
Abstract
Objective:
We examined the overlap between mood and anxiety disorders and psychological distress and their associations with functional status in Canadian Armed Forces (CAF) personnel.
Method:
Data on Regular Forces personnel (N = 6700) were derived from the 2013 Canadian Forces Mental Health Survey, a nationally representative survey of the CAF personnel. Current psychological distress was assessed using the Kessler K10 scale. Past-month mood and anxiety disorders were assessed using the World Health Organization World Mental Health Composite Diagnostic Interview.
Results:
The prevalence of psychological distress was the same as that of any past-month mood or anxiety disorder (7.1% for each). A total of 3.8% had both distress and past-month mood or anxiety disorder, 3.3% had past-month disorder without psychological distress, while another 3.3% had psychological distress in the absence of a past-month mood or anxiety disorder. After adjusting for age, sex, marital, education, income, language, element, rank, and alcohol use disorder, individuals with both psychological distress and past-month mood and anxiety disorders exhibited the highest levels of disability, days out of role, and work absenteeism relative to those with neither mental disorders nor psychological distress. Relative to individuals with both disorder and distress, those who endured distress in the absence of mental disorder exhibited lower, but meaningful, levels of disability compared with those with neither disorder nor distress.
Conclusions:
Disability is most severe among CAF personnel with both distress and past-month mood and anxiety disorders. Nevertheless, distress in the absence of disorder is prevalent and is associated with meaningful levels of disability.
Background
Mental disorders are prevalent and generate significant negative impacts in the workplace, including absenteeism, unwanted turnover, impaired productivity, and higher medical care costs. 1,2 The past 16 years of armed conflict in southwest Asia has underlined the special significance of mental disorders in military personnel. 3 They may be exposed to psychological trauma as part of their duties, meaning that many mental disorders are work related. 4 –7 In addition, mental disorder–related impairments may be particularly impactful in the high-risk, high-stakes conditions that occur during armed conflict. Effective surveillance, prevention, and control efforts must begin with a firm understanding of the extent of these important public health issues.
Mental disorders have variable impacts on well-being and functioning. Some individuals with a given level of symptomatology will be seriously disabled, while others will be able to continue to function well in at least some domains. 8 Subclinical levels of distress in the form of subthreshold disorders may also have significant impacts on functioning. 8 In parallel, individuals who experience psychological distress may exhibit variable effects on functioning depending on the presence or absence of a past-month mood or anxiety disorder. Research has shown that military personnel may be affected by a wide range of mental health disorders. 9,10
While studies of mental disorder prevalence in military organizations abound, there is little research on the occupational impacts of mental health problems on military personnel. Existing research has examined the isolated effects of mental disorders on disability and work absenteeism in military personnel. 2,11 However, to the best of our knowledge, there has been no previous examination of the combined effects of overlapping mental disorders and psychological distress on disability among military personnel. Thus, the objective of this study was to examine the overlap between past-month mental disorders and psychological distress and their associations with functional status in Canadian Armed Forces (CAF) personnel. More specifically, we (1) estimated the proportion of 4 key groups described by presence or absence of a past-month disorder and the presence or absence psychological distress and (2) examined the association between functional status and membership in these 4 groups. Given the gap in the literature, we had a particular interest in those who had clinically significant distress in the absence of a past-month disorder.
Methods
Data were derived from the 2013 Canadian Forces Mental Health Survey, a representative, cross-sectional survey of mental health of Canadian Armed Forces Regular Force personnel, as well as reservists who were deployed in support of the mission in Afghanistan (N = 8165; with a response rate of 80%). 12 The analyses of the present study are restricted to the Regular Force sample (N = 6696), representative of approximately 68,000 Regular Force personnel in the CAF in 2012. Respondents were predominantly young and middle-aged, male, and married or in common-law relationships. More than half had a postsecondary degree and a household income of $80,000 or more. Slightly more than half were in the Army and were junior noncommissioned members (NCMs). 13 Detailed information about the methodology of the 2013 Canadian Forces Mental Health Survey is available elsewhere. 14 The research protocol was approved by the relevant entities within Statistics Canada. Participation was voluntary, and all participants provided informed consent.
Mental Disorders
Mental disorders were assessed with the World Health Organization World Mental Health Composite International Diagnostic Interview (WMH-CIDI), which is a comprehensive, structured lay-administered psychiatric interview for the assessment of mental disorders. 15 The WMH-CIDI has shown good consistency with clinical diagnostic instruments. 16,17 The mental disorders measured included posttraumatic stress disorder (PTSD), major depressive episode (MDE), generalized anxiety disorder (GAD), panic disorder (PD), and alcohol use disorder (abuse or dependence). Diagnostic and Statistical Manual of Mental Disorders, fourth edition, criteria were used to create an algorithm to classify people likely to receive a clinical diagnosis.
Past-month disorder was assessed among those with past-year disorders using 1 or more items in each of the disorder-specific modules that asked how recently they had had the key symptoms of the disorder (e.g., depressed mood or anhedonia in the case of depression) within a 12-month time frame, with options including the past month, 2 to 6 months previously, and more than 6 months previously. One aggregate variable was constructed indicating those with any 30-day mood or anxiety disorder (PTSD, MDE, GAD, or PD).
Psychological Distress
The Kessler Psychological Distress Scale (K10) was used to detect nonspecific psychological distress (symptoms of anxiety and depression) occurring over the most recent 4-week period. 18,19 The K10 includes 10 items for which responses are scored on a 5-point ordinal scale—from 0 (none of the time) to 4 (all of the time)—and summed to generate a total score ranging from 0 to 40, with higher scores indicating higher levels of psychological distress. K10 has been widely used in large-scale health surveys in military, veteran, and civilian populations in a number of countries. 20 –22 The K10 has undergone validation in both general 23 –26 and military 27,28 populations, and various cutoffs have been proposed to estimate the prevalence of mental disorders and to screen for mental disorders. In the present study, the K10 scale was dichotomized based on a cutoff of 17 or greater that was previously identified for use in prevalence estimation of clinically significant psychological distress in CAF personnel. 13 At that cutoff, the number of false-positives was equal to the number of false-negatives, using any past-month mood or anxiety disorder as a reference point.
Disability
Disability was measured using the 12-item version of the World Health Organization Disability Assessment Schedule (WHODAS-2), a widely used and highly reliable self-report questionnaire that assesses disability during the past 30 days. 29 This measure has been validated in general civilian 30,31 and military populations, 11 and it has shown good internal consistency. Questions were preceded by, “In the past 30 days, how much difficulty did you have in…” and rated on a scale from 1 (none) to 5 (extreme/cannot do) and grouped into 6 subscales of 2 items each, representing various domains of functioning. In the Canadian Forces Mental Health Survey (CFMHS), total WHODAS-2 scores were computed using the “complex” scoring method recommended in the WHODAS-2 manual, 29 yielding scores from 0 (no disability) to 100 (full disability). In addition to these total scores, we created 3 severity categories following the International Classification of Functioning, Disability, and Health (ICF) 32 severity ranges (no disability, 0 to 4; mild disability, 5 to 24; and moderate to severe/extreme disability, 25 to 100).
Days out of role was measured Statistic Canada’s Two-Week Disability module, using 3 items that asked participants to report the number of days out of the past 14 days they “stay in bed for all or most of the day,” “cut down on things for all or most of the day,” and the number of days that “required extra effort.”
Absenteeism was assessed using the World Health Organizations’ Brief Health and Work Productivity Questionnaire, 33 with items assessing the number of days the respondent missed an entire or part of a work day because of problems with their physical or mental health during the previous 4 weeks (28 days).
Covariates
Covariates included age group in years (24 or younger, 25 to 34, 35 to 44, and 45 or older), sex, marital status (married or common-law; widowed, separated, divorced, or widow or never married), education (secondary graduation or less, some postsecondary, or postsecondary graduation), household income (none or less than $59,999, $60,000 to $79,999, and $80,000 or more), language (English/French), element (Army, Navy, or Air), rank (junior NCM, senior NCM, or officer), and past-month alcohol use disorder (which was conceptualized as a potential confounder of the relationship between past-month mood or anxiety disorders and the functional status outcomes).
Statistical Analysis
All analyses were weighted to accurately reflect the demographics of the military population, and bootstrap replicate weights were used for variance estimation given the complex sampling design of the survey. Presence or absence of psychological distress and any past-month mood or anxiety disorder were combined to create a 4-level variable indicating (1) psychological distress in the absence of past-month mood or anxiety disorder, (2) past-month mood or anxiety disorder in the absence of psychological distress, (3) both psychological distress and past-month mood or anxiety disorder, and (4) neither psychological distress nor past-month mood or anxiety disorder. Descriptive analyses were used to examine bivariate associations of overlapping psychological distress and past-month mood and anxiety disorder with sociodemographic (age, sex, marital status, education, household income, and language) and military (element and rank) characteristics, alcohol use disorder, and functional status (disability and days out of role and absenteeism). To achieve normality criteria, Box-Cox procedures were used as general guidance to pragmatically find the optimal normalizing transformation for each outcome variable of WHODAS score and annual days out of role and absenteeism, which were subsequently inverse-transformed. Multiple linear regression and multinomial logistic regression analyses were performed to examine the relationship between overlapping psychological distress and mental disorder with functional status in Canadian military personnel. Multiple linear regression analyses were conducted with both transformed and untransformed variables. Given that the overall pattern of results did not differ, results using untransformed variables are presented to maintain interpretability of the findings. All statistics were computed using STATA (version 13.1, Stata Corp., College Station, TX).
Results
Prevalence of Psychological Distress and Past-Month Mood or Anxiety Disorders
Table 1 presents the overlap between psychological distress (K10 score greater or equal to 17) and past-month disorders. The prevalence of psychological distress was the same as that of any past-month mood or anxiety disorder (7.1% for each). About 3.3% of the military population had psychological distress in the absence of any past-month disorder. An additional 3.8% of participants had both distress and past-month mood or anxiety disorder, while 3.3% had a past-month mood or anxiety disorder but no psychological distress.
Overlap between psychological distress and past-month mood or anxiety mental disorders.
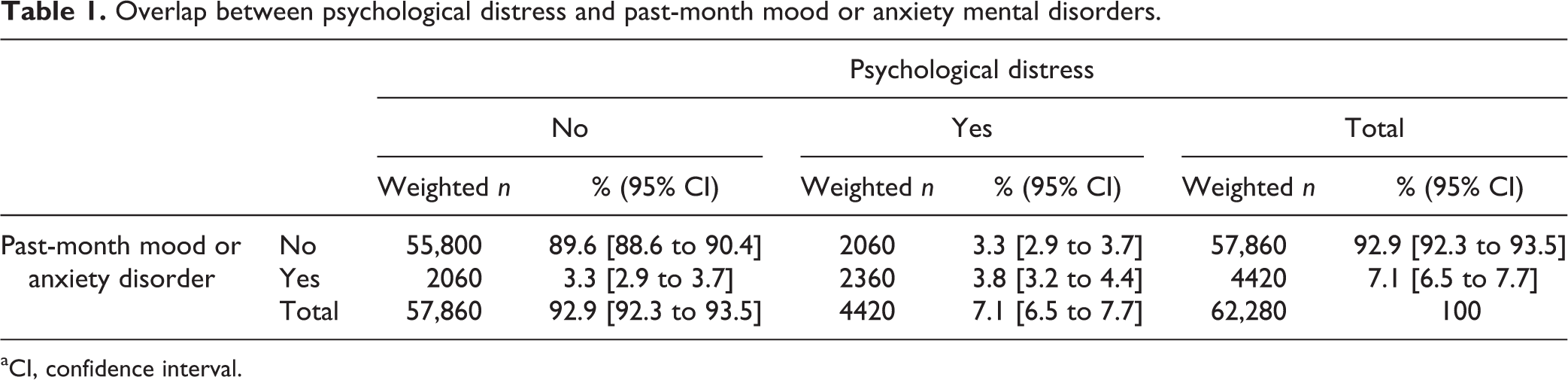
aCI, confidence interval.
Correlates of Mood and Anxiety Disorders and Distress
Sociodemographic and military correlates of overlapping mental disorders and psychological distress are outlined inTable 2. Age, sex, marital status, house income, rank, element, and alcohol disorder were significantly associated with mental disorders and psychological distress. While there was little difference across all characteristics among individuals with psychological distress in the absence of a past-month disorder, those aged 24 years or younger were less likely to have both distress and past-month disorder (1.7%). Those who indicated marital status as separated, divorced, or widowed were more likely to have both distress and past-month disorder (7.0%) than those who were single, married, or common law.
Sociodemographic and military correlates of overlapping mental disorders and psychological distress.a
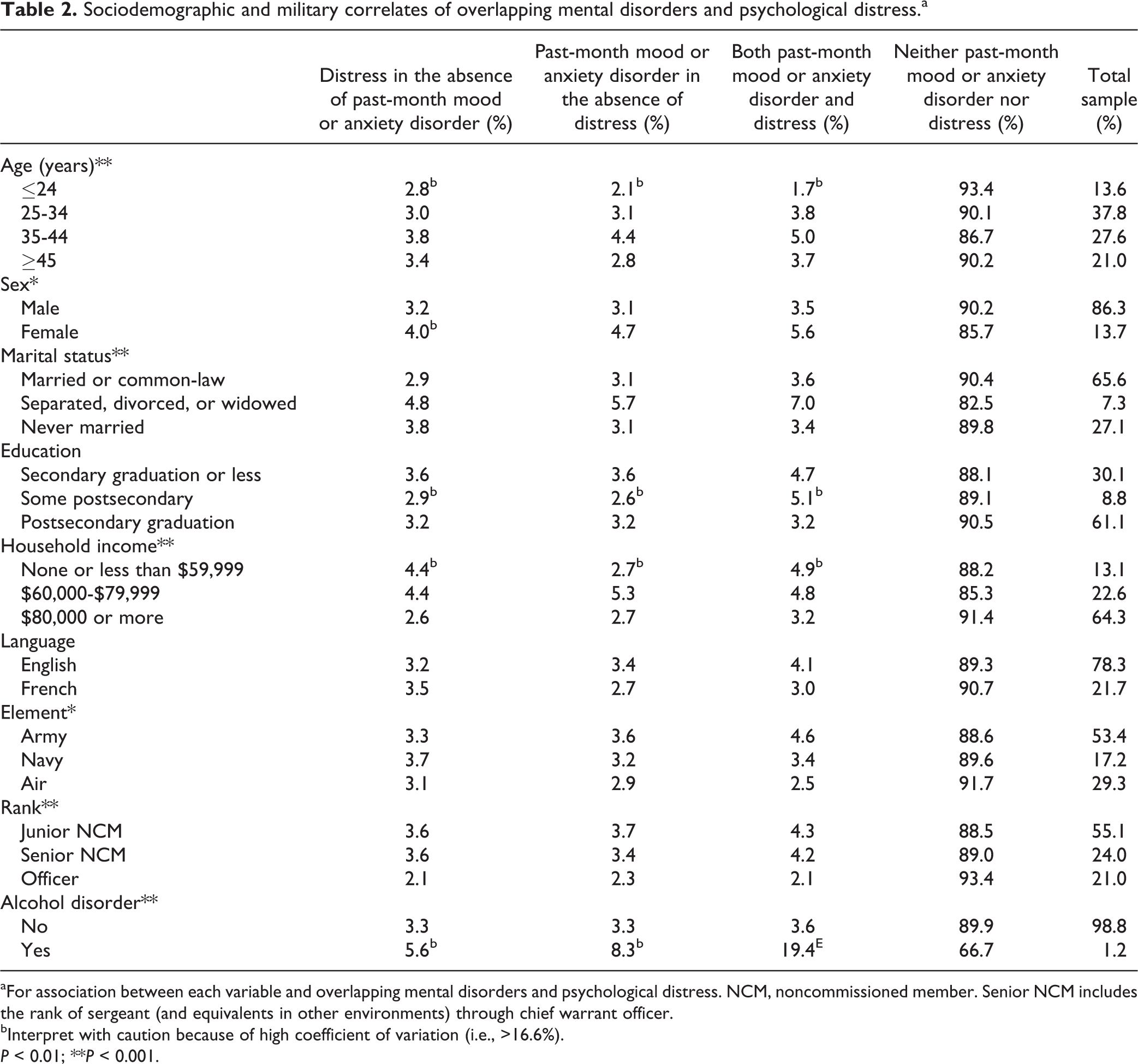
aFor association between each variable and overlapping mental disorders and psychological distress. NCM, noncommissioned member. Senior NCM includes the rank of sergeant (and equivalents in other environments) through chief warrant officer.
bInterpret with caution because of high coefficient of variation (i.e., >16.6%).
P < 0.01; **P < 0.001.
Table 3 displays the results of bivariate association between functional status and mental disorders/psychological distress. Most participants had no disability (59.4%) or minimal disability (30.6%), whereas an important minority had moderate to severe disability (10.0%). Individuals with both psychological distress and past-month disorders had the highest levels of functional status across all outcomes (WHODAS, days out of role, and absenteeism). Those above the cutoff for “psychological distress” in the absence of a past-month mood or anxiety disorder had lower levels of disability than those with a past-month disorder, although this group still a substantial prevalence of moderate to severe disability (39.6% vs. 51.1% for those with a past-month disorder).
Functional status as a function of disorder and distress.a
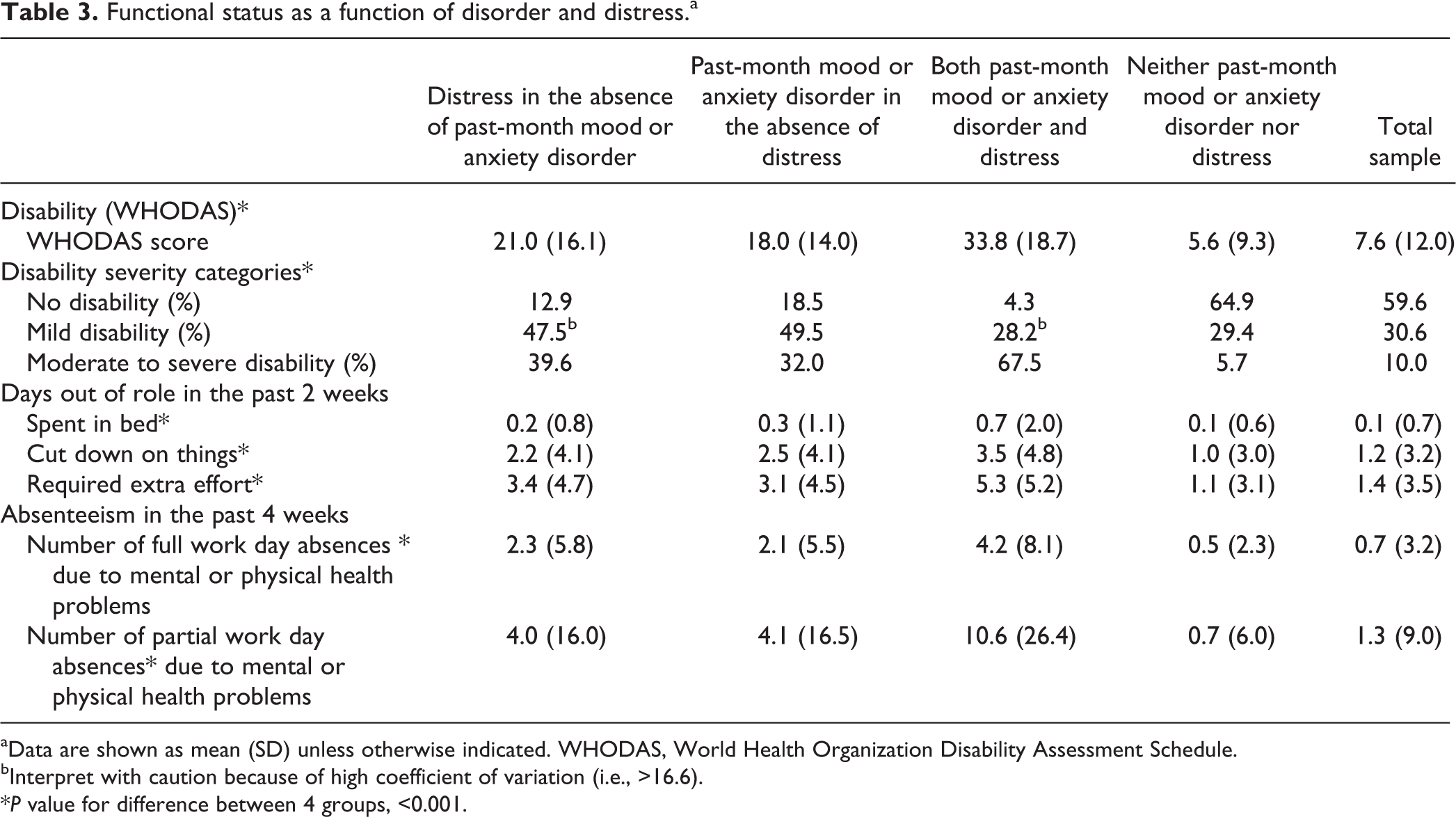
aData are shown as mean (SD) unless otherwise indicated. WHODAS, World Health Organization Disability Assessment Schedule.
bInterpret with caution because of high coefficient of variation (i.e., >16.6).
*P value for difference between 4 groups, <0.001.
Results of multiple linear regression analyses (using untransformed dependent variables of disability, days out of role, and absenteeism) adjusting for sociodemographic and military characteristics and alcohol use disorder are presented in Table 4. Consistent with the bivariate associations, there were strong relationships between mental disorders and distress with functional status. Overall, disability was most severe among CAF personnel with both clinically significant distress and past-month mood and anxiety disorders. For example, compared with individuals with neither mental disorders nor psychological distress, those with both clinically significant distress and past-month mood and anxiety were more likely to have greater levels of disability (B = 26.85; 95% confidence interval [CI], 24.32 to 29.37) and to report increased number of days out of role in past 2 weeks (spent in bed [B = 0.57; 95% CI, 0.23 to 0.92], cutting down on things [B = 2.21; 95% CI, 1.57 to 2.86], and required extra effort [B = 4.03; 95% CI, 3.31 to 4.74]) and elevated number of full and of partial work day absences due to mental or physical health problems in the past 4 weeks (B = 3.54; 95% CI, 2.34 to 4.73; and B = 9.45; 95% CI, 5.45 to 13.44, respectively). Contrary to individuals with both disorder and distress, those who endured distress in the absence of mood and anxiety disorder exhibited lower, but meaningful, levels of disability compared with those neither disorder nor distress.
Results of linear regression analyses examining the associations between overlapping mental disorders and psychological distress with functional status.a
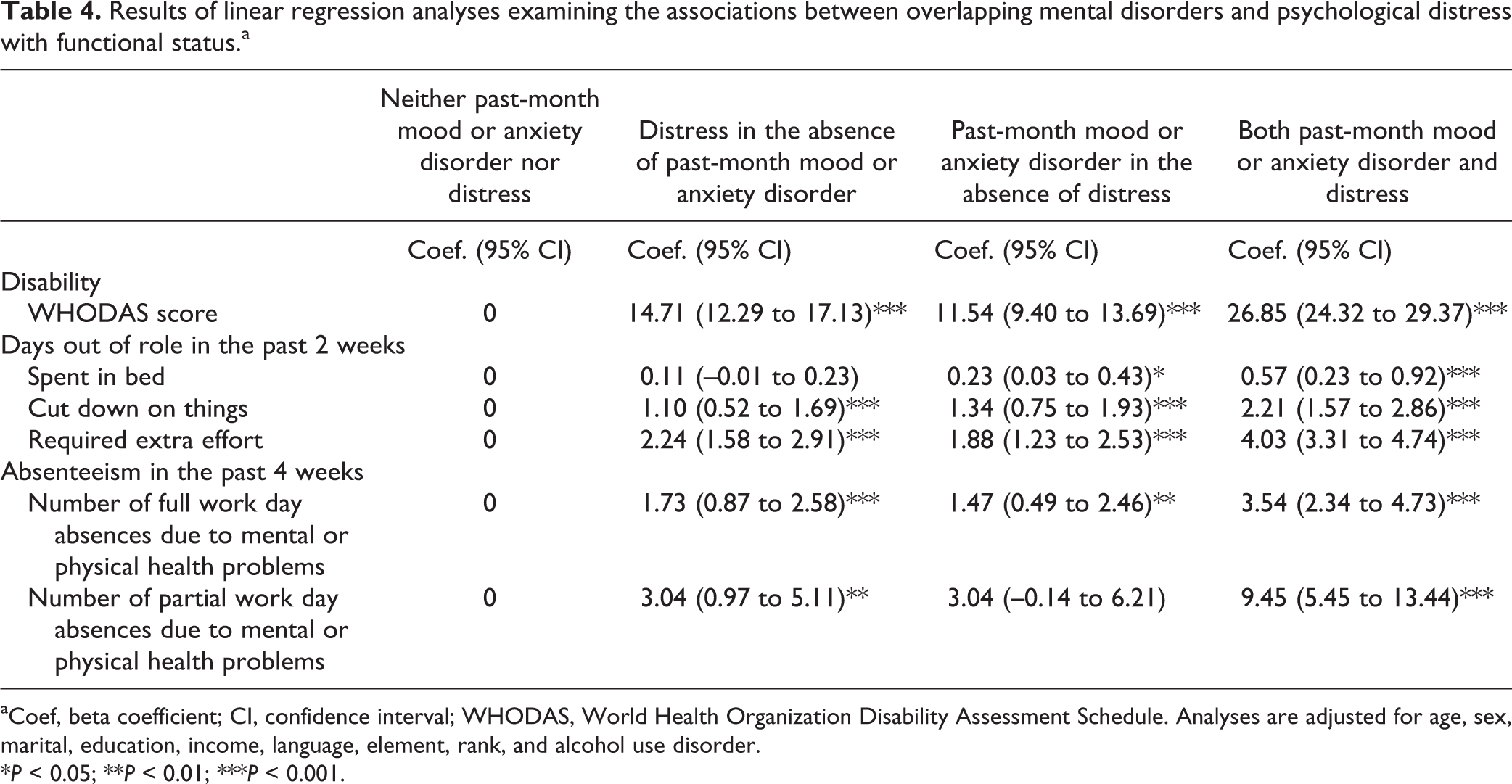
aCoef, beta coefficient; CI, confidence interval; WHODAS, World Health Organization Disability Assessment Schedule. Analyses are adjusted for age, sex, marital, education, income, language, element, rank, and alcohol use disorder.
*P < 0.05; **P < 0.01; ***P < 0.001.
Table 5 displays results of multinomial logistic regression analyses examining the associations between overlapping mental disorders and psychological distress with disability severity categories. After adjusting for sociodemographic and military characteristics, individuals with distress only, disorder only, and with both distress and mental disorder were more likely to have mild or moderate to high disability compared with those with neither mental disorder nor distress. However, the relative risks were significantly higher for moderate to high disability than mild level across all mental health indicators. Moreover, those with both psychological distress and past-month mood and anxiety disorder had the highest relative risk for moderate to severe disability compared with those with other mental health indicators (i.e., distress in the absence of mental disorder and mental disorder in absence of psychological distress).
Results of multinomial logistic regression analyses examining the associations between overlapping mental disorders and psychological distress with disability severity categories.a
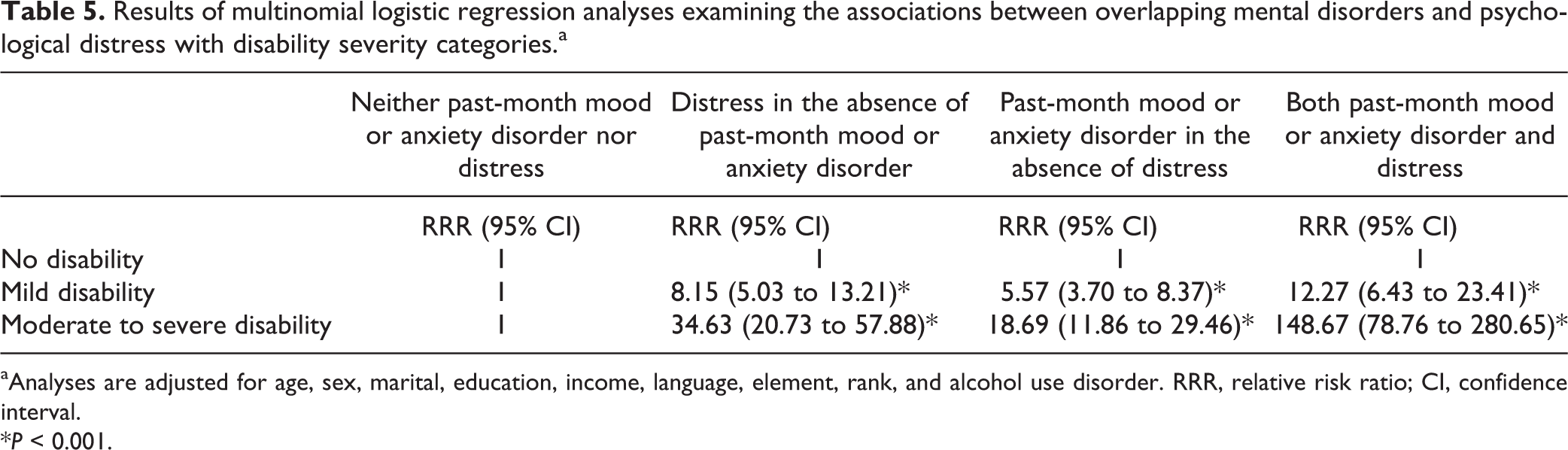
aAnalyses are adjusted for age, sex, marital, education, income, language, element, rank, and alcohol use disorder. RRR, relative risk ratio; CI, confidence interval.
*P < 0.001.
Discussion
Summary of Key Findings
This study used a representative sample of CAF Regular Force personnel to examine the overlap between mental disorders and psychological distress and their associations with functional status. Results indicated that 3.3% of the population had psychological distress in the absence of a past-month disorder assessed by the survey. An additional 3.8% had both distress and past-month mood or anxiety disorder, while 3.3% had a past-month mood or anxiety disorder but no psychological distress. While psychological distress in the absence of a past-month disorder had meaningfully elevated levels of functional status (across all outcomes, relative to those without distress or disorders), functional status was significantly greater in those with both distress and past-month mood or anxiety disorder.
Comparison with Other Findings
The prevalence of psychological distress in the absence of a past-month mood or anxiety disorder and that of past-month mood or anxiety disorder in the absence of psychological distress reported in our study are lower than those calculated based on the information provided in a previous study among Australian military population (5.9% and 6.3%, respectively). 28 Discrepancies may be related to the use of a different cutoff of 25 (corresponding to 15 on the 0-40 scaling we used) for the K10, which was deemed optimal in the Australian military population, using the same approach of balancing the number of false-positives with false-negatives. 28 However, their cutoff demonstrated a lower sensitivity (30%) than ours (52.8%). It is also possible that the poor final response rate for the Australian survey (24%), the assessment of more mood and anxiety disorders than we did, and the use of different outcome measures (disorder assessed using ICD-10 criteria) explain the observed discrepancies.
Given that only the presence or absence of past-month disorder was assessed in the present study, it is possible that the overlap with distress and its association with functional status simply reflect the severity of the disorders. Mental disorders have variable impacts on well-being and functioning: some individuals with a given level of symptomatology will be seriously disabled, while others will be able to continue to function well in at least some domains. On the other hand, many individuals experience symptoms that are not sufficient to meet diagnostic criteria but may nevertheless affect function. This is particularly evident for mood and anxiety disorders, where symptoms appear to exist on a continuum and there is considerable overlap with distress. 34,35 Individuals with such subthreshold symptoms have poorer quality of life, worse function, and worse outcomes. 35 –38 Particularly relevant for the military, those with subthreshold symptoms of PTSD have significant levels of impairment. 39,40 Such subclinical symptoms may be particularly important in a military setting, where higher impairment associated with subthreshold symptoms could affect operational success of missions. Subthreshold symptoms have been associated with occupational outcomes; subthreshold PTSD is associated with poor occupational functioning, 40 while subthreshold depression is associated with a significant number of days unable to work. 41
Strengths and Limitations
This study has several limitations worth mentioning. First, the cross-sectional nature of the CFMHS precludes determination of temporality between mental health problems and disability (although evidence has shown that disability is more likely to result from mental disorders than vice versa). 42 Notably, we could not attribute the extent of disability in those with clinically significant distress to the distress itself, as opposed to other factors. We could not, for example, identify how many had a disorder that was not assessed by the survey (e.g., bipolar disorder, obsessive-compulsive disorder, phobias), including some that have been indicated to be prevalent among military personnel elsewhere. 9,10 These nonassessed disorders could be the root of distress. However, given the difficulty in assessing all those disorders in one survey module, the prevalence of psychological distress may serve as a proxy to understand the prevalence of current disorders not covered by the disorder-specific survey modules used in the survey. Future research using a longitudinal design is needed to disentangle the interrelationships between mental disorders, psychological distress, and functional status. Second, although the present study used an optimal cutoff (of 17 or greater) for the K10 scale that was established in this study population, imposing any single cutoff (no matter how rigorously established) for a continuous construct such as psychological distress measured by the K10 may have resulted in loss of information and misclassification. Third, findings from this study cannot be generalized to Reserve Force military personnel because our analyses were restricted to the Regular Force sample.
Strengths of this study include the use of past-month mood or anxiety disorder, which has been indicated to be a good metric for current population mental disorders, whereas previous studies in the Canadian military personnel have focused on past-year measure of mental disorders. The use of past-year disorders as a primary outcome may have overestimated the current burden of poor mental health because it captures both the currently ill and the recently ill individuals. The K10 cutoff score of 17 or greater used in the present study has been previously validated in the same sample. 13 As such, the present study aligns with previous recommendations that a cutoff always be validated before use in the population of interest to ensure that the scales are working optimally. 28,43,44 Our study is the first to examine the overlap between mood and anxiety disorders and psychological distress and their associations with functional status in Canadian military personnel, who have increased risk of exposure to occupational trauma, which increases their risk of many mental disorders. Our study highlights the importance of considering individuals with psychological distress in the absence of a past-month disorder who have low but substantial levels of disability. Lastly, the current analyses benefited from an ample sample size and the high response rate.
Implications
The implications stemming from this study largely depend on the reasons for the observed mismatch between distress and mental disorders. Significantly, our results identified a small but important group of individuals with clinically significant psychological distress in the absence of common mental disorders, in that they had lower, though substantial, levels of disability relative to those with current disorder. This group of individuals with clinically significant psychological distress in the absence of common mental disorders is likely diverse, including but not limited to the following: those with a past-year disorder in which the key symptoms were not present in the past month, but other symptoms (e.g., insomnia) might be leading to distress; those with subthreshold conditions; those with past-month disorders not assessed by the survey; those experiencing distress related to a specific recent stressor; and those who had a past-month disorder but for whom the CIDI was false-negative. Hence, more practical implications could be driven by trying to get a better sense of who these distressed but not disordered people are and whether they had received treatment or not. Until there is a better understanding of this group, military personnel who endure significant distress should be evaluated clinically.
Conclusion
To the best of our knowledge, the present study is the first to examine the overlap between mood and anxiety disorders and psychological distress and their associations with functional status in Canadian military personnel. Our results identified a small but important group of individuals with clinically significant psychological distress in the absence of common mental disorders in serving Canadian military personnel. While this group had lower levels of disability relative to those with a current disorder, it still had substantial levels of disability. Hence, this is a group worthy attention in prevention and control efforts. Future research using longitudinal design is needed to study this group, with a particular focus on related occupational impacts.
Footnotes
Data Availability
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding for this work from the Department of National Defence (Canada), via salary support and a research contract with the Canadian Institute of Military and Veteran Health Research and the University of Ottawa (No. W7714-145967). This work was also supported, in part, by the Canada Research Chairs program for Ian Colman.