
Abstract
Introduction
The global population of transgender and gender non-binary (TGNB) individuals is estimated to be up to 25 million people. 1 In the United States (US), a study from 2016 reported that 1.4 million Americans (0.6% of the US population) identify as TGNB, a figure that has doubled in a decade. 2 Despite this, TGNB individuals suffer from inequalities in the provision of healthcare, with a large survey examining the experiences of 27 715 respondents reporting that 28% had postponed medical care even when sick or injured, and one-fifth were refused care because of their gender identity. 3 A survey of more than 6450 TGNB participants found that 28% of respondents were subjected to harassment in medical settings and 50% had to teach their medical providers about transgender care. 4 Radiology departments are not exempt from this, and a recent survey of US breast imaging facilities reported that many do not have the necessary procedures and policies to provide inclusive environments for TGNB patients. 5
The use of gender-inclusive language is at the forefront of ensuring respectful communication and provision of healthcare and imaging. At the individual level, this may take the form of asking for names and pronouns, as experiences of gender affirmation are known to be protective against mental health problems. 6 On the contrary, over 40% of TGNB individuals are reported to have attempted suicide at some point in their lifetimes, with experiences of discrimination or mistreatment in healthcare being a risk factor for suicide thoughts and attempts. 3
At the systems level, terminology such as “women’s imaging” represents a lack of inclusivity to non-binary and transmasculine audiences, yet continues to be used among names of radiology fellowship offerings. The aim of this study was to examine the current landscape of gender-inclusive terminology among radiology fellowship programs and public online profiles of equity, diversity, and inclusion (EDI) among Canadian and US radiology departments and identify areas for improvement.
Methods
We collected and compiled information on all the radiology fellowships offering training in Breast Imaging, Women’s Imaging, Breast and Body Imaging, or similar names in Canada and the US. In the US, fellowship match outcome data from the National Resident Matching Program database was consulted. Canadian fellowships were identified from individual institution websites. After identification of all institutions offering the fellowships of interest, data was collected from each institution’s Department of Radiology academic website. Data collection was from September to October 2021 by three team members (TY, LM, and EC) and reviewed for accuracy and consistency by a single team member (TY). The primary outcome collected from each website was the name of the institution’s fellowship program. “Gender-inclusive” naming was determined as those referring to anatomic body part instead of gender-specific terms (ie, “Breast and Abdominal Imaging” is gender-inclusive, while “Women’s Imaging” is not). Secondary outcomes included the presence of Department of Radiology-specific EDI Committees, EDI Continuing Medical Education (CME) courses, and CME courses about breast, breast and body, or women’s imaging.
Endpoints collected were dichotomous and thus analyzed using the χ2 or Fisher exact test and presented as frequencies with percentages. All analyses were conducted with R version 4.0.5. P-values < .05 were considered statistically significant, and all tests were two-sided. Ethics approval was not required since the study did not include human or animal subjects and the data was collected from publicly available sources. We also applied the “A pRoject Ethics Community Consensus Initiative” (ARECCI) screening tool which scored minimal risk and indicated that our study did not require research ethics board review.
Results
Gender-Inclusive Radiology Fellowship Program Names and EDI Among Publicly Available Websites of Canadian and US Radiology Departments.
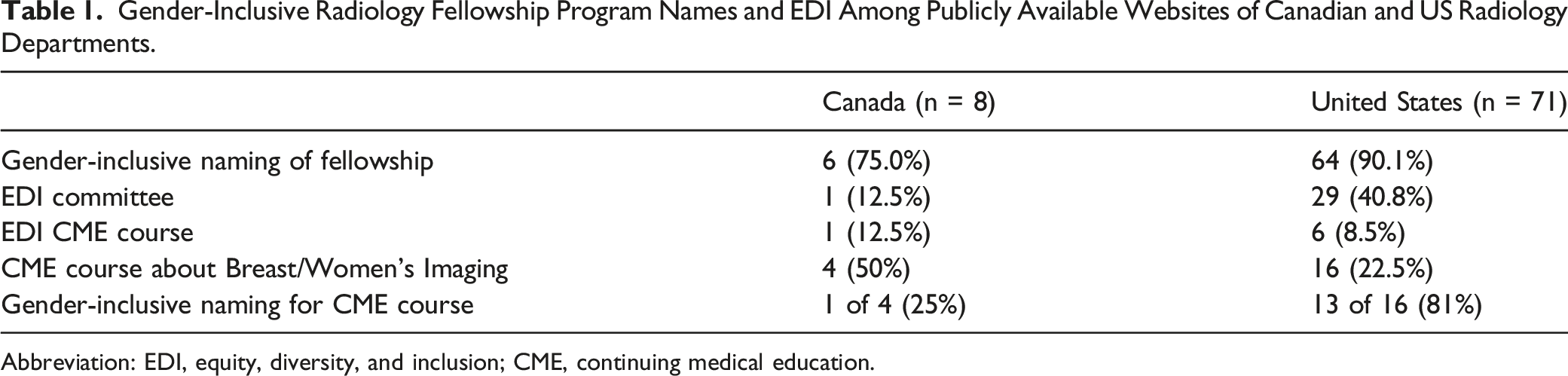
Abbreviation: EDI, equity, diversity, and inclusion; CME, continuing medical education.
Among the Canadian institutions, only one (12.5%) Department of Radiology acknowledged an EDI Committee on its website, compared to 29 (40.8%) US institutions. Radiology CME EDI courses were infrequently found on institution websites in both countries (12.5% in Canada vs 8.5% in the US).
Radiology breast, breast and body, or women’s imaging CME courses were more frequently reported among Canadian institutions (50% in Canada vs 22.5% in the US). Among those identified, 1 of 4 (25%) Canadian and 13 of 16 (81%) US CME courses used gender-inclusive terminology. Examples of CME course names that were not gender-inclusive included the “Annual Women’s Imaging Conference” and “Women’s Health: Imaging and Treatment Guidelines for Primary Care Providers”.
Correlation Between Gender-Inclusive Radiology Fellowship Program Names and Other EDI and CME Data Among Canadian Institutions.
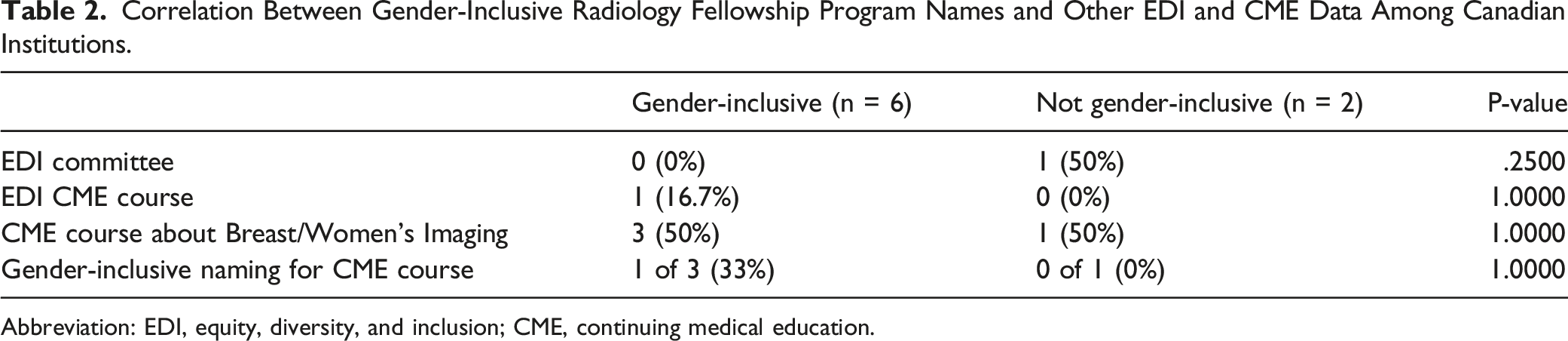
Abbreviation: EDI, equity, diversity, and inclusion; CME, continuing medical education.
Correlation Between Gender-Inclusive Radiology Fellowship Program Names and Other EDI and CME Data Among US Institutions.
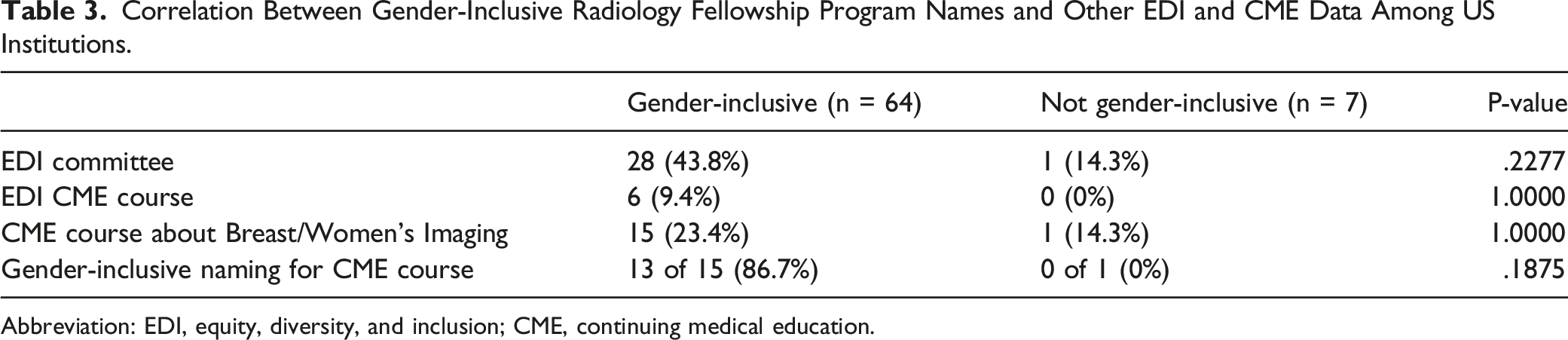
Abbreviation: EDI, equity, diversity, and inclusion; CME, continuing medical education.
Discussion
In 2015, a paper in the American College of Radiology Bulletin called to action the need for gender-affirming environments among radiology departments. 7 Despite this, the radiology literature is lacking on topics of TGNB health compared to other medical disciplines. 8 The current landscape of radiology literature continues to be limited by the outdated use of binary gender data which fails to encompass the broad spectrum of TGNB radiologists and trainees. 9 The available research on TGNB patient experiences shows room for improvement in fostering TGNB culturally competent care in radiology. 10 In a survey of 363 TGNB patients, more than 70% reported having had a negative encounter at an imaging center including use of inappropriate pronouns, being misgendered in the radiology report, and voicing concern that personnel were uncomfortable caring for a TGNB patient. 10
Our study quantified the use of gender-inclusive language among radiology departments in the US and Canada, with 75% of Canadian institutions and over 90% of US institutions having gender-inclusive radiology fellowship program names. We additionally took stock of radiology departments’ online EDI presence through the existence of publicly acknowledged EDI committees and CME courses. Despite the high number of gender-inclusive named fellowship programs, many of these institutions do not have an EDI committee listed on their website. Interestingly, the one Canadian institution that had an EDI committee referred to their fellowship as “Women’s Imaging”. However, this institution has expressed interest in changing the fellowship’s name to adopt more inclusive language after noticing advocacy efforts from organizations such as Canadian Radiology Women. When radiology departments do rename their fellowship programs to have gender-inclusive wording, we encourage them to share the reasons why they changed and to advocate for more widespread change.
In the US, there was a noticeable trend toward institutions with gender-inclusive fellowship names to also have EDI committees and gender-inclusive CME course names. However, the small number of US institutions that has yet to adopt gender-inclusive fellowship program names limits the statistical power of our comparison. Compared to their Canadian counterparts, there was a trend toward US institutions having a greater proportion of gender-inclusive names for breast, breast and body, or women’s imaging CME courses. Renaming a CME course with more inclusive language can be as simple as changing from “Women’s Imaging” to “Breast, Obstetrical, and Gynaecological Imaging”, as done by the one Canadian institution identified to have a CME course with gender-inclusive naming.
Using gender-inclusive names for fellowship programs and CME courses, as well as creating EDI committees and courses are just some of the steps in acknowledging the diversity of individuals in radiology and the patient populations we serve. Cultural competency starts during medical and radiography education, in which more than 70% of radiography educators indicated the importance of TGNB topics in the teaching curriculum to be moderate or extreme, but felt limited in their preparedness to teach these imaging considerations. 11 In a 2011 study of undergraduate medical schools in the US and Canada, the median reported time dedicated to teaching lesbian, gay, bisexual, and transgender (LGBT) related content in the entire curriculum was only 5 hours. 12 This highlights the importance of transgender sensitivity training, basics of transgender health, and imaging manifestations of gender-affirming care in fostering a truly educated radiology department about the needs of TGNB patients. Furthermore, policies and procedures including asking about gender identity, names, and pronouns on intake forms, offering gender-inclusive restrooms and dressing rooms, redesigning facilities to avoid gender-connoting color schemes or signage, and publicly displaying non-discriminatory policies and reading materials can help promote a safe environment.8,13
We believe our data will serve as a road map for institutions to take steps in creating inclusive environments in radiology for TGNB individuals. Furthermore, despite an institution being accounted for in our data as having an EDI committee or CME course, there were several instances in which this information could only be found after a prolonged and extensive search by the investigators. Our data highlights the importance of radiology departments showcasing their EDI committees and CME courses on their websites, as an institution’s public presence is foundational to the education of providers and making patients feel welcome. 14 Of note, there were numerous cases of institutions having general EDI committees but not radiology-specific EDI committees. We urge institutions to consider creation of an EDI committee at the department of radiology level, as the radiographic needs of TGNB individuals may be missed by the overarching goals of an institution-wide committee. To successfully bring about change, commitment from departmental leadership is paramount in making diversity a priority and this can be exemplified by the creation of a radiology-specific EDI committee. 15
Our study is not without its share of limitations. First, all data collected was from publicly available websites made by each institution. We may have underestimated the true number of EDI committees and CME courses offered by each radiology department. However, this is a central message of our study, which wishes to highlight only those that are publicly visible and encourage institutions to showcase their pledge to EDI through a public online presence. It is important to note that the websites reviewed in our study are those of the academic universities and not the hospitals, which one may argue could have less of an effect on patients as they are not the usual target audience for academic websites. One such way of promoting a greater impact among patients is for EDI content to be displayed through hospital websites too. Nevertheless, it is known that transgender stigma operates at multiple levels (i.e., individual, interpersonal, and structural), and that while the implementation of gender-inclusive fellowship names and CME courses on academic platforms is seemingly not directly visible to patients, it is these policies and practices that help to lessen the burden of structural stigma toward TGNB individuals. 16
Lastly, the lack of specificity in fellowship program names may limit our study in identifying appropriate gender-inclusive terminology. For example, a “women’s and breast imaging” fellowship may truly reflect a difference in content from “breast and abdominal imaging”, which in fact may be more aptly named “breast, obstetrical, and gynaecological imaging”. We urge for institutions to be appropriately specific when considering renaming fellowships and CME courses with gender-inclusive language.
Conclusion
Utilizing gender-inclusive language and terminology is a first step in providing a more welcoming and inclusive environment for TGNB patients and healthcare providers. Gender-inclusive language is used in the names of most radiology fellowship programs in Canada and the US. Where many radiology departments fall short is the lack of EDI committees and CME courses. Canadian institutions in particular can make a greater effort to use inclusive language in breast and body imaging CME courses. Radiology departments should publicly showcase their commitment to EDI on their websites. It is the responsibility of institutions and individuals to educate themselves about transgender health and to make changes toward inclusive environments for improved patient care and healthcare worker mental health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Faisal Khosa is the recipient of the American College of Radiology—Global Humanitarian Award (2021). This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.