
Abstract
Background:
Severe acute malnutrition (SAM) contributes to a substantial number of child deaths globally per year. The mortality rates can be lowered markedly if guideline-based management protocol is properly followed. However, case-fatality rates in resource-poor centers remain high even after introducing the guidelines. Perhaps, the lack of adequate knowledge leading to inappropriate management by the health care providers is responsible for such burden.
Objective:
We aimed to evaluate health care providers’ knowledge, attitude, and practice regarding the facility-based management of children with SAM in Bangladesh.
Methods:
This was a qualitative study where data were collected cross-sectionally from 4 district and 2 tertiary care hospitals. Twenty-six semi-structured in-depth interviews were conducted among the doctors and nurses involved in inpatient care of SAM. Twenty-eight hours of observation were done in each facility to obtain information regarding the management practices.
Results:
The doctors had substantial knowledge in managing children with SAM in the facilities. However, knowledge of nurses was found suboptimal when evaluated based on the national guideline. Both doctors and nurses demonstrated favorable attitude toward management of childhood SAM. Identification of SAM at the facilities was poor due to lack of practice in relation to anthropometric measurements. In addition, improper practices related to blood glucose testing, dehydration monitoring, essential micronutrient administration, and follow-up of children with SAM were observed.
Conclusion:
The study results underscore the importance of taking appropriate measures to enhance knowledge and ensure proper practice in relation to inpatient care of children with SAM according to the national guideline in Bangladesh.
Keywords
Introduction
Severe acute malnutrition (SAM) threatens the health of approximately 14.3 million children under 5 years of age and contributes to a substantial number of child deaths globally per year. 1 A large proportion of children with SAM resides in Asian and African countries among which Bangladesh holds a major position with more than 0.3 million children suffering from this acute form of malnutrition. 1 -3 Children suffering from SAM are more prone to develop infections resulting in an increased rate of morbidity and mortality. 4 The risk of mortality from any cause is 9 times greater in a child who is suffering from SAM compared to a well-nourished child. 5 A mortality rate of more than 20% is deemed unsatisfactory by the World Health Organization (WHO) in the management of severely malnourished children. It is, therefore, imperative to ensure utmost care of severely malnourished children in order to minimize possible complications as well as avoid fatal consequences during hospitalization. 6 However, the rate can be lowered if guideline-based inpatient care protocol is properly followed. 7 The management guidelines for SAM have been initiated during the 1970s which in turn resulted in the reduction of case fatalities to as low as 1% to 5%. 8,9 A study found that case fatality is decreased from 20% to 5% through the implementation of SAM management protocol. 10 Considering the success, the WHO recommended a guideline for facility-based inpatient management of severely malnourished children. 6 In accordance with that, Bangladesh has integrated a national SAM management guideline which is supposed to be followed by the doctors, nurses, and health care professionals involved in the inpatient management of under-five children with SAM. 11
However, in resource-poor settings, the case fatality rate (CFR) is still high despite using the treatment and management guidelines. 12 Inappropriate case management owing to poor knowledge among health care professionals including physicians and nurses can be attributed to persistent high CFR in low- and middle-income countries. 12 In addition, lack of resources, improper practice, and differences in following management guidelines may play vital roles in increasing the CFR. 13 Prior works indicate that the success and positive impact of the guidelines primarily depend on the availability of knowledgeable, skilled, and motivated health care staff in the facility. 14 It was also reported that knowledge on management guidelines and experience in managing children with SAM primarily contribute to motivation and appropriate attitude of the health care providers. 15 To that end, adequate knowledge, positive attitude, and proper practice in managing severely malnourished children as per the national guideline are imperative to reduce the CFR in resource-limited settings. Since SAM is not uncommon in Bangladesh, the physicians and nurses who work in pediatric wards are likely to manage severely malnourished children in their day-to-day practice. In this regard, they require specialized knowledge and favorable attitudes while treating children with SAM in the facilities. However, there is a paucity of research pertaining to the health care providers’ knowledge, attitude, and practice toward the management of children with SAM in Bangladesh. Therefore, we have designed this study with an aim to assess health care providers’ knowledge, attitude, and practice regarding the facility-based management of under-five children with SAM in light of the national guideline of Bangladesh. 11 The findings of the study would allow us to identify the gaps as well as the contributing factors for the deviation of the national guideline by the health care providers while treating in-patient SAM cases. It would also provide key information to formulate effective strategies in order to improve in-patient SAM management.
Methods
Study Design and Settings
This was a qualitative study where data were collected in a cross-sectional manner. Study location, settings, and participants were selected purposively. We have conducted the data collection in two administrative divisions of Bangladesh, one with the lowest prevalence of wasting (Rangpur = 7.3%) and another with the highest prevalence (Sylhet = 10.4%). 3 From each division, we have purposefully selected one tertiary care teaching hospital and two district hospitals (a total of 6 hospitals in 2 divisions). The tertiary care teaching hospitals were Sylhet MAG Osmani Medical College and Hospital and Rangpur Medical College and Hospital, respectively. The district hospitals were Habiganj District Hospital and Moulvibazar District Hospital from Sylhet division; and Thakurgaon District Hospital and Kurigram District Hospital from Rangpur division. These hospitals were selected because children with SAM are supposed to receive treatment according to the national guideline in these facilities. 11 These chosen facilities had the highest number of under-five children admissions in their respective divisions. 16 Subsequently, we have performed semi-structured in-depth interviews (IDI) of the health care professionals (doctors and nurses) in order to assess their knowledge and attitude regarding facility-based management of children with SAM according to the national guideline. Health care professionals actively engaged in the management of SAM were selected as the respondents for the interviews. In addition, we have observed the SAM management practice of health care providers in the respective SAM ward of the selected hospitals to compare the findings with information obtained from IDIs.
National Guideline for Facility-Based Management of Children With SAM
The national guideline is intended for physicians, nurses, and other health care workers who are responsible for the clinical and dietary management of children suffering from SAM admitted to a hospital for inpatient care. Children with SAM who are burdened with medical complications, for example, infection or bilateral pedal edema, are candidates for inpatient facility-based management. On the other hand, children without any medical complications apart from being severely malnourished are eligible for community-based care. 11 The facility-based management is divided into 2 major parts, the initial acute phase management or stabilization phase, and the rehabilitation phase. The acute phase management prioritizes cautious frequent feeding, preventing or treating hypoglycemia and hypothermia, rehydrating a dehydrated child with close monitoring for indication of fluid overload, correcting electrolyte and micronutrient deficits, and prescribing broad-spectrum antibiotics routinely. 11 The rehabilitation phase emphasizes restoring lost body tissue, providing sensory stimulation, and preparing for discharge and follow-up. This comprises a total of 10 steps of management. The study mainly focuses on the first 7 essential steps which are routinely followed in hospital settings (Figure 1).
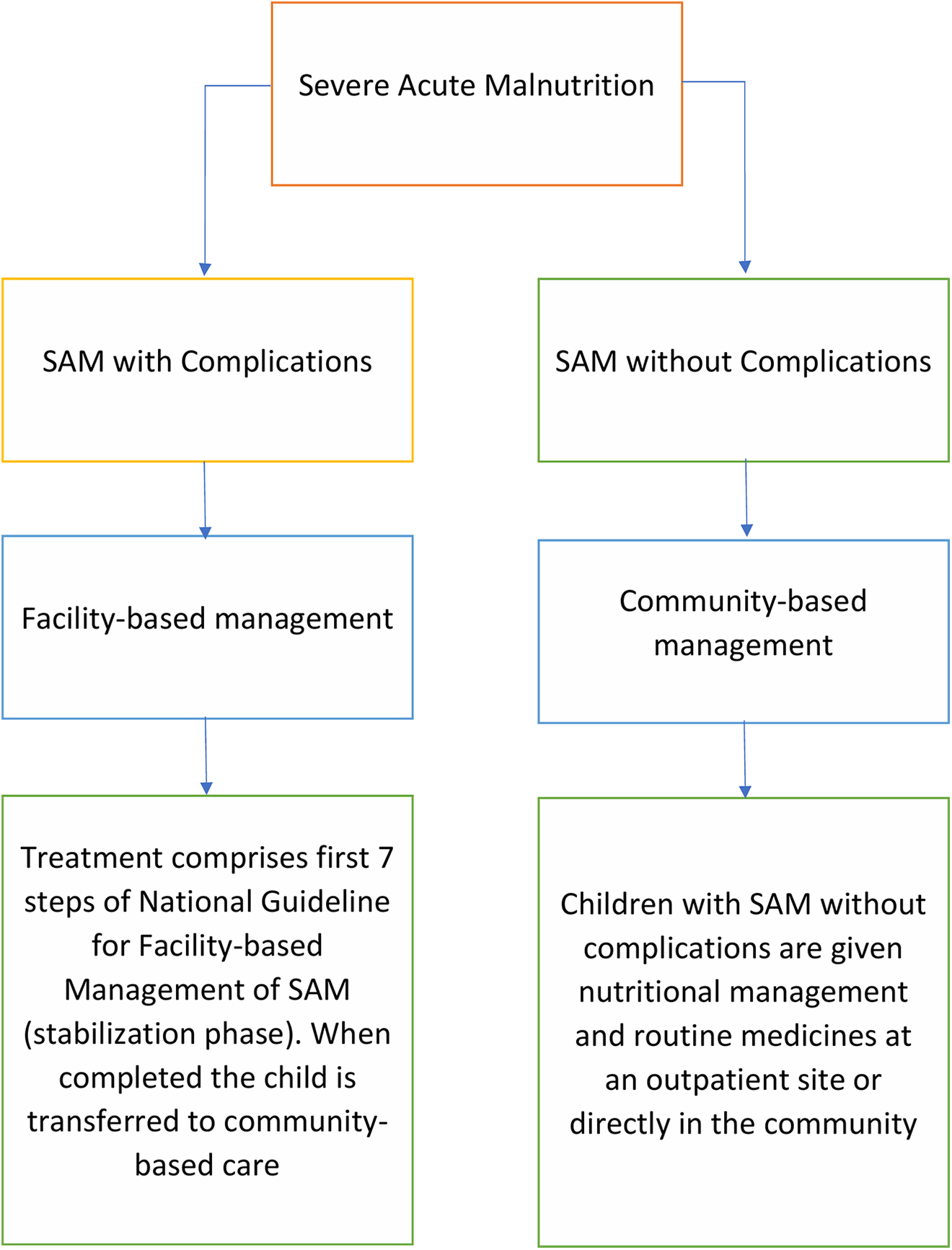
Flow of chart showing the management of severe acute malnutrition according to the national guidelines of Bangladesh.
Data Collection
All the data were collected between September 2020 and January 2021 by the study investigators. A research team with adequate experience in facility-based management of SAM constructed the interview guides and preinterview questionnaires. Interview guides were prepared based on semi-structured questionnaires as different parts of the research issue were focused on by a planned series of open-ended questions. The preinterview questionnaire extracted sociodemographic information and interview guidelines for the IDIs targeted the existing knowledge on identification of SAM, first 7 steps of facility-based management of SAM, and the national guideline itself; attitude of health care providers regarding their responsibilities; and practice of health care providers in relation to the facility-based management of under-five children with SAM. All interviews were conducted by 2 interviewers where one facilitated the interview and another recorded the interview and took necessary notes. An observation checklist for assessing the management practice of health care providers was developed to methodologically triangulate data on the practice of health care providers. The observation checklist was pretested in a hospital facility in Dhaka, Bangladesh.
Analysis and Data Handling
The interviews were transcribed by 2 research team members. Directed content analysis method was used for generating codes for our analysis. Codes were defined before and during data analysis to assess knowledge and practice. For assessing attitude, conventional content analysis was utilized as codes were defined during data analysis. Initially, data were scrutinized and cleaned by the researchers to improve the quality of data. It also helped to comprehend the dimensions and structure of the data. Subsequently, they generated codes to assess knowledge, attitude, and practice on the basis of the national guideline. A coding plan was devised to apply to the overall data to make sure that coding is done rigorously. For discussion and evaluation of developed codes, research meetings were convened on a weekly basis all through the coding phase. A matrix display was generated for each descriptive code containing the relevant section from the raw transcript for each participant. Data were interpreted from each matrix and the coded data were evaluated to look for relevant themes. Codes that digressed from the goal of the study were kept separate. Only the codes which were found to be consistent with the data were evaluated as valid and the themes that emerged were named and delineated. The criteria to assess each theme was decided upon relying on the national guideline and raw data. 11 Finally, to meaningfully represent the data, data were quantified and presented in a table. In order to thoroughly assess the knowledge of the health care providers, 8 criteria were selected based on the national guideline which addressed the diagnostic features of a severely malnourished child along with the identification and management of hypoglycemia, hypothermia, dehydration, electrolyte imbalance, infection, micronutrient deficiencies, and feeding management (Table 1). 11
Criteria for Assessing the Knowledge of Health Care Providers According to the National Guideline.
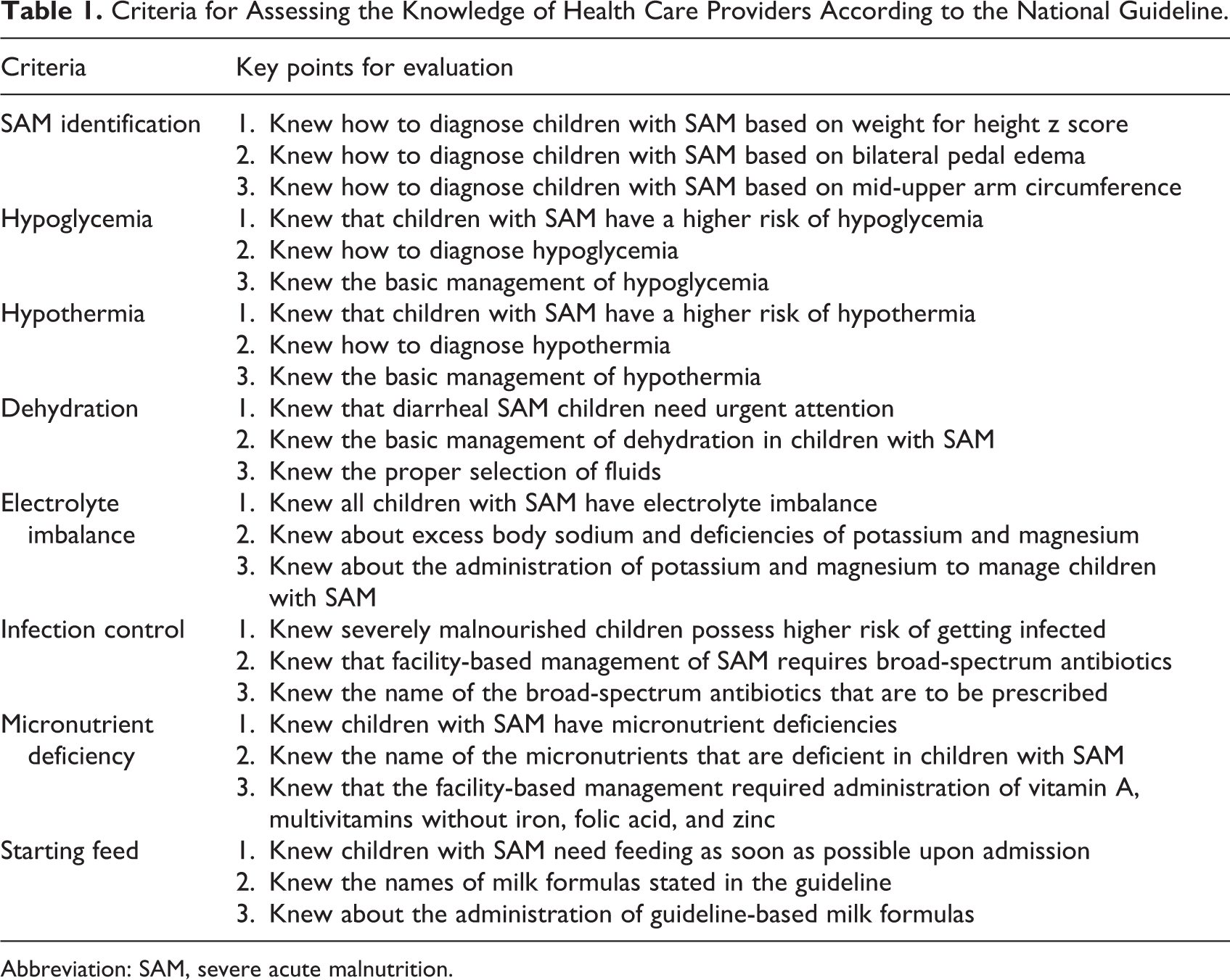
Abbreviation: SAM, severe acute malnutrition.
Three different key points were evaluated under each criterion (Table 1). Knowledge of the health care providers was assessed based on the specific 3 essential points for each criterion. Those who were able to mention all 3 of the points properly were considered to have “Adequate knowledge” for that criterion. Similarly, the respondents who were able to mention 2 out of the 3 points properly were considered to have “Average knowledge” and those who were able to mention only one point properly were considered to have “Poor knowledge.” The participants who were not able to mention a single point properly were considered to have “No knowledge” (Table 2).
Health Care Provider’s Knowledge Regarding Facility-Based Management of Children With SAM.
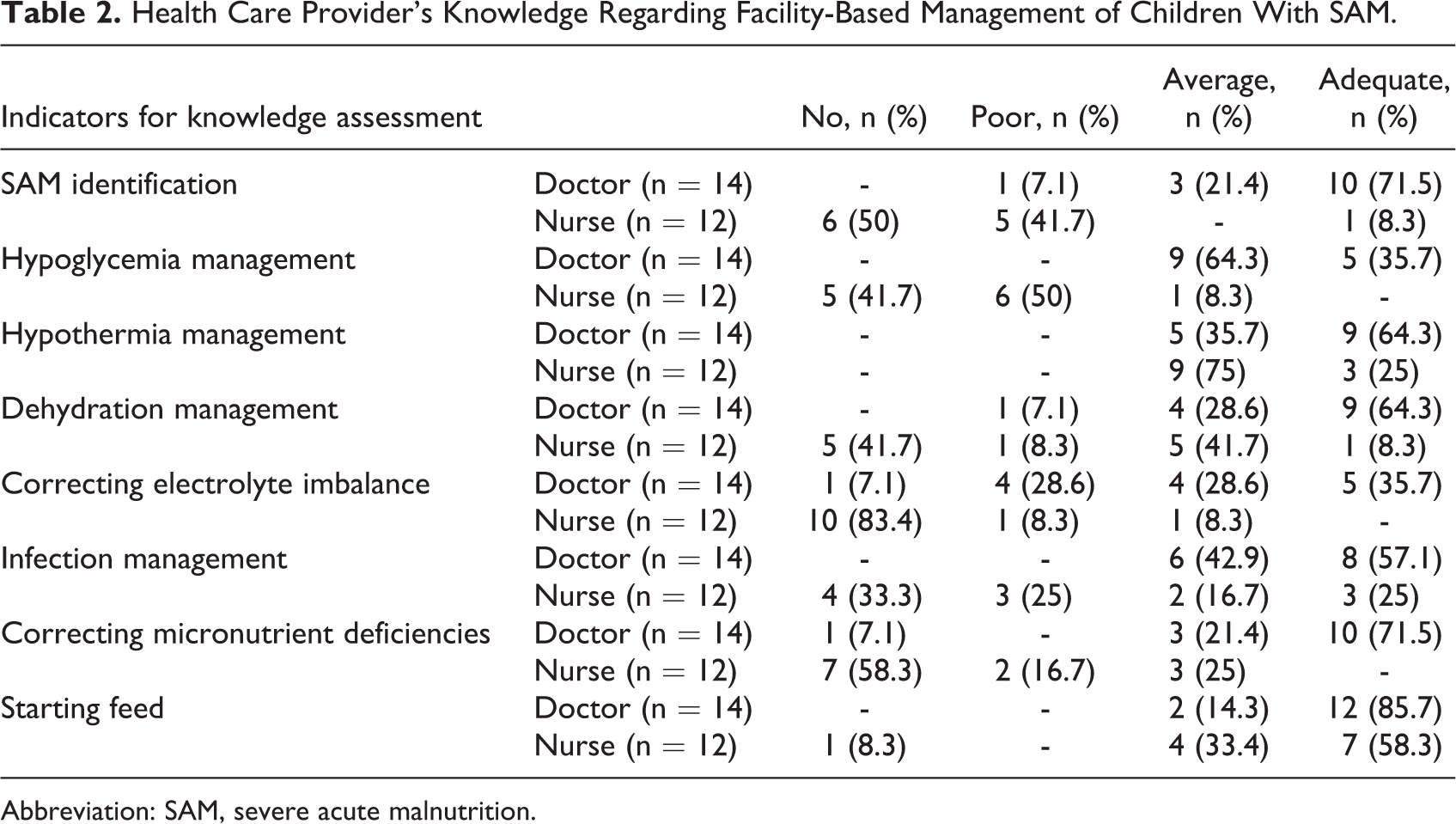
Abbreviation: SAM, severe acute malnutrition.
For assessing the attitude of the health care providers regarding the treatment of SAM, the investigators generated 5 codes after reflecting on the transcripts. The codes shed light on the respondent’s attitude toward their colleagues, counseling caregivers, intention to follow the national guideline, treating patients, and working in the ward. If the responses were interpreted to be favorable toward the criteria, they were marked as “positive” and the opposites were described as “negative.” This binary classification of attitude was used following previously published literature. 17,18
In order to document the practice of the health care providers, the investigators generated 20 codes based on the national guideline for facility-based management of children with SAM. The reported practices were reviewed and quantified on the basis of “yes” and “no.” Observation data from the wards were used to methodologically triangulate the data constituting of responses of health care providers regarding their practices in relation to the management of SAM.
Results
In total, 26 IDIs were conducted in the designated sites. Among the interviewees, 14 were doctors and 12 were nurses. Most of the participants were aged between 31 and 40 years, and 73% of the respondents were female. Only 7 respondents received training on facility-based management of children SAM. The sociodemographic characteristics of the interviewees are described in Table 3.
Summary of Sociodemographic Characteristics of Participants.
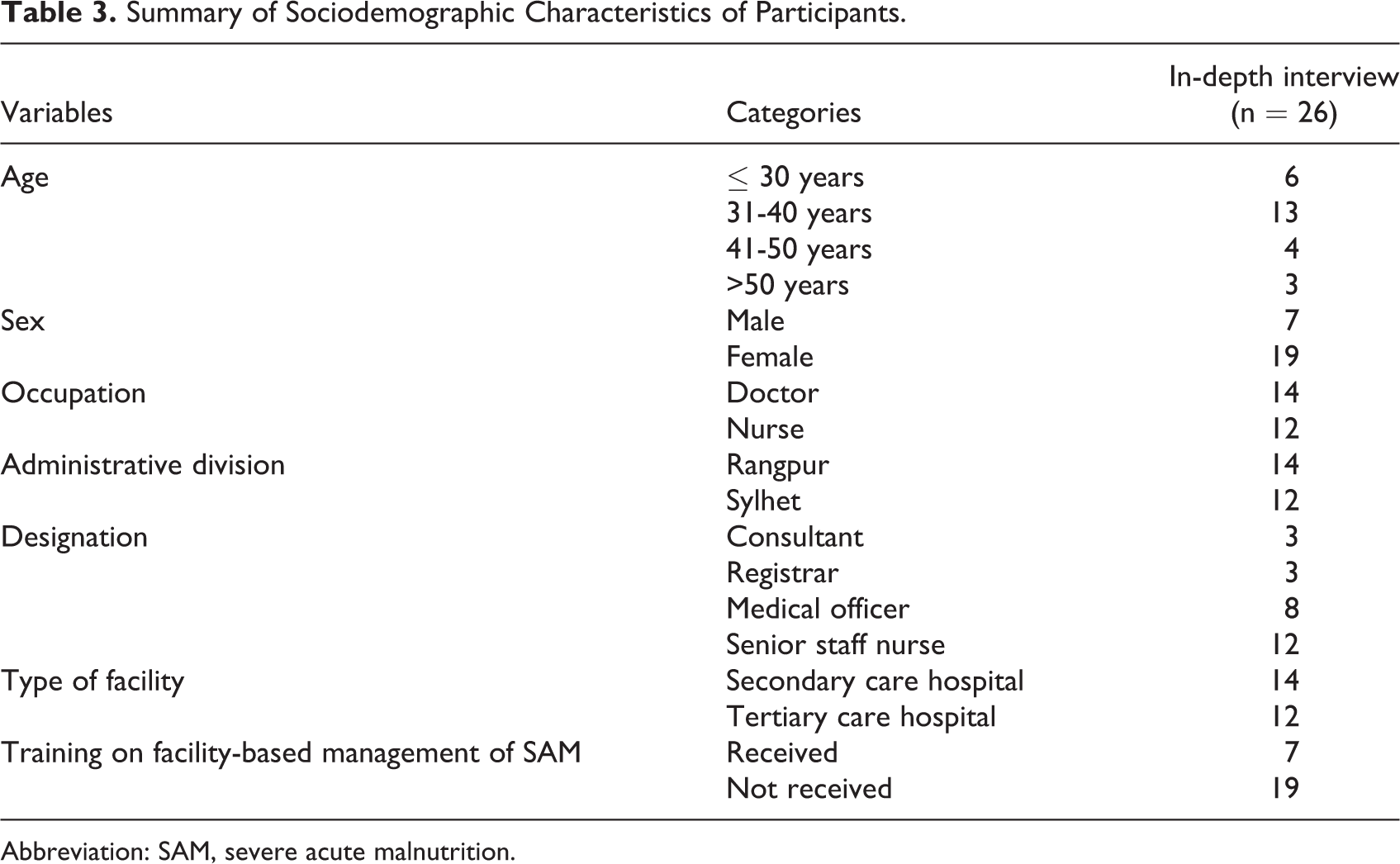
Abbreviation: SAM, severe acute malnutrition.
Knowledge of Health Care Providers in Facility-Based Management of Children With SAM
The study showed that doctors had substantial knowledge regarding the management of children with SAM in the facilities. A few of them failed to provide information on the correction of electrolyte imbalance and micronutrient deficiencies in children with SAM. Nurses had relatively poor knowledge when evaluated based on the national guideline for facility-based management of SAM. Knowledge regarding SAM identification, hypoglycemia management, dehydration management, correction of electrolyte imbalance, infection management, and correction of micronutrient deficiencies were found inadequate among nurses (Table 2). Facility-based management of the presenting conditions of children with SAM as per the national guideline are highlighted in Table 4.
Facility-Based Management Practices of Children With SAM as per the National Guideline.
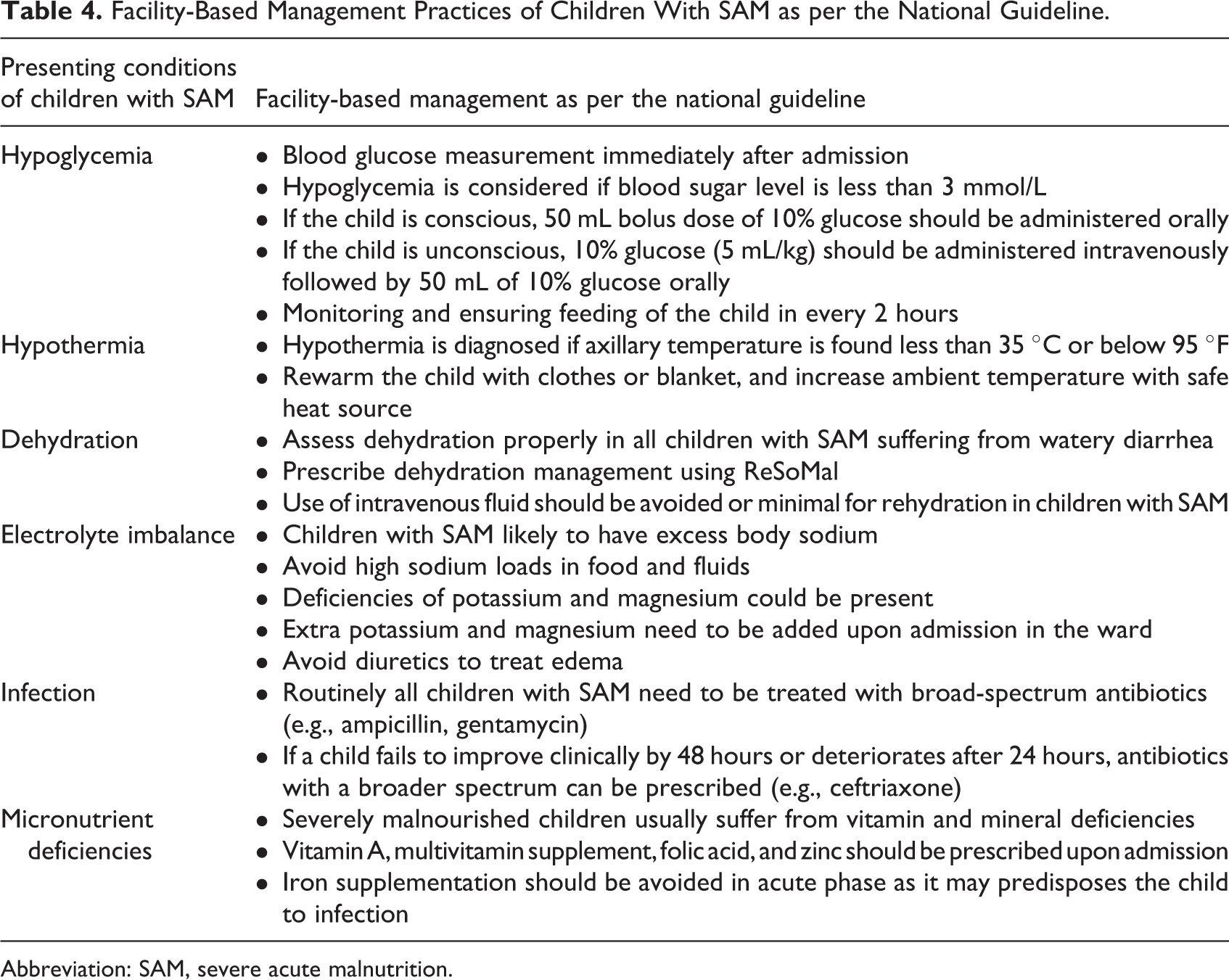
Abbreviation: SAM, severe acute malnutrition.
On the subject of SAM identification, doctors possessed a higher level of knowledge compared to nurses. Following responses from a doctor and a nurse give a reflection on the differences of knowledge between them.
A Doctor’s response, “We actually divide the diagnostic criteria into 2 groups, below 6 months and 6 months to 5 years. For below 6 months, we look for visible wasting, weight-for-length z score minus 3 standard deviation, bipedal edema; we admit a patient who has any one of these. For the patients who are aged more than 6 months, we look for MUAC less than 115 mm, weight for height less than 3 standard deviation, or bipedal edema; we admit a patient who has any one of these.” (Participant 16) “To identify SAM, we look for a child whose body is swollen, head is little bigger, sometimes they have little bit of loose motion, temperature…we identify them depending on those. Weight may be bit more than usual, again sometimes little less than usual, according to the age….” (Participant 20) “For hypoglycemia, we examine whether the child is conscious upon arriving, if he is conscious and able to tolerate feed…if sugar less than 3 we call that hypoglycemia. In that case, we give him NG tube feeding with 10% DA…that is 5 mL per kg…which is the first step. If the patient cannot tolerate, we can go for injectable. After that we start F-75 diet, half hourly for 2 hours we complete a feed, after that…I mean…if he gets settled then we start giving feed 2 hourly” (Participant 18) “In case of hypoglycemia…I mean we manage everything the same. I mean there is no separate care for hypoglycemia.” (Participant 13) “For dehydration…we directly introduce intravenous saline, if we recognize dehydration, we introduce saline, glucose….” (Participant 12) “Maybe…sometimes we give intravenous injection….” (Participant 25) “We do not prescribe them initially. After control, we provide multivitamin, folison, and Iron…. If we see that the child is in control, we give them these during discharge…for 3 months….” (Participant 14)
Attitude of Health Care Providers Toward Facility-Based Management of Children With SAM
Both the groups of health care providers had positive perspectives on the subjects of working with colleagues, approach toward routine activities in the ward, treating SAM patients, counselling their caregivers, and the intention to follow the national guideline. Only one of the nurses had a negative attitude toward working in the ward. The response was, “There are lots of problems, like we have to talk to patient’s attendants…. They can’t understand as they are from rural areas, even when we speak with them politely, they don’t want to cooperate. They return frequently to me with the same issues….” (Participant 10)
Practice of Health Care Providers in Facility-Based Management of Children With SAM
Health care providers interviewed in this study reported their usual practices in terms of management of children with SAM in their respective facilities (Table 5). Subsequently, 28 hours of observation was conducted in each of the selected hospitals to observe the practices in managing children with SAM. Facility-based management was observed in one tertiary teaching hospital as no patient with SAM was admitted to other facilities during the time of the visit of the investigators. While observing the practice, we found substantial deviation from standard protocol regarding the diagnosis of SAM. Measurement of weight, height, and mid-upper arm circumference was not practiced widely. Although more than 70% of the participants reported that they measure weight and length, it was not noticed during observation. The practice of calculating z scores and examining the edema for the purpose of diagnosing severely malnourished children were not evident as well. The admitted patients did not have weight, height, or calculated z scores documented in their hospital files or SAM register books. SAM was diagnosed on the basis of their appearance or if the child had visible wasting. A similar pattern was observed in the other 5 hospitals.
Practice According to the Facility-Based Management Guidelines of Children With SAM.
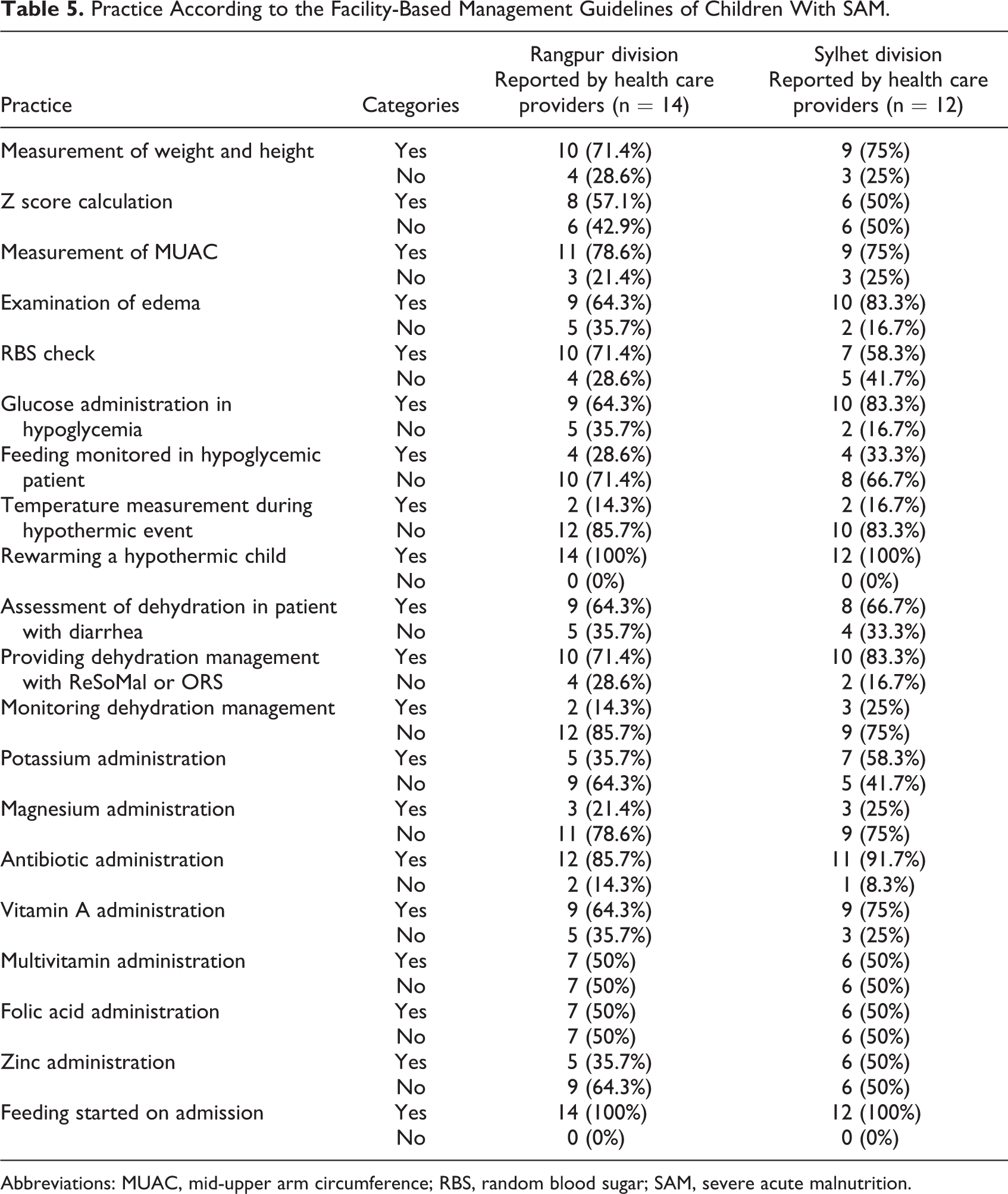
Abbreviations: MUAC, mid-upper arm circumference; RBS, random blood sugar; SAM, severe acute malnutrition.
In the observed tertiary care hospital, random blood sugar checking was not practiced as the pediatric ward did not have any glucometer. Assessment of dehydration and use of oral saline were observed in children with SAM. However, dehydration monitoring was not observed. Broad-spectrum antibiotics, potassium, vitamin A, multivitamin supplement, folic acid, and zinc were administered to the patients. Magnesium was not prescribed during the visit of the study team. Cautious feeding was started on admission. We have also observed that temperature was recorded in 2 out of 4 patients on admission. Respiratory rate was not counted, albeit physicians preferred auscultation with a stethoscope. Day-to-day anthropometric follow-up was not a common practice to monitor the nutritional progress of the child. Feeding history was taken by the health care providers and the mother was taught about basic nutrition practices. Mothers of children who were receiving some dehydration management were taught about oral saline preparation and feeding.
Discussion
The present study evaluated health care provider’s knowledge, attitude, and practice regarding facility-based management of children with SAM according to the national guideline of Bangladesh. The doctors had substantial knowledge in managing children with SAM in the facilities. Nurses’ knowledge in managing severely malnourished children admitted to hospitals was found to be inadequate. However, they demonstrated a positive attitude toward the management of children suffering from SAM.
We found that most of the nurses failed to mention properly the key identifying points of a severely malnourished child. This makes the diagnosis of SAM difficult on admission with the possibility of misplacing a child with SAM in the facility. The importance of knowing the proper diagnostic criteria is imperative as without this knowledge it would be impossible to reduce the CFR of SAM in hospital settings. 6,19 Moreover, appropriate knowledge of the nurses in managing severely malnourished children is crucial to ensure effective service delivery as they are the primary care staff in the hospital settings. 20,21 In this study, we found inadequate knowledge of nurses on some essential factors, for instance, hypoglycemia, dehydration, infection management, correcting electrolyte, and micronutrient deficiencies. In addition, the administration of intravenous fluids without severe dehydration was reported in our study. Introducing intravenous fluids in absence of proper indications carries the risk of fluid overload in malnourished children with compromised cardiological structure and reduced functionality. 22 A study conducted in Ghana observed that 70% of the nurses did not know that it is not recommended to use standard oral saline to manage dehydration in severely malnourished children which is similar to our findings. The study results emphasized adequate training as well as awareness of guidelines to make the knowledge of the nurses desirable. 23 Evidence suggests that nursing performance is directly related to their competencies which can be improved through education and training. 24 However, the number of nurses who received training on facility-based management of children with SAM was found low in our study. Perhaps, such lack of training is primarily responsible for the poor knowledge of the nurses. Several studies have pointed to the fact that nursing institutions do not provide required priority on nutrition training henceforth explaining the undesirable knowledge of nurses regarding malnutrition management. 15,25 Although the number of physicians who received training was low as well, their experience and academic knowledge may have contributed to the better scoring in this regard.
In our study, the nurses scored better in topics related to hypothermia management and feeding of malnourished children. A study conducted in the United Kingdom found that nurses possess better knowledge regarding the feeding of children. 26 They hypothesized that this outcome was due to the motivation to learn about new feeding guidelines which the nurses may want to apply to their own children. In resource-limited settings, nurses are responsible for guiding parents or caregivers regarding feeding decisions due to a lack of manpower. Such involvement for a long duration of time may enhance the knowledge of the nurses regarding the feeding of malnourished children. Moreover, the general perception that an underweight child requires proper nourishment and a hypothermic child needs rewarming could be the reason to score better in these two particular aspects despite scoring lower in other points.
Our study results revealed a positive attitude of health care providers toward the management of severely malnourished children. All the respondents acknowledged the importance of properly notifying the caregivers about their child’s condition. They were also aware of counselling the parents regarding their role in the management of sick children. It is evident that proper counselling can change a mother’s view on nutritional assessment and acceptance of newer food preparations. 27 The care providers also admitted the importance of a guideline to treat these vulnerable groups of children with a positive attitude to follow the guideline properly. These findings correspond to the results of earlier studies where they found nurses to have highly positive attitudes toward the management of malnourished children. 15,23
We observed that anthropometric measurement and z score calculation were not routine practices in any of the facilities. Precise anthropometric measurement is imperative in order to identify a child with SAM in hospital settings so that immediate guideline-based treatment can be initiated. It was reported in a study that diagnosis of SAM was being made based on clinical suspicion alone resulting in an inappropriate identification of malnourished children with high-risk status. 28 Another study documented that inadequate recording of weight and height in a children’s hospital contributed to inaccurate diagnosis of malnutrition cases. 29 Anthropometry is a simple, reliable, and noninvasive technique to identify the possible cases of SAM timely. 30 Improper practice related to anthropometry causes misdiagnosis which limits the management as per the national guideline. The importance of z score calculation lies not only with wasting of a child but with stunting and underweight as well. In case a child is suffering from all these 3 forms of nutritional deficits, the risk of mortality rises exponentially. 31 It is impossible to determine the accurate nutritional status of a child without measuring anthropometry and calculating the z scores. However, overburdened staff, insufficient training, lack of functioning instruments, increasing patient load, and the current pandemic situation may have contributed to the findings related to anthropometric measurements and nutritional status assessment in this study. 28
Our study has several limitations. Observation data of inpatient care by the health care providers were collected from one tertiary level hospital as no patients with SAM were admitted in other facilities at the time of data collection and observation. It is, however, possible that the diagnosis of some patients might have been missed at those institutions as we have observed inconsistency in anthropometric measurements. Nevertheless, limited data confined us to thorough analysis and triangulation between all the hospitals. Another important limitation is the cross-sectional nature of the study representing data collection in a single point of time. As a consequence, it does not reflect any changes in respondents’ knowledge, attitude, and practice over time in relation to the management of SAM according to the national guideline. Despite the limitations, the findings of this study provide important information regarding knowledge, attitude, and practice of health care providers toward management of SAM following the national guideline.
Conclusions
The study results illustrate suboptimal knowledge of nurses in the management of severely malnourished children admitted to the hospitals along with issues related to diagnosis of SAM using anthropometric measurements. The study results underscore the importance of taking appropriate measures to enhance knowledge and ensure proper practice in relation to inpatient care of children with SAM according to the national guideline, especially for nurses involved in management of children with SAM. Anthropometric training should be arranged to improve the identification of children with SAM. In addition, health care providers should be trained properly to practice daily growth monitoring during the hospital stay of the malnourished children. Refresher training on facility-based management guideline, both for doctors and nurses, is recommended to organize on a regular interval. Finally, policy makers, stakeholders, and concerned authorities should formulate effective policies to address the issues related to inadequate knowledge and practice regarding facility-based management of SAM in order to reduce the CFR and improve the quality of care in hospital settings.
Footnotes
Authors’ Note
MRI, SMF, MJR, and TA conceived and designed the study. MRI, SMF, and NMA collected and analyzed the data. MRI, SMF, and MGR interpreted the results and wrote the manuscript. SMF, MGR, NMA, MMIB, and TA critically reviewed and edited the manuscript. All the author(s) read and approved the final manuscript for submission. Data related to this manuscript are available upon request and for researchers who meet the criteria for access to confidential data may contact Ms. Armana Ahmed (![]() ). The study was approved by the Institutional Review Board (IRB) of International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b). Further approval was collected from National Nutrition Services (NNS), Government of Bangladesh, in order to conduct the study. Written informed consent was collected from the interview participants and the Director/Superintendent of the respective facilities to complete study interviews and observation procedures.
). The study was approved by the Institutional Review Board (IRB) of International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b). Further approval was collected from National Nutrition Services (NNS), Government of Bangladesh, in order to conduct the study. Written informed consent was collected from the interview participants and the Director/Superintendent of the respective facilities to complete study interviews and observation procedures.
Acknowledgments
We thank the interviewees and all staff members of the study who were involved in data collection. This study was funded by core donors who provide unrestricted support to icddr,b for its operations and research. Current donors providing unrestricted support include the Governments of Bangladesh, Canada, Sweden, and the United Kingdom. We gratefully acknowledge our core donors for their support and commitment to icddr,b’s research efforts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the core donors of icddr,b under the Rainy Day Grant Fund Policy for Young Scientists.