 4% to 5% of all GHG emissions. 13 The global Greenhouse Gas Protocol accounting standards provide a framework to measure and report GHG emissions in healthcare. 14 Scope 1 emissions (26%) are emissions under direct control of the organization, including fossil gas boilers, fleet vehicles, and anaesthetic gases. Scope 2 emissions (13%) are indirect emissions from purchased energy generated offsite, primarily electricity. 15 Scope 3 emissions (61%) are indirect emissions which can be influenced by the healthcare system and includes the entire global supply chain of resource extraction, production, transportation, and disposal of medical and surgical supplies, medical devices, food, chemicals, and pharmaceuticals.
The environmental footprint of global healthcare has unsurprisingly continued to increase over the decades. Despite improved energy and resource efficiencies, the doubling of global healthcare spending over the 15-year period from 2000 to 2015 has led to increases in all aspects of healthcare-related environmental metrics including a 9% increase in particulate matter air pollution and 29% increase in GHG emissions. 16
Radiology is in a unique position within the healthcare sector as a significant contributor to climate change. In a single large Canadian radiology department serving 5 hospital sites, 3235 tons of CO2 equivalents are emitted annually, comparable to the energy required to power 422 single-family homes for 1 year. 17 Worldwide, medical imaging is responsible for approximately 0.8% to 1% of total CO2 emissions. 18 This is primarily driven by the massive electricity demand required to power medical imaging equipment. 19 Furthermore, the direct emissions produced on-site by the facilities and inhalational anaesthetics, as well as indirect emissions from the upstream supply chain and downstream disposal pathways, position radiology as a leading contributor, but also as a prime area of interest in ongoing and future sustainability efforts. 19
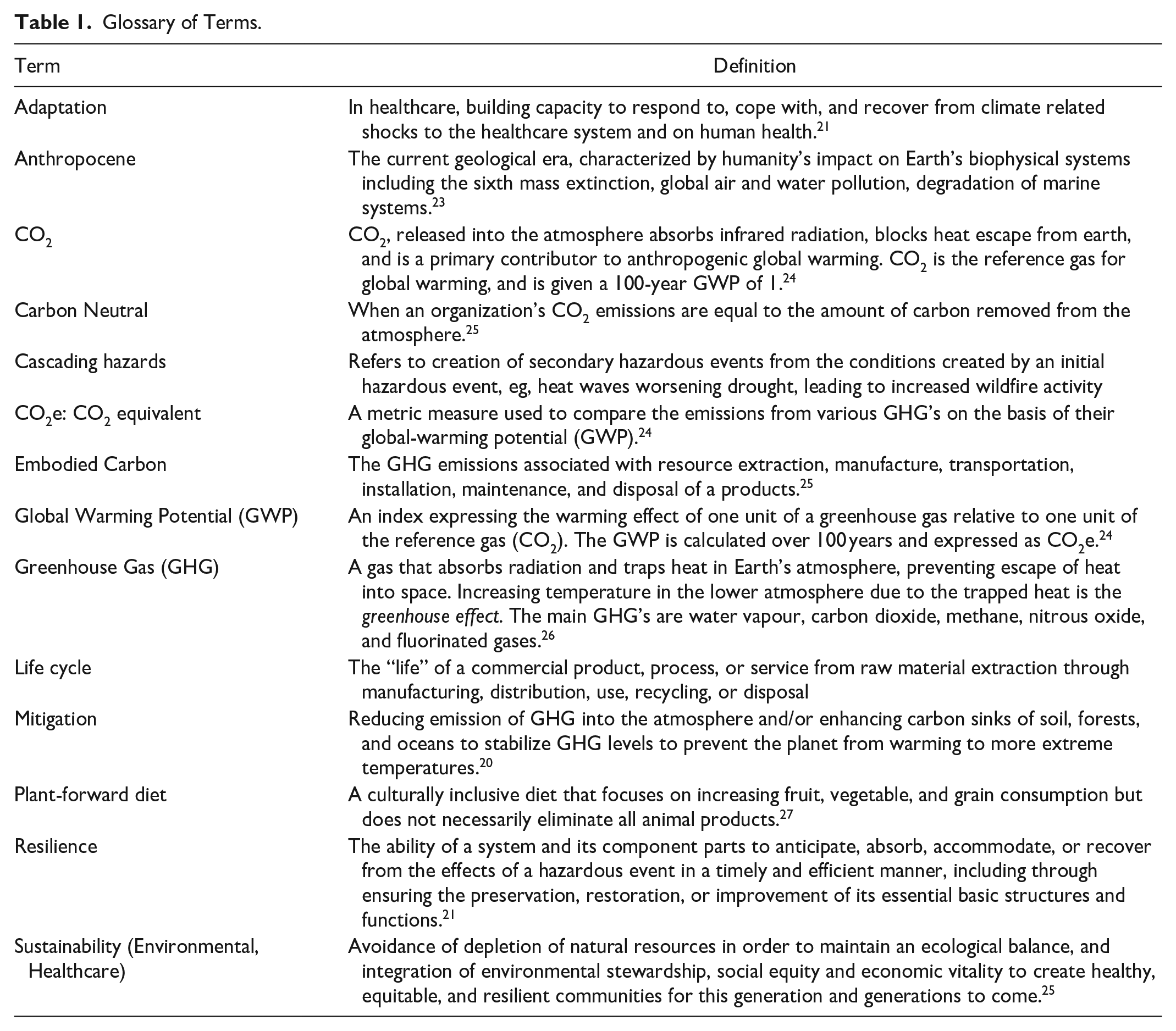
Reducing the environmental impact of radiology requires both mitigation and adaptation strategies. Mitigation is defined as efforts to reduce emission of GHG into the atmosphere and/or enhancing natural carbon sinks of soil, forest, and oceans to stabilize GHG levels to allow ecosystems time to adapt to prevent the worst impacts of climate change. 20 Adaptation in healthcare refers to the processes of updating institutional, behavioural, and infrastructural processes to build capacity to withstand the impacts of climate change on the healthcare system and human health. 21 Additional terms and their definitions pertaining to planetary health can be found in Table 1. This review outlines a planetary healthcare framework for radiology which includes expanding the focus on preventative care to reduce the need for resource intensive hospital care, ensuring the right exam is provided to the right patient at the right time, and optimizing the environmental footprint of medically necessary medical imaging. 22
Glossary of Terms.
Framework for Sustainable and Low-Carbon Radiology
There are 3 key principles to practicing environmentally conscious radiology that can be adapted from a framework proposed by MacNeill et al in 2018 (Figure 2). 22
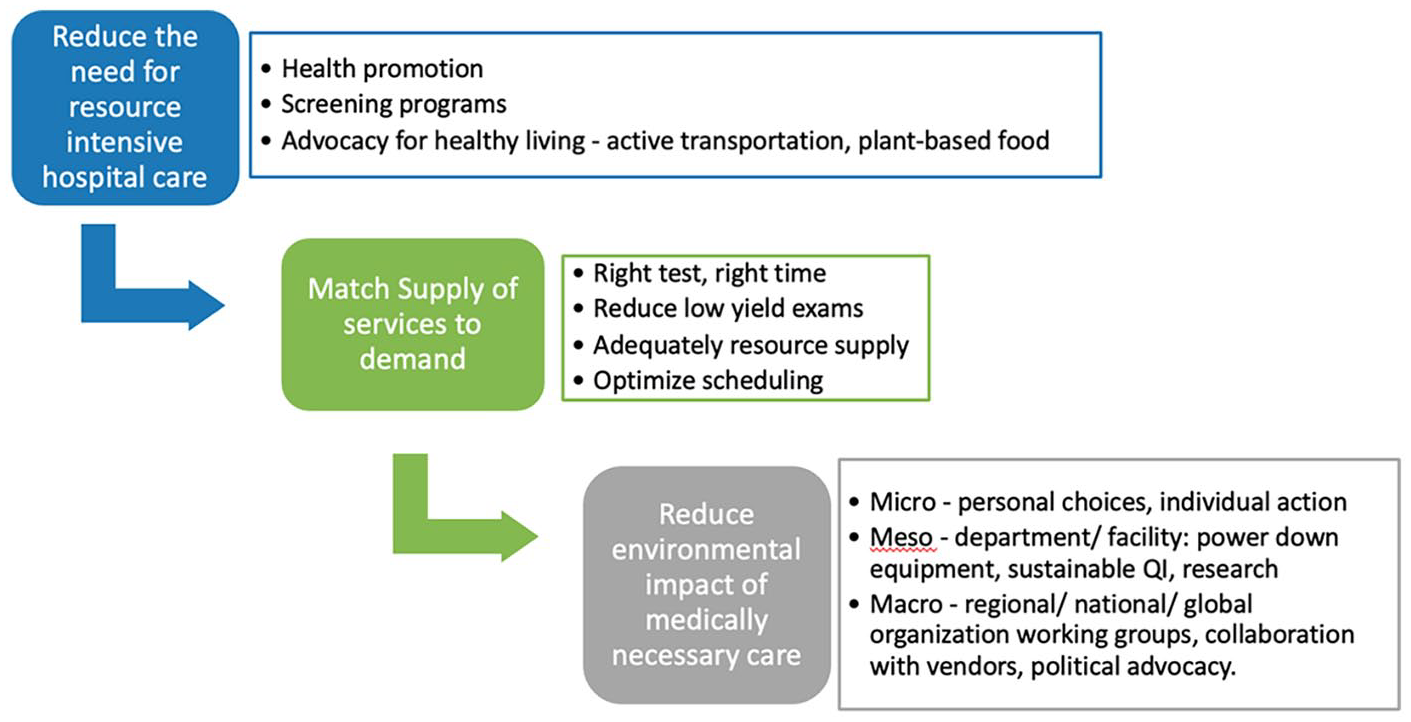
Planetary health care framework for environmentally sustainable radiology.
Reduce the Need for Resource Intensive Hospital Care
The provision of care in the hospital setting requires a significant use of resources and energy, with a study from the United Kingdom demonstrating that the average inpatient admission produces 125 kg of CO2 equivalents per day. 28 Both from a patient outcome and sustainability perspective, it is imperative that healthcare practices are shifted away from reactive care to a focus on preventive care. For patients and providers, this includes health promotion at both a micro (personal) and meso (facility or regional) level such as advocating for active transportation and plant-based foods for the home, work, and when being cared for at the hospital. The provision of effective screening programs can also promote preventative/early less-intensive care. In the case of breast cancer, recent recommendations by the US Preventative Services Task Force state that women from the ages of 40 to 74 years receiving biennial screening mammography will result in an average of 165 life-years gained among a cohort of 1000 women (just over 8 deaths averted). 29 In the case of lung cancer, screening guidelines recommend annual low-dose CT among heavy smokers from the ages of 55 to 74 years as evidenced by a 20% reduction in lung cancer-related death. 30 While the environmental impact of screening radiographs and CT scans are not negligible (mean carbon emissions of 0.76 and 9.2 kg CO2 equivalents per scan, respectively), screening programs can help mitigate the costly care downstream from advanced cancer and complex inpatient hospital management. 31 There is an argument to be made that screening programs through reducing mortality may paradoxically increase an individual’s lifetime carbon footprint and only delay inevitable end-of-life care (and its associated high carbon footprint), but from an ethical and environmental standpoint, improving patient outcomes while mitigating upfront environmental impacts are central to the importance of effective secondary prevention, while also providing more time for mitigation and adaptive strategies to develop and take effect. 32
Match Supply of Imaging Services to Demand
The increasing volumes and growing demands on radiology departments across the nation cannot be understated; from 2017 to 2040, the number of CT examinations is expected to more than double from 5.6 million to 11.9 million and the number of MRI examinations is forecasted to experience even further growth from 1.9 million to 5.3 million. 33 Imaging deemed to be “low value”—in other words, performed without an appropriate clinical indication, achieving little to no value in patient management decision making, and ultimately resulting in healthcare resource waste—is pervasive and estimated to account for 2% to 24% of imaging studies in Canada. 34
Strategies for the reduction of low value imaging have been proposed and thus would drastically mitigate the planetary health impact of medical imaging. Firstly, the implementation of point-of-care clinical decision-making tools and guidelines such as the American College of Radiology (ACR) Appropriateness Criteria are evidence-based means of ensuring appropriate testing and reducing waste at the point of requisition by the ordering provider. The CAR endorses its own top 5 recommendations for reducing low-value imaging and has created referral guidelines for appropriate imaging across several sections such as musculoskeletal, trauma, and breast imaging. 35 Central intake offices are models which pool and streamline advanced imaging referrals across regional facilities, reducing duplicate exams, prolonged waitlists, and transportation to distant sites. Central intake offices present a unique opportunity which can be coupled with clinical decision-making tools and appropriateness guidelines to standardize the provision of medically necessary care. For example, a central intake office is an effective means in which to apply appropriateness guidelines, such as not performing MRI exams for hip and knee pain in adults if severe osteoarthritis is seen on a radiograph, which in one study reduced unnecessary hip and knee MRIs by 21%. 36 A recent review of value-based radiology in Canada outlines strategies to reduce low-value imaging and provides a summary of recommended actions. 35
Appropriate follow-up for incidentally detected findings can help limit the provision of subsequent low value imaging. The ongoing development and implementation of guidelines such as the ACR White Paper on Managing Incidental Thyroid Nodules or the CAR Recommendations for the Management of Incidental Hepatobiliary Findings in Adults are critical to reducing unnecessary extra examinations and each of its downstream effects beyond improving the individual patient’s care.37,38 In concert with reducing waitlists through guidelines, clinical decisions making tools, and central intake offices, advocacy for the provision of adequate imaging capacity and effective imaging efficiency (ie, schedule optimization to reduce scanner idle time between patients) may reduce the burden of delayed medically necessary tests, and thus mitigate more intensive care for sicker patients (compounding the effects as described in framework item 1).
Reduce Environmental Impact of Medically Necessary Care
When imaging examinations are appropriately indicated, it is imperative that each study’s relative environmental impact be considered in part of the clinical decision-making process. In medical education and primary care, there is a growing emphasis on the financial aspects of low-value care such as routine bloodwork. For example, there is increasing acknowledgement of the financial cost of vitamin D testing, which is estimated to be unnecessary in up to 75% of cases and amount to $30 million annually in Canada. 39 As patients and providers become more cognisant of the financial ramifications of medical care, a similar paradigm shift in perspective must be made regarding literacy around healthcare’s climate impact. Leadership by professional medical organizations and policymakers is essential. A recent CAR Statement on Environmental Sustainability in Medical Imaging provides specific recommendations to guide radiologists, medical imaging operations and administrative teams, industry partners, and government in transforming to low carbon, high quality, climate resilient medical imaging in Canada. 40
Mitigation strategies are centred on reducing overall energy consumption and reducing unnecessary waste. As such, the simple yet substantial impact of powering down medical imaging machines when not in use is an ideal mitigation target. 19 The cumulative energy use of medical imaging equipment is considerable, with a single radiology department in Switzerland reporting that the energy consumption of its 3 computed tomography (CT) and 4 magnetic resonance imaging (MRI) machines was equivalent to 4% of the hospital’s total energy use. 41 In other terms, one CT scanner was equivalent to the annual power used by 5 four-person households and one MRI scanner was equivalent to 26 four-person households. 41 Moreover, energy consumption of these machines in standby state accounted for two-thirds of the total CT energy use and one-third of the total MRI energy use. 41 When possible, optimizing low energy idle and system off states, particularly for CT, is of utmost importance and should be an area of focus among radiologists, technologists, and industry partners. A predominantly outpatient practice environment is the optimal scenario for this mitigation strategy, as demonstrated by a recent Canadian study which found that powering down a single CT scanner during non-operational times overnight and on Sundays resulted in annual savings of 14 180 kWh. 42
Beyond the medical imaging scanners themselves, taking advantage of radiology department workstation devices and interventional rooms when non-operational is critical. In a United States study of all workstations in a single radiology department, it was reported that turning off the radiology computers and monitors at the end of a workday and on weekends amounted to a 76% reduction in energy consumption. 43 In another study evaluating the energy use of 32 workstations in a single department, a simple adjustment in device configuration to shut down after 1 hour of inactivity (as opposed to the default of entering a stand-by mode after 4 hours of inactivity) correlated with a 45% reduction in energy use. 44 When interventional radiology suites are not in use, allowing greater fluctuations in temperature and limiting climate control and air change systems can significantly reduce energy consumption.19,45
Addressing Scope 3 (supply chain) emissions in radiology will require transition to a circular economy model. Current linear supply chain procurement involves resource extraction, manufacture, transportation, single use and disposal, creating continuous demand for raw materials and landfill/incineration. In a circular supply chain, products are reused, repurposed, and recycled to next best use, minimizing resource consumption and waste generation. The 5 R’s of waste hierarchy (refuse, reduce, reuse, repurpose, recycle and lastly dispose) place emphasis on waste prevention over disposal.46,47 At the production and packaging steps, switching from single-use to multi-patient CT contrast delivery systems has been shown to reduce contrast waste by 73%, plastic waste by 93%, and cost by 35%. 48 Establishing a circular supply chain is a multi-step and industry collaborative process but can be achieved through examples such as creating contrast medium recycling pathways, switching from disposable to reuseable medical supplies, and optimizing the efficiency of imaging scanners in recapturing finite resources.19,49
When imaging is appropriately indicated, choosing lower-energy imaging tests may provide a similar degree of diagnostic clarity, while potentially reducing carbon emissions by over 17-fold such as in cases of suspected uncomplicated acute cholecystitis or appendicitis in which ultrasound (emitting an average of 0.53 kg CO2 equivalents) may avert the use of a CT scan (emitting an average of 9.2 kg CO2 equivalents). 50 Additionally, abbreviating imaging protocols can lead to substantial reductions in emissions with potential benefits of improved patient experience and reduced waitlist times. For example, using an abbreviated cardiac MRI protocol with a change in the timing of certain sequences after contrast administration leads to savings of 8 minutes per scan and the downstream energy savings equivalent to 27 homes annually if implemented across the United States. 51
Innovative means of providing portable and low-energy imaging can help reduce the climate impact of excessive transportation. In Canada, transportation is responsible for 22% of national GHG emissions, presenting a major sustainable opportunity by optimizing both patient and provider transportation needs. 52 In rural and remote communities of Northern Saskatchewan, the implementation of a remote telerobotic ultrasound program yielded a diagnostic study in 70% of cases, minimizing unnecessary travel, improving wait times, and reducing disparities in imaging accessibility. 53 Furthermore, following the implementation of a low-energy, portable MRI machine (0.064 tesla) in a remote Ontario community, it was found that patient transfer to another centre for fixed MRI examination could be deferred in over half of their cases, correlating to significant mitigation in GHG emissions and approximately $854 841 in savings per 50 patients annually. 54
Lastly, adaptation to the now unavoidable impacts of the climate crisis is essential for all medical imaging departments. Complete description of adaptation measures is beyond the scope of this paper, however, should include backup systems to prevent power and data loss, up to date disaster response protocols, building structural preparedness against floods, extreme heat, and wildfire smoke as well as workforce planning for increased demand and to anticipate healthcare worker shortages. Collaborative action on adaptation measures requires education and engagement of front line radiology team members including radiologists and technologists, facility operations and medical administration, as well as regional, national, and global radiology organizations. A recent statement by the CAR highlights the need to integrate climate change knowledge into the Canadian Radiology educational curricula. 55 Further adaptive efforts should lean heavily into structural preparedness of buildings against natural disasters, developing protocols and back-up systems in the event of disasters or power loss, and applying an iterative approach which assesses and continually improves upon ongoing sustainable initiatives.
Conclusion
Medical imaging plays a considerable role in healthcare’s and the world’s greenhouse gas emission profile. Addressing planetary health in radiology requires significant buy-in from medical imaging departments and key partners. Strategies to mitigate and adapt to climate change impacts should be a central focus to radiologists, technologists, hospital administrators, industry partners, learners, and educators. An overarching framework for practicing sustainable radiology includes reducing the need for resource-intensive care, reducing low value imaging, optimizing energy efficiency, and reducing waste when providing medically necessary care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MB is co-Chair of the CAR Environmental Sustainability Working Group.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.