
Abstract
Introduction
The experience of an acute psychotic episode and its treatment for the first time, can be so traumatic that up to one in two people report post-traumatic symptoms or disorder as a consequence (Jackson et al., 2004; McGorry et al., 1991; Mueser et al., 2010; Tarrier et al., 2007). People with first-episode psychosis (FEP) also report traumas in childhood at high rates (Bendall et al., 2008; Conus et al., 2010; Greenfield et al., 1994; Neria et al., 2002; Ucok and Bikmaz, 2007). The presence of post-traumatic symptoms, either childhood or psychosis-related, contribute to a raft of negative outcomes in psychosis, including more severe depression, anxiety, and substance abuse, increased suicidality and reduced treatment adherence, which greatly impede recovery from psychotic disorder (Mueser et al., 2010; Schenkel et al., 2005). Post-traumatic symptoms are responsive to treatment and are beginning to be targeted in the treatment of FEP (Bernard et al., 2006; Jackson et al., 2009). However, little is known about the relationship between childhood trauma-related and post-psychotic post-traumatic stress disorder (PTSD) in FEP, with only one study tentatively suggesting a relationship (Mueser et al., 2010). A relationship between childhood trauma, childhood trauma-related PTSD and post-psychotic PTSD may be due to the experience of childhood trauma and related PTSD, sensitising individuals to PTSD in response to subsequent traumas (Ehlers and Clark, 2000). Alternatively, it is possible that childhood trauma and concomitant PTSD cause more severe acute psychosis (Lysaker et al., 2005), which is more traumatic due to its greater severity. As such, the aim of the current study was to test the following hypotheses:
that those who reported childhood trauma were at greater risk of developing PTSD in response to acute FEP than those without childhood trauma;
that those with childhood trauma-related PTSD had a greater risk of PTSD in response to acute FEP than those without childhood trauma-related PTSD; and
that the relationship between childhood trauma and childhood trauma-related PTSD, and post-psychosis PTSD was not explained by illness-related factors such as duration of untreated psychosis (DUP), severity of psychosis symptoms, and age of onset of psychosis.
Materials and methods
Participants
The study was conducted at the early psychosis services, within Orygen Youth Health (OYH) and Eastern Health Mental Health Services (EHMHS), Melbourne, Australia between February 2007 and February 2008. These programmes provide specialised early psychosis services within the public mental heath service to the Western and Eastern metropolitan areas of Melbourne, respectively. Both services provide inpatient services, medical follow-up, and intensive outpatient case management for young people with early psychosis between the ages of 15 and either 25 (OYH) or 29 (EHMHS) years. Inclusion criteria for the study were being aged between 15 and 29 years; within 18 months of first treatment for FEP; fluent in English; and able to provide consent for participation in the study. Participants were excluded if they were assessed as having an intellectual disability by their case manager, showed evidence of an organic brain disease, or were assessed as experiencing childhood trauma after the onset of psychosis. All participants were recruited when they were receiving outpatient case management. Case managers referred young people to the study. Sixty participants were referred to the study by their case managers: 14 refused to participate, 10 were excluded (two due to poor English, two because they did not receive a DSM psychosis diagnosis during the research assessment, two because their childhood trauma occurred after the onset of psychosis and four because they were unwilling or unable to complete the trauma and PTSD questionnaires during the assessment). Thirty-six participants completed assessments and were included in the study.
The mean age of the group was 21.42 years (SD = 3.43) and the mean time in treatment was 9.81 months (SD = 7.33). Fourteen participants were female (39%) and four were born outside Australia (11%). The majority of people received a diagnosis (based on the SCID, see below) of schizophrenia (n = 16, 44%) or schizophreniform disorder (n = 6, 17%). Other diagnoses received were bipolar disorder (n = 8, 22%), depression with psychotic features (n = 4, 11%), psychosis not otherwise specified (n = 1, 3%) and schizoaffective disorder (n = 1, 3%).
The study was part of a larger investigation of cognition and childhood trauma in FEP (Bendall et al., 2011). Ethical approval was received from the Melbourne Health Mental Health Research and Ethics Committee, the Eastern Health Ethics Committee, and the University of Melbourne Ethics Committee. Each participant received written information about the study and gave written consent to participate in it.
Measures
All measures were administered in one 1.5 hour clinical interview by a clinical psychologist (SB). The Structured Clinical Interview for DSM-IV-TR Axis I Disorders (First et al., 2001) was used to establish the primary psychosis diagnosis. The Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987) measured severity of psychotic symptoms. The presence of childhood trauma was measured by the Childhood Trauma Questionnaire (CTQ) (Bernstein et al., 1997). Childhood trauma was classified as present if participants scored in the moderate or severe range in any of the emotional, physical or sexual abuse subscales. All participants completed the Impact of Events Scale - Revised (IES-R) (Weiss and Marmar, 1997), a questionnaire that measures the three domains (intrusions, avoidance and hyperarousal) of PTSD and is rated in relation to a specific traumatic event. All participants rated the IES-R in relation to their experience of acute psychosis. Those participants who reported childhood trauma (based on the CTQ) also completed an IES-R for the most severe childhood trauma reported. The IES-R cut-off score of 33 was used to estimate the presence of PTSD (Creamer et al., 2003). As a full diagnostic interview for PTSD was not undertaken, we were not able to confirm a diagnosis of PTSD but only that participants reported PTSD symptoms at a clinical level or not. For clarity, we will describe participants as having or not having PTSD throughout the paper when in fact they have self-reported PTSD symptoms at a clinical level.
Analysis
The association between childhood trauma, childhood trauma-related PTSD, duration of untreated psychosis, age of onset and psychosis symptom severity, and post- psychotic PTSD was first examined via a series of univariate logistic regression models. Those illness-related variables associated with post-psychotic PTSD at an a priori set p-value of 0.15 were subsequently retained for the multivariate analysis to assess the strength of the association after controlling for potential confounders. Childhood trauma and childhood trauma-related PTSD were not included in multivariate models together due to high correlation (r = 0.62). DUP was log transformed to rectify skewness.
Results
Thirty-six participants completed measures of childhood trauma and PTSD. Seventeen (47%; 95% CI 31–64%) participants were estimated to have post-psychotic PTSD. Twenty-three participants (64%; 95% CI 48–80%) identified some kind of childhood trauma, of which 12 (33%) endorsed sexual abuse, 13 (36%) endorsed physical abuse and 16 (44%) endorsed emotional abuse. Most of those reporting childhood trauma reported experiencing more than one type of trauma, with seven participants (19%) reporting two, and eight participants (22%) reporting three types of trauma. Fourteen participants (39%; 95% CI 23–55%) reported childhood trauma-related PTSD symptoms at clinical levels.
The relationship between post-psychotic PTSD, childhood trauma and childhood trauma-related PTSD
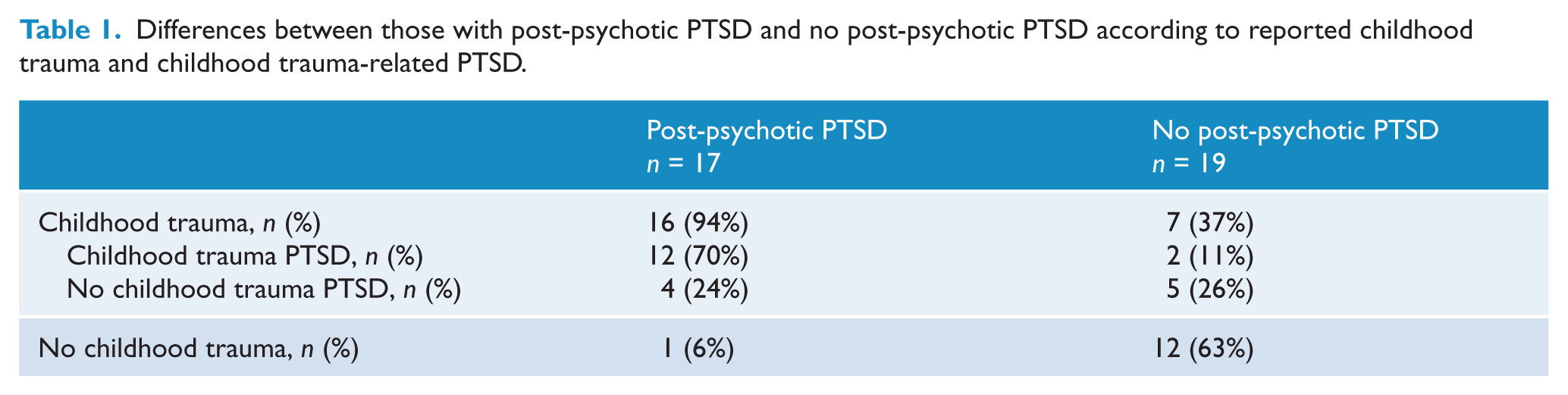
Table 1 shows the numbers and proportions of people with and without childhood trauma, childhood trauma-related PTSD and post-psychotic PTSD. Six percent (n = 1; 95% CI 3–8%) of those who were estimated to have post-psychotic PTSD did not report childhood trauma.
Differences between those with post-psychotic PTSD and no post-psychotic PTSD according to reported childhood trauma and childhood trauma-related PTSD.
Childhood trauma and risk for post-psychotic PTSD
Participants who reported childhood trauma were 27.43 times more likely to report clinical level PTSD symptoms as a consequence of their experience of acute psychosis compared with those who did not report childhood trauma (95% CI 2.96–253.80, p = 0.01; r2 = 0.44).
Childhood trauma-related PTSD and risk for post-psychotic PTSD
People with PTSD related to their childhood trauma were 20.40 times more likely to report PTSD related to their experience of acute psychosis (95% CI 3.38–123.25, p = 0.01; r2 = 0.45) than those who did not report childhood trauma-related PTSD.
The influence of illness-related factors
DUP (OR = 0.72; 95% CI 0.33–1.56, p = 0.41) and age of onset (OR = 1.00; 95% CI 0.86–1.17, p = 0.98) did not significantly predict post-psychotic PTSD. The proportion of variance explained by these variables was negligible (r2 = 0.04 and 0.01, respectively).
Psychosis symptom severity approached significance in predicting post-psychotic PTSD (OR = 1.05; 95% CI 0.99–1.11, p = 0.11; r2 = 0.11) and therefore met criteria for inclusion in multivariate models. After accounting for psychosis symptom severity the association between childhood trauma and post-psychosis PTSD remained strong and significant (OR = 23.49; 95% CI 2.47–223.27, p = 0.01; r2 = 0.46). The proportion of variation explained by the multivariate model was similar to that of the univariate model, which indicated little additional predictive value for psychosis symptom severity. This was also the case for the same multivariate model with childhood trauma-related PTSD as a dependent variable (OR = 17.43; 95% CI 2.78–109.32; r2 = 0.46).
Discussion
Participants in this sample reported high rates of childhood trauma (64%), and psychosis-related PTSD symptoms at clinical levels (47%), which is broadly consistent with previous literature. Previous investigations in FEP groups have found rates of childhood trauma of between 52% and 68% (Greenfield et al., 1994; Neria et al., 2002; Ucok and Bikmaz, 2007) with the exception of one study conducted at Orygen Youth Health (Conus et al., 2010). This study found that 34% of young people reported childhood sexual and/or physical abuse. The lower rate is probably due to the use of file audit over questionnaires to detect trauma, and the exclusion of emotional abuse from the audit. Rates of post-psychotic PTSD in FEP within the first 18 months after acute psychosis in previous studies were between 35% and 66% (Jackson et al., 2004; McGorry et al., 1991; Mueser et al., 2010; Tarrier et al., 2007). The finding that clinical level PTSD symptoms in reaction to childhood trauma (39%) were nearly as high as those of psychosis-related PTSD (47%) in this study makes a valuable contribution to the existing literature.
Both childhood trauma and consequent PTSD dramatically raised the risk of developing post-psychotic PTSD. Further, no illness factor (DUP, psychosis symptom severity and age of onset) could explain the elevated risk. This suggests it is the direct effect of both childhood trauma and childhood trauma-related PTSD that raises the risk of post-psychotic PTSD rather than an indirect effect of childhood trauma and its consequences impacting on the severity of the acute psychotic illness.
Cognitive and biological theories predict more severe PTSD responses in traumatised individuals who have been previously exposed to childhood trauma and PTSD (Ehlers and Clark, 2000; Yehuda et al., 2010). PTSD symptoms are common in response to severe trauma, and extinguish in most people in the months after the trauma (Ehlers and Clark, 2000). Recovery from the trauma of FEP may be compromised by childhood trauma, whereby the cognitive and social strategies developed in childhood to survive the trauma (such as maladaptive schema development, data-driven processing, avoidance) are used to process the acute psychosis memories. These strategies were adaptive for survival in childhood but may maintain PTSD symptoms in adulthood as they may prevent intrusions and hyperarousal from naturally extinguishing. Childhood trauma may also lead to increased stress sensitivity in those with psychosis (Lardinois et al., 2011), which may lead to a more severe stress response to the trauma of psychosis. The data in this study suggest that if young people have not been exposed to childhood trauma, they are generally able to successfully process the trauma of FEP. This, however, must be replicated with a larger sample.
PTSD symptoms in young people with FEP are beginning to be targeted for psychological interventions (Bendall et al., 2010) and thus far controlled trials have focused on PTSD symptoms related to the experience of acute psychosis (Bernard et al., 2006; Jackson et al., 2009). The data from the current study suggest that treating PTSD symptoms from previous traumas in tandem with post-psychotic PTSD may be appropriate as these symptoms are active in many people with FEP.
Limitations
A number of limitations must be noted. First, the study was cross-sectional and so the direction of causality cannot be determined. An alternative explanation for the data is that the trauma of acute psychosis produces PTSD symptoms and also triggers childhood trauma memories and concomitant PTSD symptomatology. Further research with a longitudinal design is needed to elucidate this. However, whatever the causal direction, the fact that PTSD from psychosis and childhood trauma is frequent in the year after a first episode of psychosis indicates a need for intervention to alleviate PTSD symptoms. Second, the study utilised retrospective reporting of childhood trauma (see Bendall et al. (2008) for an exploration of this issue). Third, the sample size of the study was small and confidence intervals around odds ratios are very wide. However, the lower limits of 95% confidence intervals for odds ratios are not less than 3, and highly significant. The results need to be replicated with a larger sample. Fourth, a clinician-rated interview as well as a self-report measure of PTSD symptoms would have strengthened the study. Further research should use both measures of PTSD.
In conclusion, this study highlights two important and hitherto unknown risk factors for post-psychotic PTSD: childhood trauma and childhood trauma-related PTSD. As such, this underlines the importance of assessing for all trauma experiences in people with psychosis (Read et al., 2005). It also suggests that interventions targeting post-psychosis PTSD symptoms in FEP may reduce the chances of PTSD becoming persistent and debilitating by addressing childhood trauma and concomitant PTSD.
Footnotes
Acknowledgements
The authors wish to acknowledge the Colonial Foundation for their support.
Funding
The study was funded by a Melbourne Research Scholarship for SB.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.