
Abstract
Mental health problems are prevalent in the general population worldwide [1, 2], causing a significant burden on society [1–4]. In the World Health Organization–World Mental Health (WHO-WMH) initiative, the 12 month prevalence of mental disorders varied widely from 4.3% in Shanghai to 26.4% in the USA [5, 6]. The 12 month prevalence of mood and anxiety disorders in adult populations in Beijing and Shanghai was lower than those of other countries [5, 6]. The Chinese component of the WHO-WMH initiative, however, targeted individuals aged ≥ 18 years. There is a paucity of studies investigating the epidemiology of mental health problems in Chinese adolescents.
Adolescence is a critical time for developing a robust and resilient personality. Adolescents with mental disorders are usually accompanied by low psychosocial function and academic achievement [7, 8]. Severe or chronic mental health problems are likely to impede development [9]. It is well known that mental disorders in adolescents are strongly related to the development of mental disorders in adulthood [10–12]. Thus, it is important to study the aetiology of mental health problems in adolescents so as to develop prevention and treatment strategies.
Severe psychological distress (SPD), which covers the symptoms of mood and anxiety disorders, is severe enough to cause moderate to serious impairment in social, occupational, or school functioning [2]. The causes and mechanisms of psychological distress are unknown. It has been widely recognized that mental health problems are the results of interactions of biological with psychosocial factors.
Previous studies have identified risk factors for psychiatric disorders including genetic, cognitive, temperamental, interpersonal and family environmental factors [13, 14]. It is commonly accepted that family psychiatric history [14, 15], family environment involving high discord, low cohesion and high affectionless control [16, 17], negative family interactions [18, 19], and harsh parental discipline [13] are risk factors of child pathology. Poor relationship with peers [16, 20], and feeling of lack of security [21] may increase the risk of developing mental disorders in children and adolescents. In addition, negative life events and personal temperament [14] may increase risk for depression and anxiety.
In the past years, China has been experiencing various changes in many areas and there has been tremendous improvement in people's quality of life. Few epidemiological studies, however, have been conducted to examine the mental health status of adolescents in China. The Kessler Psychological Distress Scale (K10) is an excellent screening tool to assess the current status of mental health [22]. It covers core depressive symptoms and has been shown to have good ability to detect non-specific psychiatric distress [22].
The objectives of the current study were to (i) estimate the prevalence of psychological distress in adolescents in China, and (ii) to examine the relations between a broad range of potential risk factors and psychological distress in this population. Some variables are specific to the Chinese culture.
Methods
Study population and design
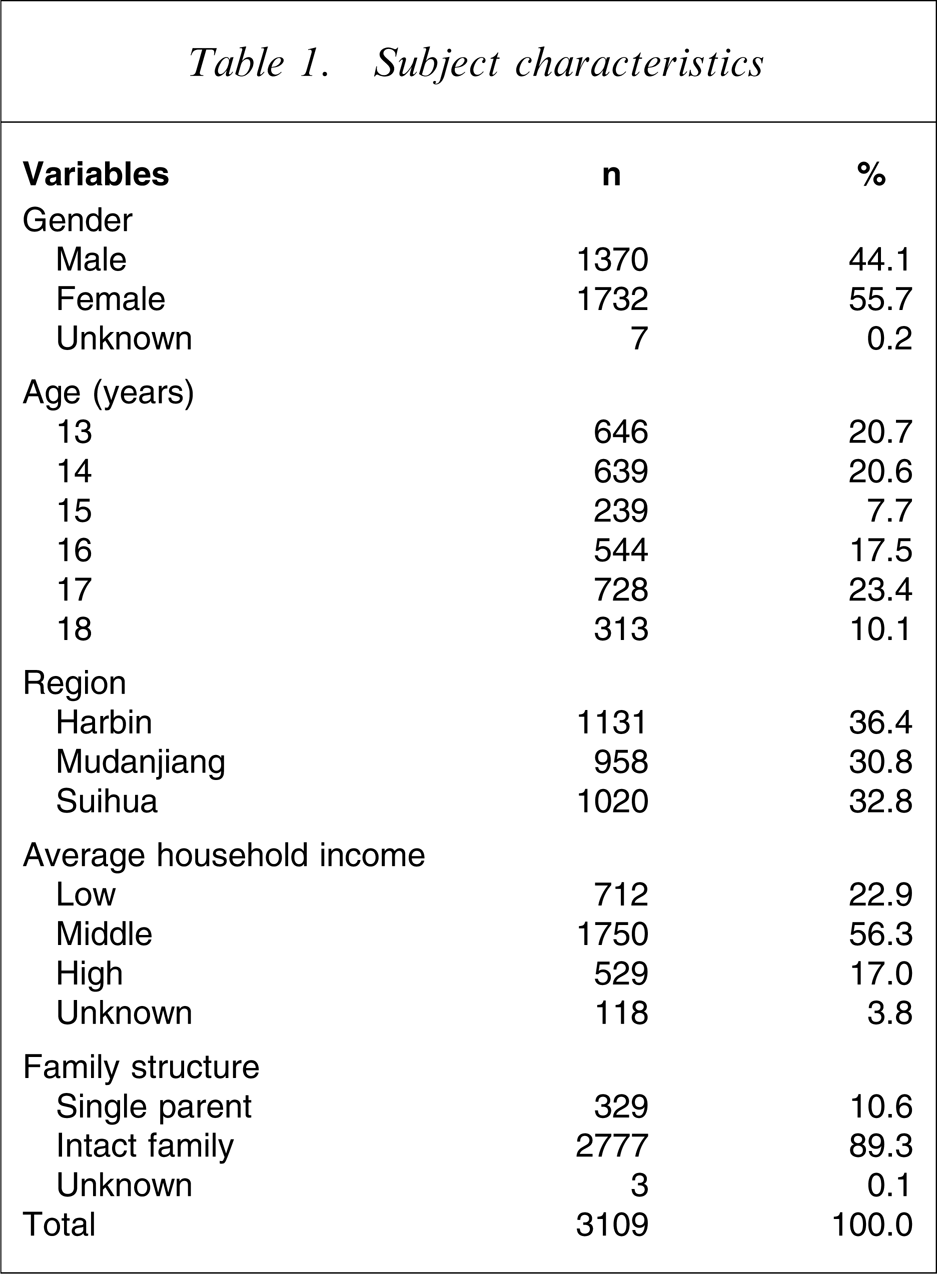
The study was conducted in Heilongjiang province, China. We used multiple-stage, stratified, clustering sampling procedures. The provincial capital is Harbin, which is the largest city of the province, with > 3 million people. There are three middle level cities with a population between 1 and 2 million (Qiqi Har, Mudanjiang and Jiamusi). For the present study we included Harbin and randomly selected Mudanjiang city. There are more than 100 county-level cities in the province. Due to the considerations of financial resources and field operation, we chose Suihua city, which is close to Harbin. In Harbin, we randomly selected a junior and a senior high school among schools in three districts, which are at different levels of education and economic development. In Mudanjiang city we randomly selected a junior school and a high school from an economically higher district and an economically lower district, respectively. In Suihua city there is only one district. We randomly chose a junior school and a high school from all the junior and senior high schools. In each of the participating schools we randomly selected two classes. All students of the selected classes were invited to participate in the study. We distributed 4324 copies of questionnaires based on the number of potential participants provided by the participating schools. At the end 4278 questionnaires were returned (98.9%). Excluding invalid questionnaires (those with systematic patterns of answers in K10 or those with >80% questions unanswered), 4096 copies remained. In the current analysis we targeted students aged 13–18 years old (n = 3109). There were 1370 boys (44.1%) and 1732 girls (55.7%). Seven questionnaires had missing information about gender. In these participants, 1457 (46.9%) were in junior schools, and the other 1652 (53.1%) were high school students. The median age was 16.0 years.
Psychiatric measures
In the present study we used the K10 to measure psychological distress. The K10 was developed by Kessler et al. to measure the clinically significant range of the distribution of non-specific psychological distress [23]. We chose this scale because it has been used in the adolescent populations in Australia [24] and in Canada [25, 26]. Therefore, international comparisons would be possible. Although the K10 was developed as a screening instrument for serious mental illnesses [23], in the present study it was used not to identify psychiatric cases, but to identify non-specific psychological distress in general.
We translated the K10 into Chinese and back-translated and pilot-tested the Chinese version in a small group of Chinese adolescents. The K10 consists of 10 questions asking about the frequency of non-specific psychological distress in the past month [22]. Each question has five answers, ranging from ‘none of the time’ to ‘all of the time’ and was scored from 1 to 5 correspondingly. The answers were recoded in reverse order, and all the items were summed to obtain a total score.
The Zung Self-Rating Depression Scale (SDS) [27], a tool to assess the severity of depressive symptoms, has been validated in adolescent populations in the USA, Japan, China and other countries [28, 29]. The 20-item SDS focuses on a range of symptoms covering emotional, physical and behavioural, cognitive manifestations of depression during the past week. An SDS score of ≥57 indicates severe depression [30]. In this study we used SDS as a supplementary tool for the measurement of psychological distress and for examining the validity of K10.
Preliminary analysis showed that the K10 scores were not normally distributed (Skewness/kurtosis = 1.03/0.94, Figure 1). Various transformations were not successful. There is no standard cut-off for K10 in adolescents. For the objectives of the present study we ran receiver operating characteristic (ROC) analysis using the SDS and the K10 scores. The ROC analysis showed that the optimal cut-off of the K10 for predicting SDS severe depression was 31 (sensitivity = 87.3, specificity = 87.5). In an adult population, a K10 score of 22 indicates severe psychological distress; in adolescents, a score of 22 might indicate temporary mood disturbance. Therefore, in the present study we defined a K10 score of ≥31 as severe psychological distress, a score between 22 and 30 as moderate psychological distress.
Distribution of Kessler Psychological Distress Scale (K10) scores in Chinese adolescents.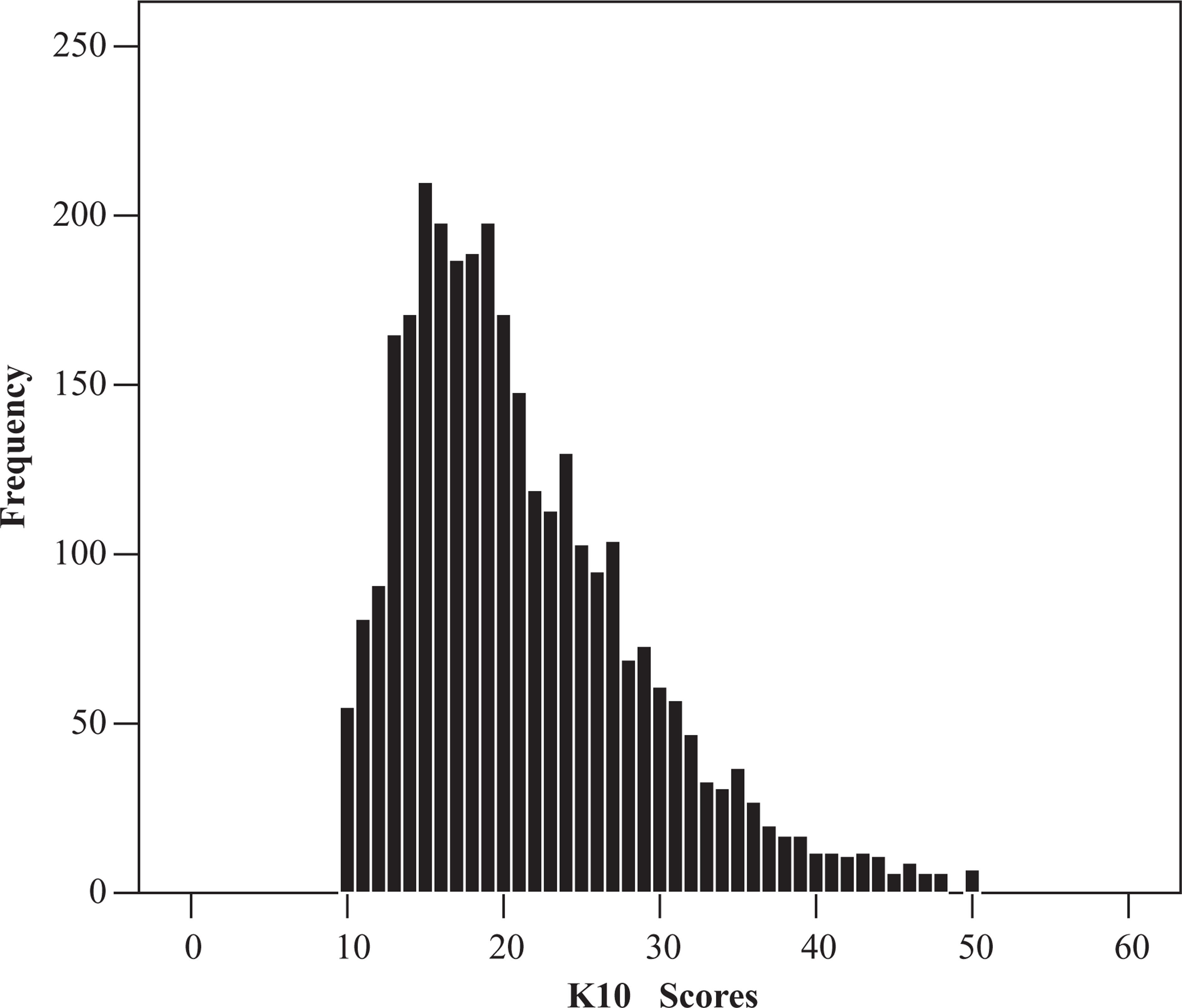
Demographic, psychosocial variables
The demographic variables included sex, age (13–18), region (three selected cities), family structure (single parent vs intact family), and average monthly household income. We defined <800 RMB as low income, 800–2000 RMB as middle income and >2000 RMB as high income, which is in accordance with the State Labor and Social Security Department [31].
Other psychosocial factors included in this analysis were as follows (questions for some constructs specific to the Chinese culture are presented in Appendix I): (i) family environment: parents quarrel frequently (no vs yes), parental educational manners (democratic (friendly, understanding), not democratic (strict, hostile, neglectful), or combined), communication with parents (always, sometimes, occasionally or never), perceived relationship with parents (good relation with both parents; good relation with one of them; poor relation with both of them), parents care about your study (really care about my study vs sometimes, occasionally care or not at all) and parental satisfaction with your study (always, sometimes, seldom, not at all); (ii) school: self-satisfaction with study (always, sometimes, seldom, not at all), perceived relationship with teachers and peers (excellent, good, average, poor, bad); (iii) self-perception: self-satisfaction with appearance and life (always, sometimes, seldom, not at all); and (iv) other variables: self-rated physical health (healthy vs not healthy), negative life events (e.g. death or severe illness of direct relatives, great conflict or divorce of parents, maladaptation under new circumstance) in the last 6 months (yes vs no) and self-reported family psychiatric history (yes vs no).
Analysis
The demographic and socioeconomic status of the sample was first examined. We calculated the percentages of psychological distress of different levels by demographic and socioeconomic factors. Bi-variable analysis (χ2 test) was done between psychological distress and the socioeconomic and psychosocial factors. Because the K10 scores were not normally distributed and transformations were not successful, we used ordinal regression analysis to estimate the associations between demographic, socioeconomic and psychosocial variables and psychological distress. The analysis was conducted using SAS 9.1 (SAS Institute, Cary, NC, USA).
Results
Subject characteristics
Prevalence of psychological distress vs demographics and socioeconomics
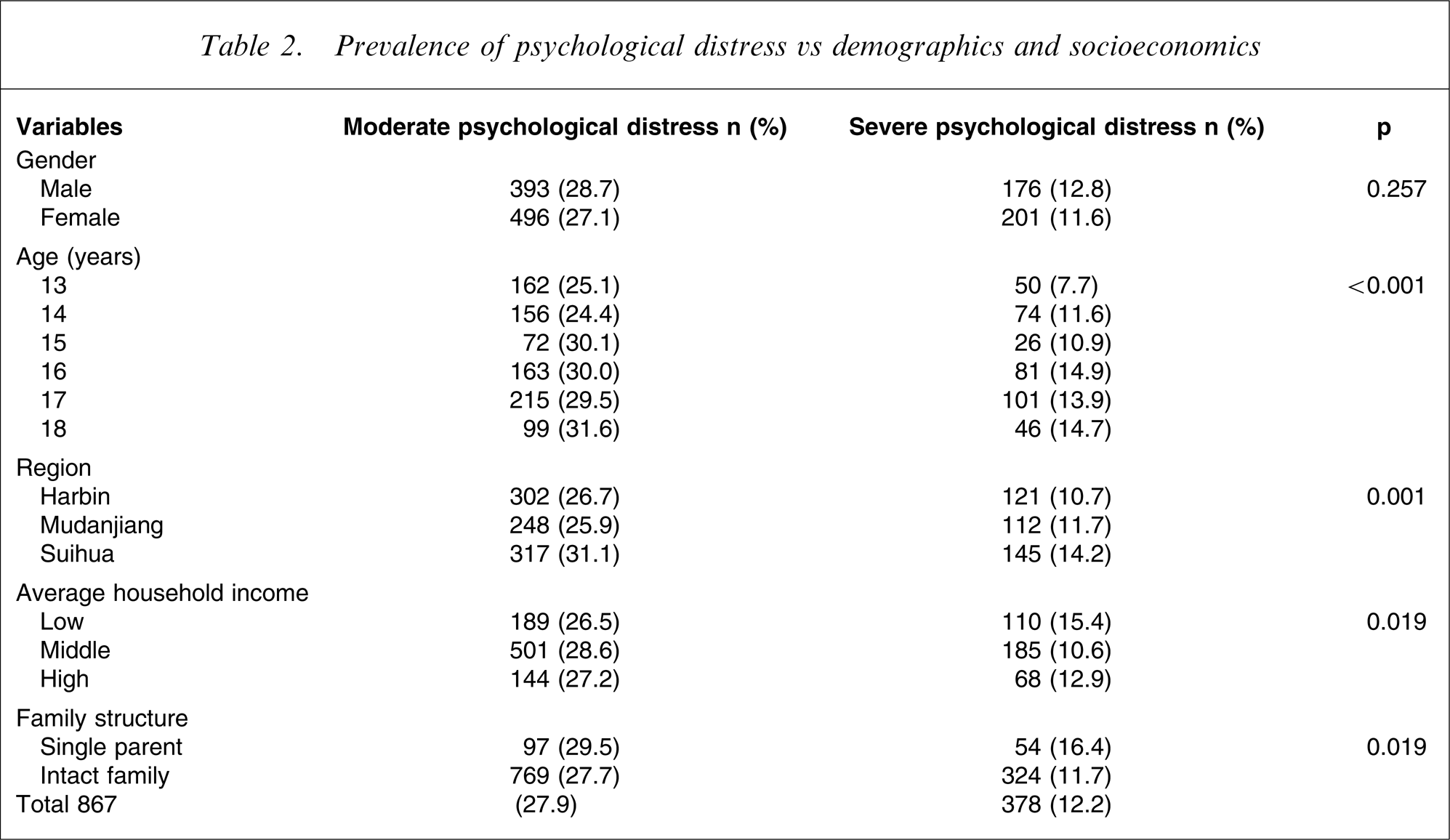
Bivariable analysis showed that there were significant differences in psychological distress by family environment variables. Schooling variables and other variables all showed strong correlation with psychological distress. The prevalence of severe psychological distress was as high as 61.5% if there was a poor relationship with peers and 55.0% if there was dissatisfaction with life. Of those who were dissatisfied with their appearance, 36.8% had severe psychological distress.
Because the psychological distress scores were not normally distributed and we classified the score into three levels, we used ordinal regression modelling to identify factors associated with psychological distress. Prior to the modelling, we examined correlations among the selected variables. Strong correlations were found between perceived relationship with peers and with teachers (r = 0.56) and between parental satisfaction and self-satisfaction with study (r = 0.46). We kept perceived relationship with peers and self-satisfaction with study in the model. We found no interactions between age and gender in relation to psychological distress, and no interactions between other variables in the analysis.
Ordinal logistic regression analysis
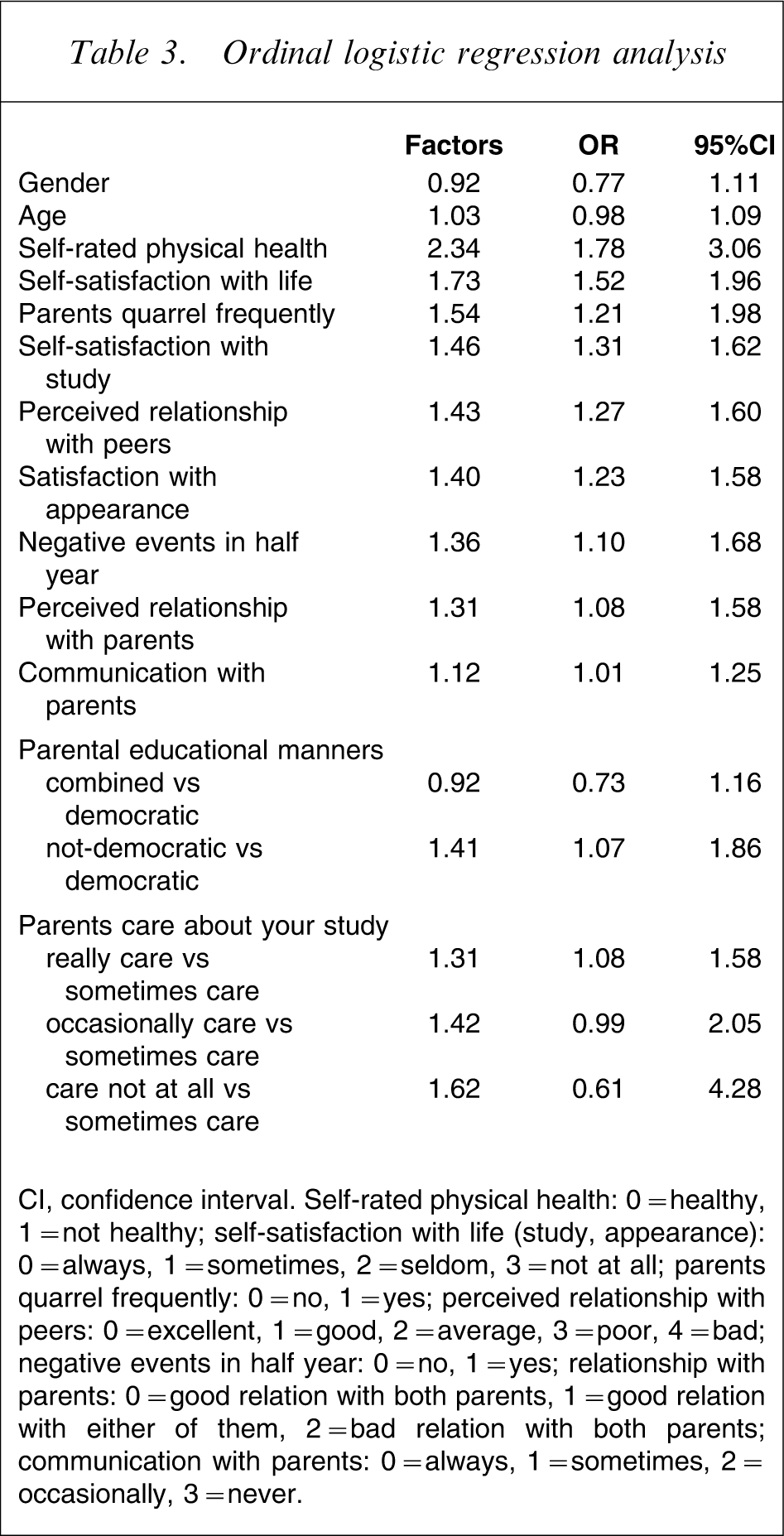
CI, confidence interval. Self-rated physical health: 0 = healthy, 1 = not healthy; self-satisfaction with life (study, appearance): 0 = always, 1 = sometimes, 2 = seldom, 3 = not at all; parents quarrel frequently: 0 = no, 1 = yes; perceived relationship with peers: 0 = excellent, 1 = good, 2 = average, 3 = poor, 4 = bad; negative events in half year: 0 = no, 1 = yes; relationship with parents: 0 = good relation with both parents, 1 = good relation with either of them, 2 = bad relation with both parents; communication with parents: 0 = always, 1 = sometimes, 2 = occasionally, 3 = never.
Discussion
The present study is one of a number of large epidemiological studies about psychological distress in Chinese children and adolescents. The present results show that a significant proportion of participants had experienced severe psychological distress and that there was no gender difference in the prevalence of psychological distress. In multivariate analysis, we found that family and school environmental factors and self-perception factors were associated with the levels of psychological distress. With reference to the observation that adolescent mental health is a growing global concern, the present study can be regarded as a timely response, because there have been few Chinese epidemiological studies on adolescent mental health, especially psychological distress.
Rates of affective symptoms have varied by region, and comparisons across culture become complicated because it may be affected by a number of factors, including social, economic, and cultural factors and methodological differences. Previous studies have suggested that Asian adolescents have a comparable rate of depressive symptoms with Western countries [32]. In the present study we found that significant proportions of Chinese adolescents reported moderate or severe psychological distress. Combining moderate and severe psychological distress in the present study, the rate (40.1%) is similar to the studies (42.3%) using Beck Depression Inventory and SDS [33]. Adolescents in the present study were born in the 1990s, when China was experiencing great economic and social change. In addition to the fact that there is only one child in each family, parents have high expectations of their children. Meanwhile, children are going through puberty, a time when they experience obvious physical and psychological changes. All these factors may explain the higher prevalence of severe psychological distress in China.
Western studies generally found that the prevalence of mental health problems in adolescent girls was higher than in boys [34, 35], whereas studies conducted in China have not been consistent with respect to the gender difference [29, 36, 37]. In the present study, male students appeared to have a higher prevalence of severe psychological distress than female students, but the difference was not statistically significant. The same was found when we stratified gender-specific rates by age and by region. In the excluded questionnaire (n = 168) there were more boys and more negative choices in psychological distress. Therefore, it is possible that the prevalence of severe psychological distress in boys could have been underestimated.
The gender difference in severe psychological distress observed in the present study is consistent with the Liu et al. study, which was also conducted in mainland China [29], and a study conducted in Deli, India [38]. Due to the large population in China, there is high competition for higher education. In contrast, Chinese people often hold such opinions that girls should be encouraged while boys should be educated and trained differently. Because of the influence of traditional culture, parents may still have higher expectations on boys than on girls in terms of academic and social achievements. Such social and family expectations may have imposed more pressure on boys than on girls, leading to an increased level of distress among boys. Biologically, the Chinese girls may be more likely to experience mental health problems than boys, but the exposure of these culturally unique psychological risk factors in the Chinese boys may have reduced the gender difference. This may partly explain why there was no gender difference in the prevalence of mental health problems in the present study, whereas such a difference was observed in studies conducted in Western countries. Nevertheless, the K10 is not a diagnostic instrument. It is not clear, based on the present results, whether there is a gender difference in the prevalence of mental disorders in Chinese adolescents.
Previous studies have shown that children in single-parent and low-income families are vulnerable to mental disorders [39, 40]. There were differences according to family income and family structure on bivariate analysis, but family income and family structure were not associated with psychological distress in the multivariate ordinal regression model. The significant difference according to family income and family structure observed on bivariate analysis might be due to the confounding effects of other variables.
Previous studies have found that family dysfunction and poor relationships with peers are strongly associated with adolescent mental disorders in either Eastern or Western countries [16, 41, 42]. The present results were consistent with this.
Different cultures and societies impose different demands on their members, with sources of stress varying across culture. For example, Chinese parents place great emphasis on children's learning and education, with success in academic pursuits being seen as a source of honour for the family. In the present study, participants whose parents ‘really’ cared about their studies were more likely to have severe psychological distress than those who reported that parents ‘sometimes’ cared about their studies. It was possible that extreme care and concern from parents about children's study and academic performance would make the students more anxious and/or depressed, especially when the students could not make significant achievements or perform at a satisfactory level.
Self-rated physical health, self-satisfaction with life, study and appearance, and perceived relationship with peers were strong correlates with psychological distress, which is consistent with previous studies [37, 41, 42]. Poor self-satisfaction with life, study and appearance may be either the risk factors or the consequences of poor mental health. Adolescents become autonomous and establish their own identity. The salience of self-perception, especially among senior high school students, highlighted the importance of appropriate parenting styles. Creating a sound environment to enhance adolescents’ confidence is very important.
Exposure to negative life events was positively associated with psychological distress on multivariate analysis, which is consistent with previous studies [37, 42]. Psychiatric history in the family was associated with psychological distress on bivariate analysis, but this factor was not significant on multivariate analysis. Although this was also reported by Lewinsohn et al. [42], given the important of family history in the aetiology of mental disorders, more studies are needed to replicate this particular result. Alternatively, there could be misclassification about family psychiatric history, for example, some students might not know that one of their family members had a mental illness. Hence, the association between family history and psychological distress could have been diluted.
There were several limitations in the present study. First, all participants were from Heilongjiang province, northeast of China. The sample might not be representative of all Chinese adolescents. Cautions is needed when the results of this study are generalized to the populations in other regions. Second, this was a cross-sectional study, so causal inferences could not be made. Third, the data were based on self-report. Thus, reporting and recall biases were possible.
Conclusions
Psychological distress is prevalent in the Chinese adolescent population. Family dysfunction, higher academic pressure, poor relationships with parents and peers and negative self-perception are important risk factors associated with psychological distress in adolescents. Studies using the K10 scale in different cultures or in the same ethnic populations living in different regions are needed so that national and international comparisons can be made.
Footnotes
Appendix I: Questions used to assess family and school environment that are specific to the Chinese culture
Parents quarrel frequently
If you live with both your biological parents, do they quarrel frequently?
1) no 2) yes
Perceived relationship with parents
You perceive your relationship with your parents as:
1) good relation with both parents 2) good relation with either of them
3) bad relation with both parents
Communication with parents
Do your parents play and communicate with you?
1) always 2) sometimes 3) occasionally 4) never
Parental educational manners
Your parents adopt the following educational manners (multiple)
1) friendly, understanding 2) strict, tough3) hostile, distrusting
4) neglectful, indifferent
Perceived relationship with peers
You perceive your relationship with your peers as:
1) excellent 2) good3) average4) poor5) bad
Parents care about your study
How much do your parents care about your study?
1) really care about my study(spend a lot of time and energy on my study)
2) sometimes care 3) occasionally care
4) they don't care at all
Parental educational manners: 1 = democratic; 2 or 3 or 4 = not democratic; 1 and [2 or 3 or 4] = combined.