
Abstract
The relationship between mental illness and homicide has been established in a variety of studies. Psychotic illness is the serious mental illness (SMI) most often associated with homicide, with non-psychotic mental illnesses other than substance use disorders and personality disorders less overrepresented among homicide perpetrators (e.g. [1-3]). The population studies, the most robust method for this type of research, have employed two types of linkage between mental illness and homicide. The first type defines as mentally abnormal those perpetrators who legal processes define as mentally impaired (such as those found unfit to stand trial, not guilty be reason of insanity or of diminished responsibility) [2-4]. The second type defines perpetrators as mentally abnormal if they received a clinical diagnosis at any time because of treatment contact or in clinical surveys, regardless of their legal outcome [1,5-8]. Legally defined groups can be criticized because the categorizations arrived at are simply measures of the outcome of legal processes, and subject to the vagaries of court [9, 10]. However, they have the advantage that some nexus between mental abnormality and the criminal behaviour must be proven for the legal disposal to occur, at least in insanity and diminished responsibility findings. For the clinically defined groups, the criteria for inclusion have greater clinical rigour, but the link between illness and the offence is unknown. The study of mentally abnormal homicide provides insights into both the prevalence of violent behaviour among people with SMI, and patterns and time trends of the behaviour. It is thus valuable to know if clinical and legal definitions of mentally abnormal homicide are describing the same populations. No study has previously looked at these two types of definition in the same population.
Clearly, the two classifications are measuring different issues, culpability or capacity in the legal approach, and illness and treatment needs in the clinical. They are serving needs of justice on the one hand, and record a clinical history on the other. Different countries employ different criteria for considering how people with a history of mental illness are dealt with if charged with homicide: some, such as Sweden, take generally diagnosis as sufficient for mental health disposition. Anglo-Saxon based legal systems generally rely on a specific defence or nexus being demonstrated in court, meaning either, or even both, mental health or correctional dispositions may occur.
Because of these theoretical differences in definitions, it has been unclear whether the picture gained of the relationship between mental illness and homicide employing different definitions is the same or different. We do not know to what degree the clinical and offence profile of populations defined by different methods may differ. We examined this question by applying both legal and clinical definitions of mentally abnormal homicide to a population of all homicide perpetrators in New Zealand from 1988 to 2000.
Method
This study is part of a larger population study of mentally abnormal homicide in New Zealand. The aim of the principle study was to consider time trends and rates of all homicide in New Zealand from 1970 to 2000. A legal definition of mentally abnormal homicide was used in that study. However, for the purposes of this paper we considered only the time period 1988–2000 as for this time period we could define mentally abnormal homicide using both clinical and legal definitions (the methodology of the study is briefiy described here, but is fully described in [11, 12]).
We defined homicide as events of culpable homicide involving murder, manslaughter, or infanticide as defined in New Zealand legislation. New Zealand clearance rate for homicide has averaged 74% for the last 8 years [13]. Mentally normal homicides were those convicted of murder, manslaughter, those convicted and discharged, and cases of murder-suicide. Murder-suicide is a unique category, as no legal finding, consistent with either mental normality or abnormality, has been made. We placed murder-suicide cases in the legally based mentally normal homicide category consistent with prior research. We examine this group fully in another paper [14].
The legal definition of mentally abnormal homicide was that the perpetrator received one of four mental health dispositions through the courts, namely: unfit to stand trial, not guilty by reason of insanity (NGRI), convicted and sentenced to psychiatric committal, and conviction for the offence of infanticide.
Mentally abnormal homicide by clinical definition were those perpetrators of homicide who had a prior or subsequent hospitalization for SMI as diagnosed on discharge from an inpatient psychiatric facility at any time in their life. We focused particularly on those who received a psychotic diagnosis.
The data sources used were secondary databases in a variety of government agencies. These were:
The Homicide Monitoring Database (HMDB) of the New Zealand Police, which is a detailed schedule that records all homicide events since 1988 with information regarding the circumstances surrounding the event, the victim(s) and the suspect(s) charged with the offence. The Law Enforcement System (LES), which is a national database of criminal prosecutions. Information includes standard demographic data, the date of the offence and the outcome of the court process. The Ministry of Health files of all people who receive a mental health service disposition after a homicide. The New Zealand Parole Board database of people convicted of murder. The Coroner's Court files of murder-suicide perpetrators. The New Zealand Health Information Service (NZHIS) database records admission/discharge details of hospitalization and diagnosis from 1988. Prior to 1988, it was voluntary for health services to submit such detail, but many did. Thus, we searched the earlier incomplete datasets also, but only on homicides occurring after 1988.
The names of all homicide perpetrators from 1988 to 2000 were matched with the NZHIS to detect any hospitalization, and diagnosis on discharge was recorded. We employed a diagnostic algorithm that assigned primacy to a psychotic diagnosis provided it was the major diagnosis. For instance, there was a small number of subjects with many admissions, but with only a single admission suggesting a psychotic illness. Such cases were coded according to the predominant diagnosis. Psychotic illness included schizophrenia, schizoaffective disorder, delusional disorder and affective illness with a psychotic qualifier. Subjects admitted who received another diagnosis comprised the non-psychotic group.
Studies of this type are limited by the fact that original data were gathered by non-researchers for a purpose other than clinical research. While we were likely to have detected most cases with a major psychotic illness, we will have missed many personality, substance and depressive disorder diagnoses that did not result in hospital admission. The datasets have particular limitations as well. Ethnicity, along with other sociodemographic variables, was poorly and incompletely recorded.
Data were entered into SPSS version 11 (SPSS Inc., Chicago, IL, US, 2002) for analysis at the completion of the data collection. Results are presented as raw frequencies. The percentage of total homicide perpetrated by those with SMI is presented in annual groupings. Ethical approval for this study was granted by the Auckland Ethics Committee as a multicentre study and permission for access to specific datasets was gained via research agreements with the Director of Mental Health, the Commissioner of Police and the Ministry of Justice.
Results
In the period 1988–2000 there were 844 convicted homicide perpetrators recorded, with 915 victims. Annual numbers of each type of offender is shown on Table 1. Of the perpetrators, 65, or 7.7% had an admission for a psychotic illness, 122 (14.5%) for a non-psychotic illness and 657 (77.8%) had no psychiatric admissions (Table 1). The rate of mentally abnormal homicide associated with psychotic diagnoses per 100 000 population per annum was 0.16 (95% CI = 0.11 − 0.21). We found no change in psychotic homicide as percentage of annual total homicide, nor the rate per 100 000 population, during the 13 years of the study, although there was marked year by year fluctuation.
Numbers of homicide offenders by year, 1988–2000
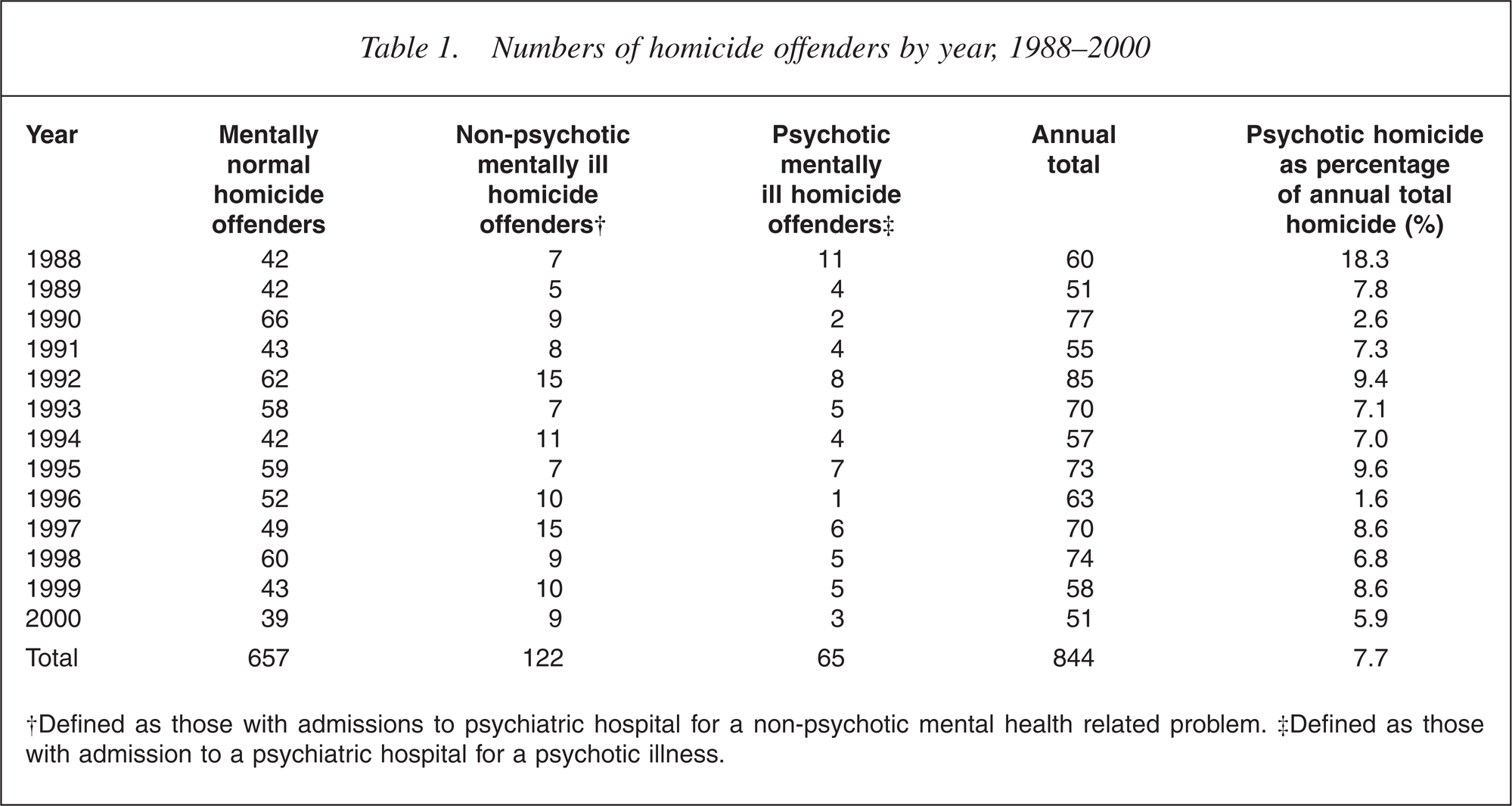
†Defined as those with admissions to psychiatric hospital for a non-psychotic mental health related problem. ‡Defined as those with admission to a psychiatric hospital for a psychotic illness.
Table 2 displays both legal and clinical categories of mentally abnormal homicide. While 65 (7.7%) had been admitted for a psychotic illness, employing the legal criteria found that 60 offenders (7.1%) are deemed to be mentally abnormal (i.e. unfit to stand trial, NGRI, infanticide, convicted and committed). Five cases were initially found unfit to stand trial and were later returned to trial. They are coded by final legal status following the eventual outcome of court process.
Homicide perpetrators by legal and clinical categories, 1988–2000
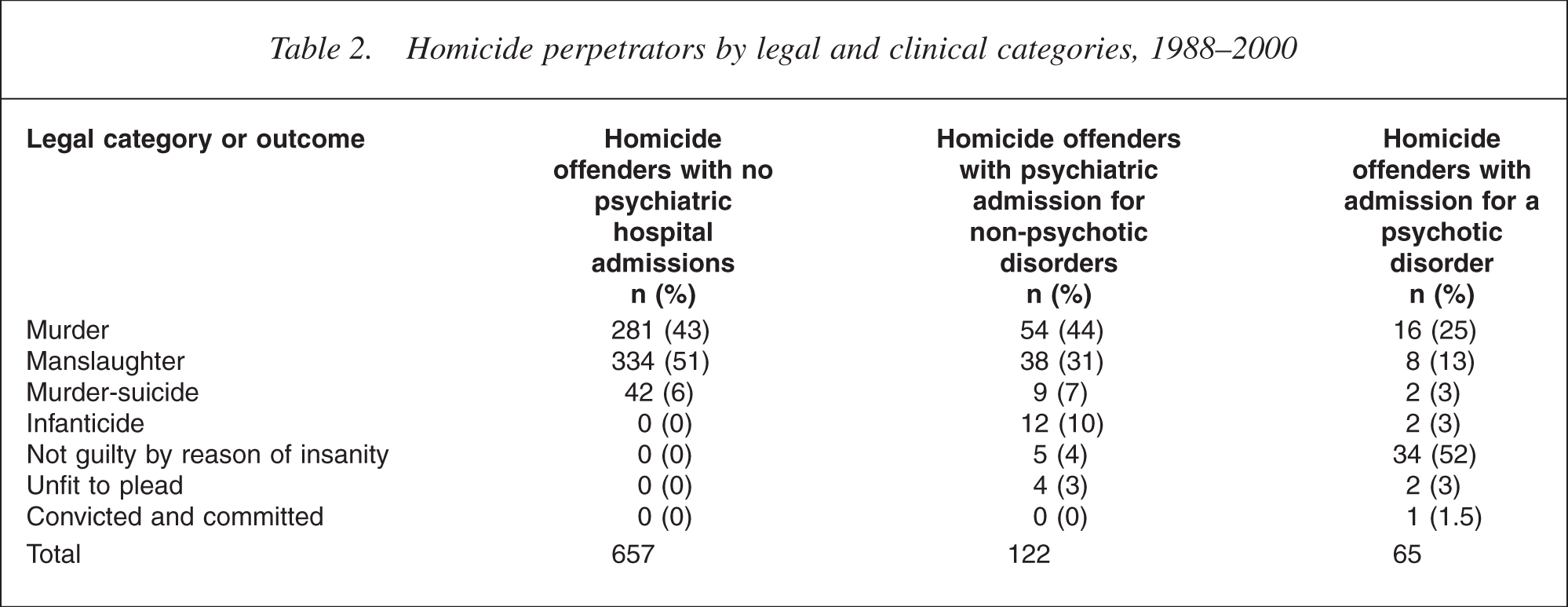
All offenders who were found to have committed a legally defined mentally abnormal offence experienced a hospital admission. Of all convicted of murder, 70 (20%) had a mental health admission at some time in their life, of whom 16 (4.5%) had an admission for a psychotic disorder. For manslaughter, 46 (12.1%) had a hospital admission of whom eight (2.1%) were for a psychotic disorder. Of the 39 people acquitted on the grounds of insanity, 34 (87.1%) suffered a psychotic illness. The remaining five offenders suffered a major depressive illness (three cases) or organic disorders (two cases).
There is very considerable overlap between the groups. Of the total of 844 perpetrators, 758 (89.8%) were in neither the legal or clinical abnormal groups, 26 (3.1%) were in just the clinical, 21 (2.5%) in just the legal, and 39 (4.6%) in both the clinical and legal groups. The 26 offenders who were only in the clinical group are comprised of two who committed murder-suicide but had a history of psychotic illness, and 24 with a prior psychotic illness who were convicted of murder (16 cases) or manslaughter (eight cases). These subjects served prison sentences, but 17 had further psychiatric admissions during sentence. Put another way, of the 65 perpetrators who received a psychotic diagnosis, 39 (60%) received a mental health disposition (of whom 34 were found NGRI), two committed murder-suicide and 17 remained in contact with mental health services as measured by admission. Thus, 56 of the 63 surviving offenders with a psychotic history (89%) received a hospital disposition or spent periods of their incarceration in hospital.
The 21 who did not have a psychotic diagnosis but received a legally abnormal categorization were primarily those with less SMI and convicted of infanticide, and a small group of perpetrators with organic and depressive disorders found NGRI or unfit to plead.
The murder-suicide group is a difficult one to categorize, Barraclough and Harris [15] comment noting they overlap with both mentally abnormal homicide and mentally normal homicide groups. Of the 53 murder-suicide cases, 11 had prior admissions of whom two had received a psychotic diagnosis.
Of the 122 homicide perpetrators who had been admitted with nonpsychotic diagnoses, 101 (82.8%) were perpetrators of legally defined mentally normal homicide, with 12 cases of infanticide (10%) being the only significant legally defined mentally abnormal offence category.
Table 3 shows the comparison between the characteristics of the offenders without psychiatric admission, with admission for a nonpsychotic disorder and admission for a psychotic disorder. Offenders without admission were more likely to be male, and the offenders with admission for a non-psychotic disorder were most likely to be female, with 22% female compared with 9% for the non-admitted group (χ2 = 20.2, df = 2, p < 0.001). This was primarily accounted for by the infanticide perpetrators being present in the non-psychotic admitted group. Psychotic offenders took up an intermediary position. Mean age was distributed similarly, with the non-admitted being youngest and those admitted with a non-psychotic illness significantly older (ANOVA F = 9.2, df = 2, p < 0.001). The age difference was primarily because of a much larger proportion of the mentally normal group (21%) being less than 20 years, as compared with the other two groups (8%). Ethnicity showed greater over representation of Pacific Island and other people in the non-admitted group when compared with the other two subpopulations (χ2 = 50.4, df = 12, p < 0.001).
Characteristics of offenders with and without psychiatric admission
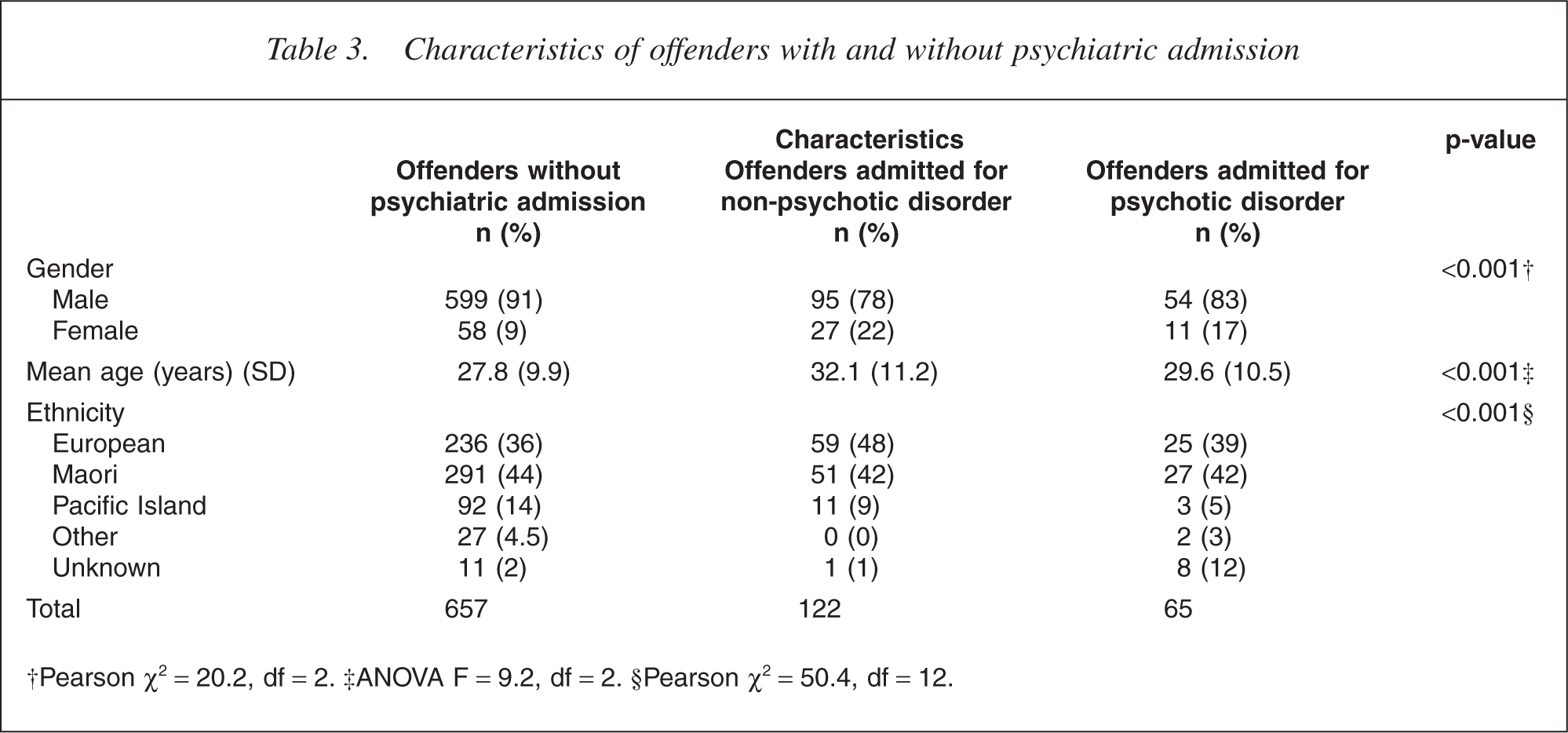
†Pearson χ2 = 20.2, df = 2. ‡ANOVA F = 9.2, df = 2. §Pearson χ2 = 50.4, df = 12.
Investigation of the timing of the first admission in relation to the homicide found that 74% (90/122) of those admitted for nonpsychotic diagnoses had admissions prior to the homicide and 12% (15/122) at the time of the homicide. Significantly more psychotic patients were admitted for the first time immediately following the homicide (28%, 18/65) with fewer admissions (60%, 39/65) prior to the homicide (χ2 = 6.9, df = 2, p = 0.03). Similar numbers (14% 17/ 122 and 12% 8/65, respectively) had first admissions subsequent to but not immediately after the homicide. Relatively few perpetrators were admitted in the time immediately prior to the offence (5% or 6/ 122 and 11% or 7/65, respectively), although 18% (21/122) of the perpetrators with an admission for a non-psychotic illness and 31% (20/65) of those with a psychotic illness were admitted in the year prior to the offence. In all, 42% (50/122) of the-non-psychotic group and 48% (31/65) of the psychotic group had admissions in the 5 years prior to the offence.
Discussion
This study provides further evidence for an association between mental illness and homicide. In the absence of good community prevalence studies of mental disorder in New Zealand, we are unable to calculate accurate odds ratios for the increased homicide risk with psychotic or other illness. Nonetheless, we have little reason to believe that the community prevalence of psychotic disorders in general exceeds the approximately 1% of the population found in most other countries, making the finding of around 7% of the homicide population meeting either legal or clinical criteria for mental disorder a clear overrepresentation. This magnitude of association is similar to other comparable studies [2–6].
Further, we found that while 22.1% of homicide perpetrators had admissions at some time for mental disorders, most were for non-psychotic disorders that uncommonly resulted in a legal categorization as mentally abnormal. The only exception to that was the offence of infanticide, where depressive disorders were accepted as grounds for this specific diminished responsibility offence. If a perpetrator had a psychotic diagnosis (as 7.7% had) over half received a not guilty on the grounds of insanity finding, and a total of 60% a mental health disposition. Just under one-third of psychotic offenders were first admitted at the time of the offence and another 12% once in prison. In all, 89% of offenders with a psychotic diagnosis remained in mental health care, either as a result of mental health disposition or on transfer to hospital from prison.
Our finding that 22.1% of perpetrators had had a mental health admission at any time is lower than the Confidential Inquiry in England and Wales, which found that 31% had prior mental health service contact [7]. Shaw et al. [7] found that most of these problems were for substance misuse and personality disturbance, as Mullen et al. [16] have also emphasized in relation to violent behaviour more generally. For those with a psychotic illness, however, this raises the issue of to what degree mental health services may have been able to predict or prevent tragedies among people with psychotic illness. Reviews of inquiries into such events have generally found that delivery of effective services would have prevented approximately 60% of them [17], [18]. Rare events are hard to predict, and the events where the person has no prior mental health contact cannot be seen as service failures. However, there may be a significant number that are preventable with the provision of effective services.
The limitations of this study are that the diagnoses used were discharge coded and not verified in a research paradigm, and no interviews of offenders occurred, making missed disorders quite probable. This is especially so for less serious mental disorders, personality disorders and substance misuse. However, there have been well developed forensic psychiatric services to prisons and a psychiatrically informed National Parole Board operating during the period of this study and thus it is unlikely that many cases of psychotic illness among life prisoners (the mandatory sentence for murder) have been missed. However, there may well be poorer detection of other mental disorders among the other sentenced prisoners, as found in a survey of New Zealand prisoners [19]. Further, a high-level case linkage study cannot test the relationship, if any, between specific symptoms of illness and the homicide.
There have been no previous studies that link the two means of defining mental abnormality in the same population, and can look at the relative contribution of mental disorder to the various legal categories to enable the tracing of all those, for instance, with a psychotic illness who perpetrate homicide. Legal definitions require a nexus between the illness symptoms and the offence, for instance via an insanity test or a diminished responsibility test. However, legal tests may be subject to the vagaries of local political or social factors, although Appelbaum [20] suggests that the rate of NGRI acquittals may be less prone to variation than one might imagine. In general, however, legal definition and clinical definition find similar global rates of mentally abnormal homicide, with similar profiles of age, gender and ethnicity (3, 2 for legal categorizations; 5, 6, 7, 1 and 8 for clinical categorization). Both definitions of mental abnormality find an increased prevalence of homicide perpetrators, and that mentally abnormal homicide perpetrators are older, more likely to be female and less likely to be of minority ethnicity. We found this also, regardless of whether legal or clinical definition was applied. This suggests that different factors may give rise to mentally abnormal homicide than give rise to mentally normal homicide. This is supported by the finding that neither legal nor clinical defined rates of mentally abnormal homicide showed any significant time variations, while total homicide increased threefold from 1970 to 1992, and has declined since then [11], [12]. However, even though some differences can be discerned between these groups, males, young adults (less than 35 years) and those of minority ethnicity remain over represented in all offender groups relative to the total population.
Unlike Wallace et al. [1] who found that only one from eight homicide perpetrators who had a schizophrenic diagnosis received a mental health disposition, we found 60%. New Zealand has a broad McNaughten-based insanity test that is interpreted purposively by courts and juries. Although there is no volitional component to this test, it still allows juries to consider the effect of psychotic symptoms on moral judgement, and this may allow more frequent offenders with psychotic illness insanity findings than other jurisdictions. Further, a successful NGRI plea in New Zealand always resulted in a hospital disposition, which did not always happen in Victoria during the same time period. As UK data have shown, the use of the defences to murder may be affected by multiple factors including the wording of legislation, the effects of the finding and prevailing practice [21]. Intriguingly, although, in our sample most offenders with a psychotic diagnosis were diverted to hospital, either as their total disposition or via periods of post-conviction admissions suggesting that clinical needs determine pathways through care, even if convicted of the offence as charged.
Legal and clinical definitions of abnormal homicide appear to yield helpful insights, with the legal categorizations tending to lend themselves to longer-time trend studies, and clinical methods generally only being applicable in more recent time periods, when clinical registers have been more common. These data raise the hope of prevention of some of these offences, and the fact that all offenders with mental illness are not diverted at court emphasizes the need for ongoing care in prison to meet clinical need that is not deemed relevant to culpability. Future research should consider matched homicide offenders to study patterns and motivations, with the contribution of personality, illness symptoms, disability and service provided, to offence context and outcome.