
Abstract
Objective:
Victims of child sexual abuse (CSA) present with a higher risk of psychotic disorders. However, the developmental course of psychosis following CSA, such as the age at onset, remains unknown. This study aimed to determine whether the age at onset of psychotic disorders was influenced by sexual abuse, sex, and confounding factors (substance misuse, intellectual disability, and socioeconomic status).
Method:
A prospective matched-cohort design was used, with administrative databases from a child protection agency (CPA) and a public health system. Children who received a substantiated report of CSA at the CPA and whose health data could be retrieved were selected (n = 882) and matched with children from the general population using their date of birth, sex, and geographical area. Survival analysis was performed to estimate the association between sexual abuse, sex, and confounding factors and the age at onset of psychotic disorders.
Results:
Sexual abuse and substance misuse are significantly associated with the age at onset of psychotic disorders. In the sexually abused group, only substance misuse is associated with the age at onset of psychotic disorders, but this was not significant for the general population.
Conclusions:
These findings highlight the importance of prevention of psychotic disorders among sexually abused youth, especially those with a substance misuse diagnosis.
Introduction
Accumulating evidence over the past 15 years revealed a robust relationship between child sexual abuse (CSA) and psychosis. According to a recent meta-analysis, individuals with a diagnosis of psychotic disorder are more than twice (2.38) as likely than the general population to report CSA. 1 Also, a study using a prospective design revealed that sexually abused youth are up to 10 times more likely than the general population to receive a diagnosis of psychotic disorder. 2 Furthermore, up to 40% of individuals with a psychotic disorder have been sexually abused in their childhood, 3 –5 which is more than thrice than the worldwide prevalence of CSA (12.7%). 6
A history of sexual abuse is also an aggravating factor for individuals with psychotic disorders. A study found that for those who report a CSA, there was a larger impairment of social functioning before the first psychotic episode. This impairment was more severe when the sexual abuse occurred prior to the age of 12 years. 7 Another study reported that patients with a child maltreatment history, including CSA, received a diagnosis of schizophrenia on average 4 years earlier than patients who didn’t report maltreatment. 8 Other studies also reported an earlier onset of psychotic disorders among individuals who reported childhood trauma or CSA in comparison to those without a history of trauma. 5,9
Younger age of onset of psychotic disorder has been linked with worse illness course including more severe symptoms and impaired cognitive functioning. A systematic review revealed that early onset schizophrenia is associated with a poorer general functioning (psychological, social, and occupational) than later onset schizophrenia. 10 Furthermore, a meta-analysis uncovered that youth onset (childhood or adolescence) schizophrenia is associated with large deficits on almost all cognitive measures including arithmetic, executive function, IQ, psychomotor speed of processing, and verbal memory. 11 A recent study also identified that early onset of psychotic disorders was associated with prefrontal cortical dysfunction. 12 Finally, Van der Werf and colleagues 13 found that early onset of a psychotic disorder was associated with more negative symptoms, higher antipsychotic dosage, impairments in memory and attention, as well as with a diagnosis of schizophrenia.
Besides CSA, other factors have been associated with an earlier age at onset of psychotic disorders. A meta-analysis revealed that substance use, other than alcohol, is associated with an earlier age at onset of psychosis. 14 When compared to nonusers, the age at onset was 2.7 years earlier for cannabis users and 2 years earlier for substance use in general. Male sex is also associated with an earlier onset, 10,13 men generally having their first episode 3 to 4 years earlier than women. 15 Those variables need to be considered when assessing the developmental trajectories of psychotic disorders in sexually abused youth.
Although providing important information on the association between CSA and the course of psychotic disorders, previous studies relied mostly on retrospective designs and didn’t controlled for other factors associated with an earlier onset, such as substance use 14 or for factors associated with a higher risk of CSA (e.g., intellectual disability and socioeconomic status). 16,17 Such information would inform mental health prevention strategies and programs among sexually abused youths. There are clear clinical and economic benefits in offering early intervention for people at risk of developing psychotic disorders. 18
This study used a prospective matched-cohort design to clarify the developmental trajectory, in terms of age of onset of psychotic disorders among sexually abused youths. Specifically, this study aimed to determine whether the age at onset of psychotic disorders was influenced by CSA, sex, and potential confounding factors such as substance misuse, intellectual disability, and socioeconomic status. We expected that sexually abused youth would have a higher risk to receive their first psychotic disorder diagnosis at an earlier age when compared to the general population. Also, we expected that male sex and substance misuse would be associated with a higher risk of an earlier onset of psychotic disorders.
Methods
As mentioned previously, 2 this study was part of a larger project in which administrative databases from a child protection agency (CPA) and public healthcare system in a large Canadian city were linked. A prospective matched-control cohort design was used. Certificates of conformity or authorizations to obtain confidential information from administrative databases were obtained from the ethics committee of the CPA, the Information Access Committee, the public health insurance agency, and Université de Montréal. The requirement for consent was waved as the data were taken from existing databases.
Procedures
All children younger than 18 years who received a substantiated report of sexual abuse at a CPA in a large Canadian city between January 1, 2001, and December 31, 2010, were selected for the study (N = 955). Personal data from the CPA database were matched with data from the public health agency for 92% of the selected children (n = 882) using their health insurance number or their surname, name, complete address, and date of birth. In Quebec, the public healthcare system covers Canadian citizens residing in the province, foreign nationals authorized to stay within the province for more than 6 months and their accompanying spouses and children. Thus, it was more probable that unmatched data were due to misspelling of personal information rather than because the participants were not covered by the public healthcare system.
Each of the 882 sexually abused participants was matched to another child from the public health agency according to the following criteria: (a) year and month of birth, (b) sex, and (c) geographical area served by the CPA. Children in the general population group were not included in the sexually abused group and did not have any substantiated reports of sexual abuse between 2001 and 2010 from the participating CPA.
Participants
The final sample comprised 882 youth with a substantiated report of sexual abuse and 882 matched youth from the general population. There were 661 girls (75%) and 221 boys (25%) in each group. As described elsewhere, 2 participants’ average age was 11.11 years (standard deviation [SD] = 4.18 years, range = 1 to 18 years) at the time of the first substantiated report of sexual abuse (study entry) and 18.95 years (SD = 4.71 years, range = 7 to 29 years) at the end of the data extraction period. The moment of study entry corresponds to the date when the report of sexual abuse was corroborated by CPA services, meaning that there was sufficient evidence that the abuse has occurred. As reported previously, 19 boys were significantly younger than girls by almost 1.5 years at the time of report. For the majority of the sexually abused group, sexual abuse (88%) was their first substantiated report at the CPA. Other substantiated reports included neglect (30%), physical abuse (10%), behavioral problems (8%), and abandonment (2%). The majority of the sample was involved in a judicial process (84%). Many were placed out of home (24%) or entrusted to a distant family member (10%).
Measures
Sexual abuse
Sexual abuse is defined as any gesture of a sexual nature, with or without physical contact, committed without consent, or through emotional manipulation or blackmail. 20 In Canada, when sexual abuse is reported to the Director of Youth Protection, a CPA worker conducts a summary analysis of the situation and decides whether the report should be retained for evaluation. If the report is retained for evaluation, a social worker evaluates the situation and makes a clinical judgment regarding the level of corroboration of the abuse. 20 Participants in the sexually abused group were those whose report was substantiated, meaning there was sufficient evidence that sexual abuse had occurred.
Psychotic disorders
In this study, psychotic disorders refer to all diagnoses of psychosis, including mood disorders with psychotic features and substance-related psychosis. Included diagnostic categories from the International Classification of Diseases Tenth Revision 21 were schizophrenia, schizotypal, and delusional disorders (F20 to F29), mood (affective) disorders (F30 to F39) with the psychotic symptoms specifier (.2, .3, or .5), and mental and behavioral disorders due to psychoactive substance use (F10 to F19) with the psychotic disorder specifier (.5). All documented diagnoses from the preceding categories made during medical consultations or hospitalizations were obtained from the public health insurance agency (outpatient services) and Ministry of Health (inpatient services) databases between January 1, 1996, and March 31, 2013.
Confounding factors
The socioeconomic level of participants at the time of the first substantiated report of sexual abuse was estimated via postal codes, using a material and social deprivation index, 22 which was controlled for in all analyses because of its potential link with socioeconomic status and psychotic disorders. 16 Also, the diagnoses of intellectual disability and substance misuse before the first diagnosis of a psychotic disorder were used as control variables because of their potential link with sexual abuse and psychotic disorders. 14,17 The pairing index was controlled for when comparing groups. For within-groups analysis, the age at the time of the first substantiated report of sexual abuse was controlled for.
Statistical analysis
A multivariate analysis of variance was conducted to calculate the observed and adjusted means for the age at the first diagnosis of psychotic disorders. Survival analysis using Cox regression models 23 was performed to determine whether group and sex were associated with the age at onset of psychotic disorders. First, the hazard rates of the abused and general population group on the age at onset of psychotic disorders were estimated. Second, we conducted the analysis separately for the sexual abuse and general population groups to estimate the hazard rates of the effect of sex on age at onset of psychotic disorders (group-stratified analysis). Confounding factors described in the previous section were controlled for in all analyses. Analyses were conducted using IBM SPSS version 24, with a 5% significance level.
Results
Sample Description
In the abused group, 5.2% of participants received a diagnosis of a psychotic disorder during the period studied. Most of them received their first diagnosis after a substantiated report of sexual abuse (76%). The prevalence of psychotic disorders in the general population group was 1%. In the sexually abused group, 4% of the participants with a psychotic disorder received a diagnosis for an intellectual disability before receiving a first diagnosis for a psychotic disorder, and 15.2% received a diagnosis of substance misuse prior to an initial diagnosis of a psychotic disorder. None of the participants from the general population group received a diagnosis for either intellectual disability or substance misuse prior to receiving a diagnosis of psychotic disorder.
Observed and Adjusted Means
Table 1 presents the observed and adjusted means for the age at the first diagnosis of psychotic disorder by group and sex. Those means are presented in a descriptive way and do not enable us to conclude to a difference between groups; the Cox regression models presented in sections “Childhood Sexual Abuse and the Age at Onset of Psychotic Disorders” and “Sex Effect According to Groups and the Age at Onset of Psychotic Disorders (Group-Stratified Analysis)” tested group and sex effects. The observed means are unadjusted, while the adjusted means take into account the pairing index, substance use, intellectual disability, and socioeconomic status. As shown in Table 1, the unadjusted mean age at onset appears slightly higher for the sexually abused group; however, this is not the case for the adjusted means. This could be explained by the fact that the pairing index takes into account the number of years of data we have per participant and the age at study entry.
Age at First Psychotic Disorder Diagnosis by Group.

a Means are adjusted for the following covariables: substance use, socioeconomic status, intellectual disability, and pairing index.
Childhood Sexual Abuse and the Age at Onset of Psychotic Disorders
The first Cox regression model (model 1) included all participants. While controlling for socioeconomic status, substance use, intellectual disability, and pairing index, factors significantly associated with the age at onset of psychotic disorders were sexual abuse and having received a diagnosis of substance misuse prior to the first psychotic disorder diagnosis. The relationship was negatively correlated for sexual abuse and for substance use, which means that participants with a corroborated report of sexual abuse and those with a diagnosis of substance seem to receive their first diagnosis of psychosis earlier. Hazard ratios are presented in Table 2, and the survival curve is presented in Figure 1.
Cox Regression Analyses.
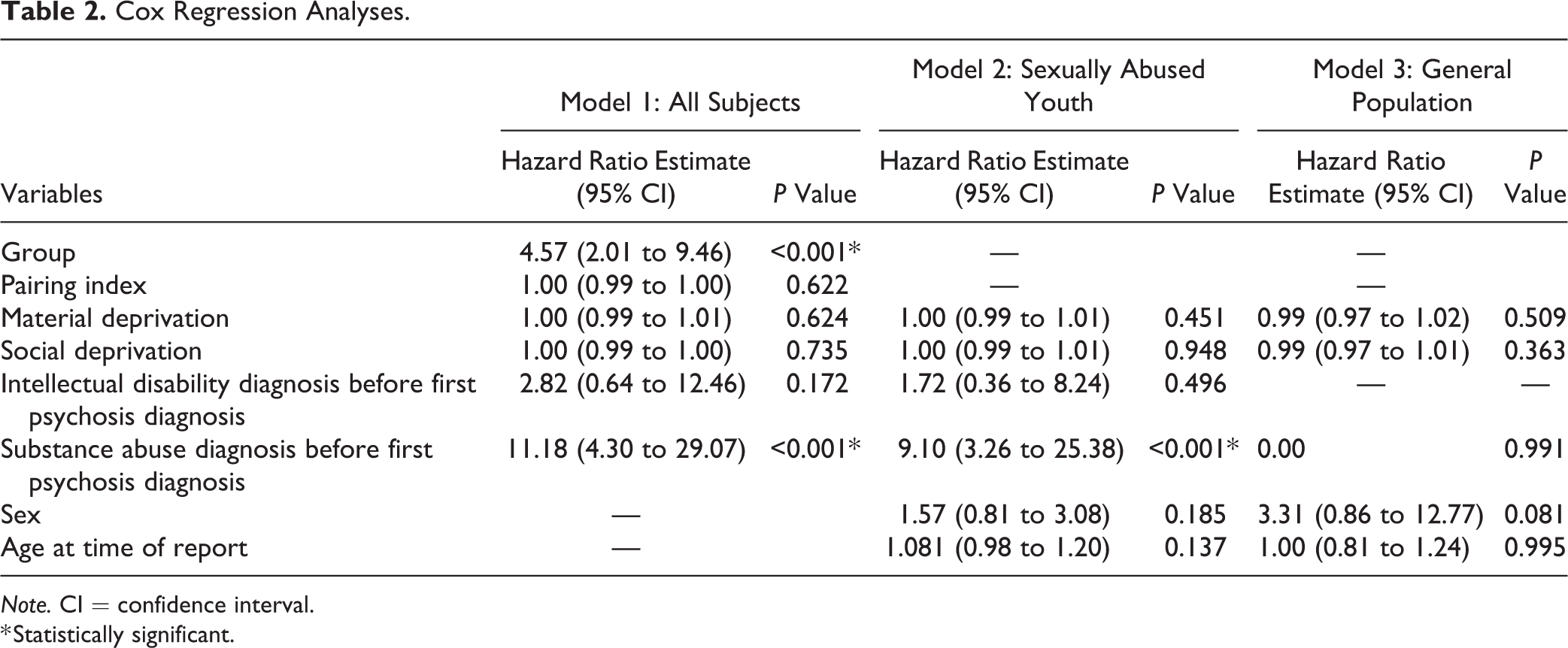
Note. CI = confidence interval.
* Statistically significant.
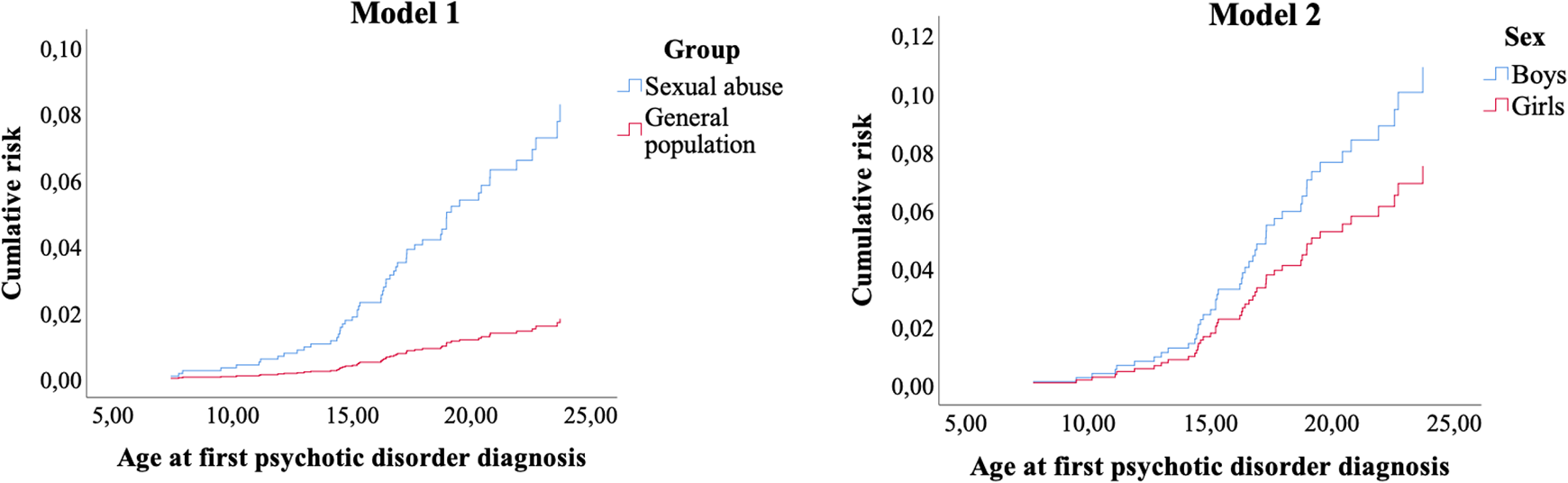
Age at onset of psychotic disorders by group and sex.
Sex Effect According to Groups and the Age at Onset of Psychotic Disorders (Group-Stratified Analysis)
To assess sex effect according to group within the present matched study design, stratified analyses were realized using Cox regression models. Model 2 compared sex within the sexually abused group and is presented in Table 2 and Figure 1. When comparing sexually abused boys with sexually abused girls, while controlling for socioeconomic status, intellectual disability, substance use, and the age at the time of the first substantiated report of sexual abuse, the only variable associated with the age at onset of psychotic disorders was having received a diagnosis of substance misuse before the diagnosis of psychotic disorder. The relationship was negatively correlated, meaning that those with a substance use diagnosis seem to receive their first diagnosis of psychosis earlier than those who didn’t receive that diagnosis. The same analysis conducted with the general population group (model 3) was not significant (see Table 2 for hazard ratios).
Discussion
Consistent with our hypotheses, having received a substantiated report of sexual abuse during childhood and substance misuse disorder were factors that were associated with the age at the first diagnosis of psychotic disorder while controlling for socioeconomic status, intellectual disability, substance use, and the pairing index. However, the hypothesis that sex would be associated with the age at onset wasn’t supported in neither group. This is the first study to assess the age at onset of psychotic disorders in sexually abused youth using a prospective matched-cohort design.
Results revealed that CSA is associated with the age at onset of psychotic disorders when compared to a matched sample from the general population, while controlling for confounding factors. This confirms the findings from previous studies that assessed sexual and childhood trauma in groups of patients with psychotic disorders. 5,8,9 Similarly, having received a diagnosis of substance misuse, also stressor and risk factor for psychosis, was negatively associated with the age at onset. This is consistent with results from a meta-analysis, which revealed that patients with a psychotic disorder who had a substance abuse diagnosis or clinically significant substance use presented with an earlier onset when compared to patients with the same diagnosis who were nonusers. 14
In this study, sexual abuse was significant in an integrated model with substance misuse, which was also significant, meaning that sexual abuse is a critical risk factor for the age at onset of psychotic disorder above and beyond substance misuse. However, because we considered all diagnoses of psychotic disorders and not only those that occurred after the substantiated report of sexual abuse, this result might have two possible meanings. First, sexual abuse could lead to an earlier onset of psychotic disorders. 24 Second, individuals with psychotic disorders might present with a greater risk to suffer from victimization, thus being more at risk of sexual abuse. 24 Nonetheless, because most of our participants received their psychotic disorder diagnosis after the substantiated report of sexual abuse (almost 70%), the first hypothesis seems more plausible.
Youths with a substantiated report of sexual abuse might present a higher risk to receive their first diagnosis of psychotic disorder earlier than youth from the general population because of the specific impact of CSA on the brain. As suggested by Van Os and collegues, 25 environmental stressors such as early life adversity, growing up in an urban environment, being in a minority group, and cannabis use have specific impact on the brain during sensitive developmental periods. Thus, trauma occurring prior to 18 years might impact brain development such as neuro- and social cognition.
Furthermore, this study found no association between sex and age at onset and thus couldn’t confirm that men present with an earlier onset of psychotic disorders than women. 10,13 It is possible that the fact that boys were significantly younger than girls at the study entry prevented us from identifying all those who developed a psychotic disorder and that some participants may develop a psychotic disorder later on. Participants were 19 years old on average by the end of the study period, while psychotic disorders generally develop between 15 and 30 years of age. 26 Also, previous studies that found an earlier onset of psychotic disorders in men used larger samples of individuals with a psychotic disorders. 10,13 In the present study, 3% of the total sample received a diagnosis of psychotic disorder. This might constitute too small a subsample to enable us to observe the trends generally observed in other studies.
Strengths and Limitations
The use of administrative health data limited the investigation of psychotic disorders and substance misuse to youths who received such diagnoses. Thus, it is possible that other participants used substances or had psychotic symptoms in a nonclinically significant way or without the situation being noticed by their physician. Another limitation is the fact that there were few cases of psychotic disorders in the general population group, although this prevalence represents what is normally found in the general population. 27 This limited the final sample of participants of the general population group who received a psychotic disorder diagnosis and therefore increased the risk of type 2 error. In future studies, these results should be replicated with a larger sample of youth from the general population with a psychotic disorder diagnosis. Furthermore, the average age of participants at the end of our study (19 years) was lower than the median age for a first psychotic episode (21 to 23 years). 28 –30 Thus, it is reasonable to think that a significant number of psychotic disorders have yet to develop in this sample. Many participants may not have developed a first psychotic episode by the end of data extraction, which means that our data are limited to early onset psychotic disorders on average. Finally, because sexually abused youth were from a CPA, our results are specific to a subpopulation that presents more severe abuses and represents only 10% of victims of childhood maltreatment in Canada. 31 Hence, it is possible that some youth from the general population experienced sexual abuse without the situation being reported to the Director of Youth Protection or substantiated. The difference between both groups might then be minimized by this study’s design.
The use of a longitudinal matched-cohort design allowed us to identify the sequence in which variables of interest occurred, thus enabling us to perform survival analyses. Survival analysis is in itself a strength of the study as it considers time and the sequence between psychotic disorders and sexual abuse, which is important when investigating the age of onset. Also, administrative health data made it possible to identify all the diagnoses of psychotic disorders and substance misuse that occurred for our participants during the study period. Lastly, another strength is the inclusion of mood disorders with psychotic symptoms and substance-induced psychosis in the study. Previous studies didn’t include these diagnoses and may have underestimated the prevalence of psychotic symptoms and the risk of developing a psychotic disorder following CSA. Their inclusion can contribute to shed light on the common sexual trauma etiology of psychotic symptoms in different mental health disorders. 9,32
Implications and Future Research
These results highlight the importance of targeted prevention of psychotic disorders in sexually abused youth, especially among those who received a diagnosis of substance misuse. Health practitioners should pay particular attention to youth who are more vulnerable to psychotic disorders, such as those with a family history of psychosis, who are socially isolated or using drugs. 16,33,34 This could enable prevention programs to target individuals at high risk of psychosis and also decrease the duration of untreated psychosis, which is known to negatively influence the course of psychotic disorders. 35 This could also reduce the negative consequences of early onset psychosis, which tends to be associated with a more severe and chronic prognosis as well as worse cognitive impairment than later onset psychosis. 10 –13
Patients with co-occurring psychotic disorders and trauma-related symptoms due to child abuse represent a clinically distinct group and, therefore, need appropriate interventions. 36 Trauma-focused psychological interventions such as cognitive behavioral therapy and prolonged exposition were found to be effective in individuals with psychosis, reducing positive symptoms, delusions, and post-traumatic symptoms. 37,38 Acceptance and commitment therapy was also identified as a promising intervention for individuals with both psychosis and a history of trauma, reducing psychotic and anxiety symptoms and improving emotional regulation. 39 Although more studies are needed, especially for interventions targeted at the prevention of psychosis in sexually abused youth, psychological interventions seem promising in treating individuals with psychosis and childhood trauma.
Conclusions
This study found that sexual abuse and substance misuse were significantly and negatively associated to the age at onset of psychotic disorder. This suggests that sexually abused youth receive their first diagnosis earlier than the general population, especially when there is a substance misuse diagnosis. Future studies are needed to understand the mechanisms implied in the development of psychotic disorders in this population.
Footnotes
Authors’ Note
The views expressed in this study are those of the authors and do not necessarily represent those of the Ministry of Justice. The funding sources were not involved in the study design, analyses, writing, or decision to submit the manuscript for publication. It is impossible for the authors to make the data from this study available, as it would violate the ethical authorizations obtained for this study. The authorizations obtained from the Centre jeunesse de Québec—Institut Universitaire and from the Commission d’accès à l’information du Québec strictly prohibit the diffusion of this data, as they are extracted from personal databases both from the youth protection system and the public health system. Only the authors and the other persons who received the ethical authorizations from those institutions can access the data.
Acknowledgment
The authors wish to thank Denis Lacerte of the Quebec City Youth Centre for his advice in planning this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Canadian Institute of Health Research (no. GSD-157954), the Ministry of Justice’s Victims of Crime Emergency Fund (no. 126489), the Interdisciplinary Research Centre on Intimate Relationship Problems and Sexual Abuse (Centre de recherche interdisciplinaire sur les problèmes conjugaux et les agressions sexuelles; no. 2015-RG-178804), and Team Sexual Violence and Health (Équipe violence sexuelle et santé; no. 2012-SE-144392).