
Abstract
Background:
The problem of severe acute malnutrition (SAM) among < 5 years old (U-5) children in Bangladesh is awful with higher risk of death or morbidities. However, there is no nationwide program where these children are managed with take-home therapeutic/supplementary food as recommended by World Health Organization.
Objective:
This study aimed to identify the changes in nutritional status and morbidities over 3 months of U-5 children having severe wasting (ie, SAM) whose parents refused to admit their children in the residential nutrition rehabilitation unit of the Dhaka Hospital of icddr, b (an international health research Institute based in Dhaka, Bangladesh), and instead attended the nutrition follow-up unit (NFU), and thus did not receive any food supplementation during nutritional rehabilitation.
Methods:
At the NFU, these SAM children on every visit (fortnightly to monthly) received health and nutrition education, multivitamins, zinc and iron supplements, and treatment of illnesses if any.
Results:
During the study period, a total 180 U-5 SAM children came regularly for NFU visit for at least 3 months, and they comprised our study sample. Their age at first NFU visit (baseline) was 13.4 ± 7.8 months and 46% were female. Over these 3 month follow-up period, the rate of weight gain was 2.2 ± 1.9 g/kg/d, change in mid upper arm circumference was from 105 to 115 mm, and change in weight-for-length or weight-for-height z-score was from −2.70 ± 0.94 to −1.95 ± 1.00. During the prior 14 days to the 4 NFU follow-up visit, 13.6% to 22.8% had common cold and/or cough, and 12.2% to 15.1% had pneumonia.
Conclusion:
Because the rate of weight gain was far below the expected ∼5 g/kg/d, the NFU visits without food supplementation are insufficient in terms of catchup growth. Thus, additional efforts are required to improve the management of these SAM children for their catchup growth.
Introduction
Worldwide approximately 13.6 million children aged < 5 years (U-5) have a very severe form of undernutrition, that is, severe wasting 1 (weight-for-length or height z-score [WHZ] < −3); this condition is also known as severe acute malnutrition (SAM). 2 Wasting accounts for 4.7% of all deaths among U-5 children. 3 Owing to heightened association with morbidity and mortality, childhood wasting requires urgent attention from policy-makers and program implementers. Severely wasted U-5 children are approximately 11 times more likely to die than their healthy counterparts 4 and severe wasting is responsible for up to 2 million annual deaths globally. 5 The majority of all moderately (69%) and severely (71%) wasted children live in Asia. 1 Like other low- and middle-income countries, the prevalence of wasting is still considerably high (8% including 1.5% severe wasting) among all U-5 children in Bangladesh. 6
There are very few nutrition follow-up services/units taking care of these severely wasted/SAM children, and there is no active nationwide program in Bangladesh where these severely wasted/SAM children are managed with take-home supplementary or therapeutic food as recommended by World Health Organization (WHO). 2,7 Many of the severely wasted/SAM children in Bangladesh are not properly screened/identified and unfortunately do not receive any standardized management. Thus, the information is lacking on catchup growth and morbidities during the rehabilitation period (that usually takes around 3 months) of these severely wasted/SAM children managed in the community with or without food supplementation.
The Dhaka hospital of icddr, b runs a residential nutrition rehabilitation unit (NRU), and an outpatient-based nutrition follow-up unit (NFU). U-5 children having severe wasting or nutritional edema, that is, SAM, are managed in the NRU. Children with severe underweight (weight-for-age z-score [WAZ] < −3) and/or moderate wasting (WHZ < −2 to −3) are served on an outpatient basis from the NFU. 8 The NFU also provides services to SAM children (severely wasted children with WHZ < −3 or mid-upper-arm-circumference [MUAC] < 115 mm who refuse NRU admission 9 ). This study aimed to identify the changes in nutritional status and morbidities of U-5 children with severe wasting/SAM over 3 months attending the NFU.
Methods
This was a descriptive study with the data retrieved from the follow-up record of the U-5 children having severe wasting/SAM reported to the NFU of the Dhaka Hospital of icddr, b. With limited resources, the NFU is primarily serving the relatively less malnourished children discharged from the hospital, thus no food supplementation is provided other than micronutrient supplementation. At the time of discharge from hospital, the undernourished children were requested for follow-up visits at the NFU initially after 14 days from discharge and then monthly until the children attain the WHZ ≥ −1. During each follow-up visit at the NFU growth monitoring, health and nutrition education, clinical check-up, treatment of child’s morbidity, and ration of micronutrient (zinc [10 mg/d] for ∼ 15 days, multivitamin drop [1 mL/d] for ∼1 month, and iron [3 mg elemental/kg/d] for ∼ 2 months) supplementation were provided for oral administration without any food supplementation. 10,11 During the follow-up visits, children’s weight, length, and mid-upper-arm-circumference (MUAC) were measured using standard procedure, children with suspected comorbidities were assessed by a medical doctor and treated accordingly.
At each follow-up, the health assistant (HA) measured the children’s weight, using a digital scale with 10 g precision (Seca, model-345); recumbent length for < 2 years old children or who could not stand, and standing height for ≥ 2 old children was measured to the nearest mm, using a locally constructed length/height board. MUAC was measured to the nearest mm with a nonstretchable insertion tape. During each follow-up visit, immunization (according to the National Guidelines of Bangladesh 12 ) and deworming of the children, counseling of parents on birth spacing and contraceptives services were provided from the NFU free of cost, mothers/caregivers were given structured lessons (standardized previously) by HA on the causes and prevention of malnutrition, the importance of breastfeeding, preparation of nutritious low-cost diets with locally available food ingredients, home management of diarrhea, use of safe water and hygienic practices, and counseling on birth spacing. The HA recorded child’s morbidity (if any) that occurred during past 2 weeks at each follow-up visit. In addition, self-referral of the children at any time and day was encouraged for intercurrent illnesses.
Data Analysis
Data were entered and analyzed using SPSS for Windows (version 20) and WHO Anthro software (version 3.2.2 WHO). Descriptive statistics were generated for all measurements. Baseline and end-line data (continuous variables) of the same children were compared by paired t test. Differences in proportions were compared by χ2 test. A P value of less than .05 was considered statistically significant.
Results
During the study period, a total 180 U-5 children having SAM but the mother/caregiver refused NRU admission and thus asked them to came regularly at the NFU and they came for at least 3 months period and completed on an average 4 follow-up visits. Of them, 82 (46%) were female children. The mean ± SD age of the children at first follow-up visit was 13.4 ± 7.8 months, ranging from 6 to 59 months. When they completed the 3 months follow-up, their age was 16.0 ± 7.5 months. Over the 3 months, follow-up period anthropometric parameters including length or height, weight, and MUAC of the children increased compared to first follow-up data (Table 1). The WHZ improved from −2.70 ± 0.94 to −1.95 ± 1.00, P < .001, MUAC from 105 ± 8 to 115 ± 9 mm, P < .001, and WAZ improved little from −4.65 ± 0.60 to −4.12 ± 0.71. However, stunting status remained unchanged (length or height-for-age z-score [HAZ] −4.75 ± 1.08 vs −4.81 ± 1.23, P = .376; Table 1). Their increment in weight was 882 ± 614 g and rate of weight gain was 2.2 ± 1.9 g/kg/d over these 3 months follow-up period.
Anthropometric Parameters at First Follow-Up, After 3 Months, and the Changes Over 3 Months.a
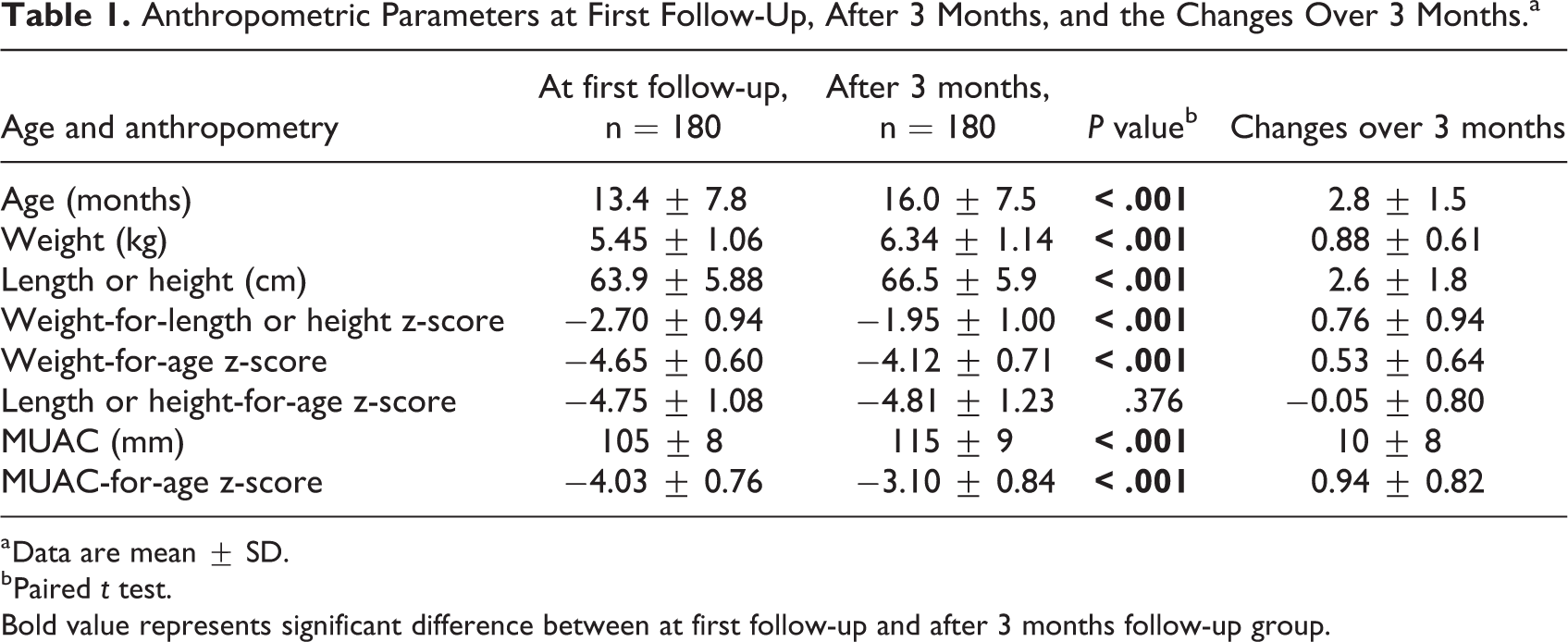
a Data are mean ± SD.
b Paired t test.
Bold value represents significant difference between at first follow-up and after 3 months follow-up group.
Overall comorbidity during the prior 14 days of respective NFU visits was lowest (46%) at first follow-up and it was gradually increased (63%) up to third follow-up. Common cold and/or cough, and pneumonia were the main causes of morbidity in all follow-up visits which ranged from 13.9% to 22.8% and 12.2% to 15.1%, respectively. Skin infection was 8.3% to 12.8%, and diarrhea was 3.3% to 6.1% (Table 2). Analyzing the cumulative morbidities, it was observed that 12.2% of children had 4 episodes of morbidities, 25.3% had 3 episodes, 34.1% had 2 episodes, and 21.7% had single episode of morbidity, and only 6.4% did not have any history of morbidity over these 3 months of follow-up period. Younger children had frequent morbidities (> 2 episodes over 3 months) than older children (Table 3).
Morbidities (%) of Severely Wasted Children Prior to the Respective Follow-Up (FU) Visit.a
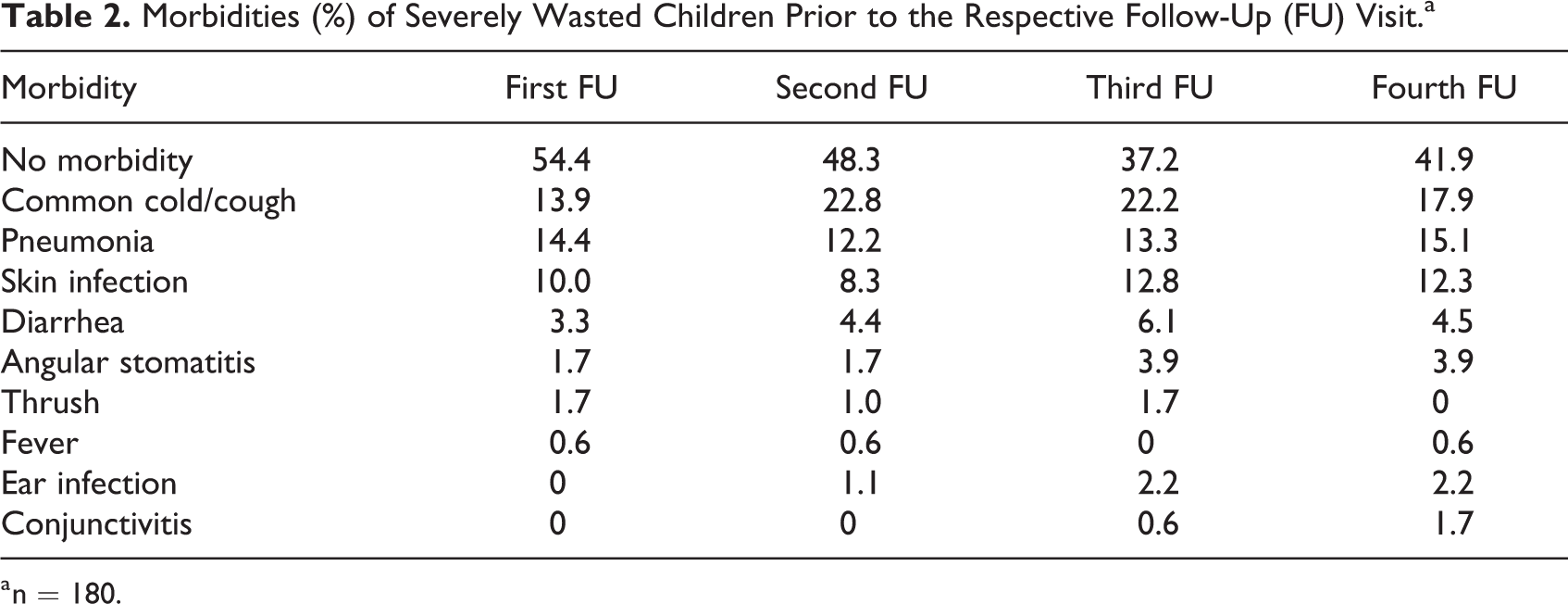
a n = 180.
Anthropometrics on Enrollment and Changes in Nutritional Status Over 3 Months of Follow-Up by Morbidity Status.a
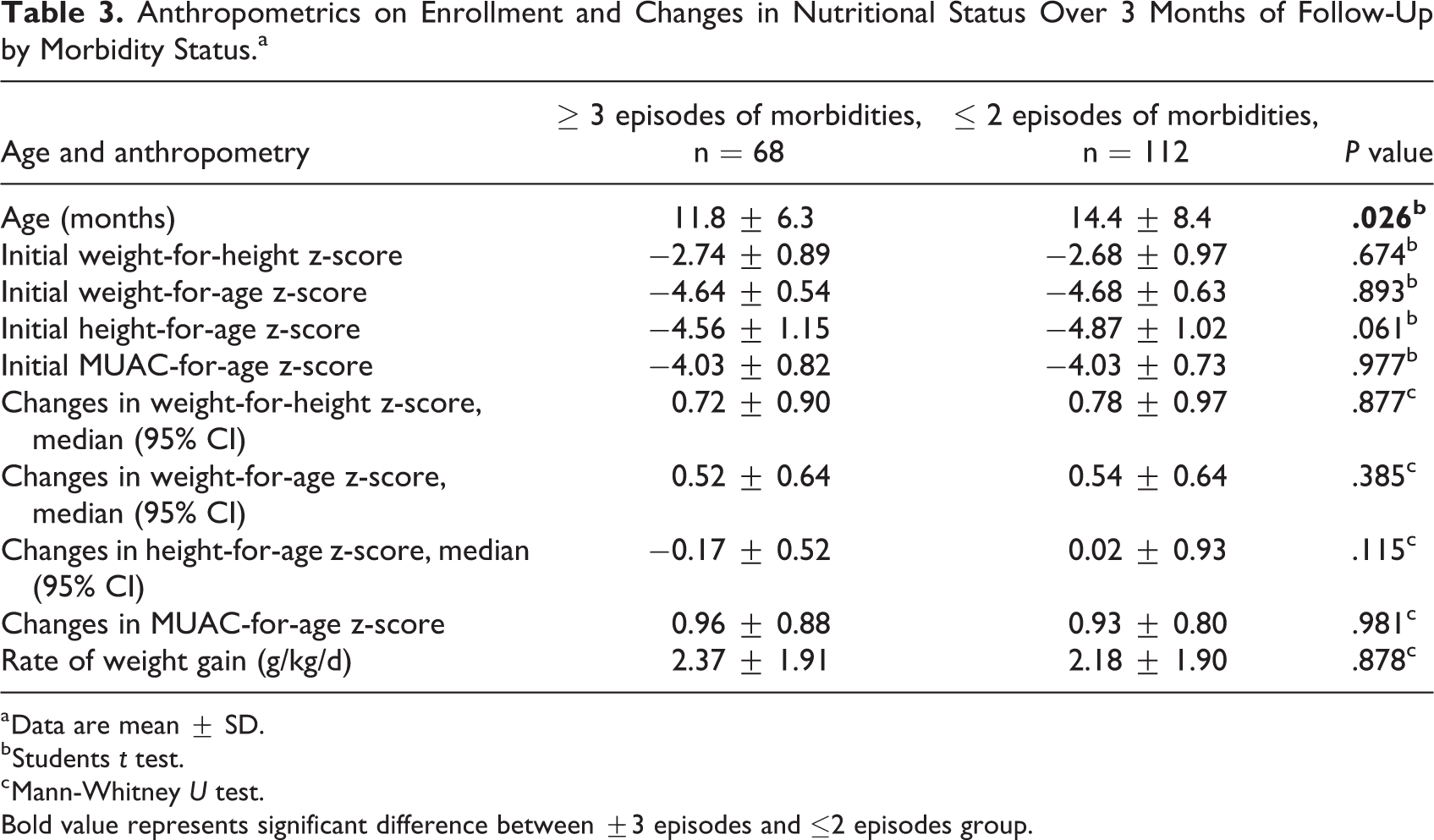
a Data are mean ± SD.
b Students t test.
c Mann-Whitney U test.
Bold value represents significant difference between ±3 episodes and ≤2 episodes group.
Discussion
Addressing severe wasting is of critical importance because of the higher risk of morbidity and mortality 4,5 for children who lose too much of their body weight in respect to their length or height. It will be difficult to continue improving rates of child survival without improvements in the proportion of severely wasted children receiving timely and appropriate lifesaving treatment. 7,8,12 This study assessed the anthropometric changes and morbidities of the U-5 children with severe wasting/SAM during the follow-up visits at the NFU of icddr, b over 3 months period. There is a paucity of published data regarding the anthropometric changes and morbidities in this group of children with severe wasting who did not receive any dietary intervention. Management of the children having SAM in few places (eg, Rohingya-refugee SAM-children came from Myanmar in the makeshift camp in Cox’s Bazar district) in Bangladesh and in some other (especially, African) countries is done using ready-to-use therapeutic food as per the recommendation of WHO. 2,7,10 However, in the NFU of the Dhaka hospital of icddr, b these severely wasted/SAM children were provided with dietary counseling, health education, and micronutrient supplementation without any food supplementation. A previous study from this same research center showed that undernourished children who attended the follow-up visits regularly had no post-discharge mortality, whereas 32 (10%) of 315 patients died in the community during the 3 months follow-up period who did not attend any follow-up visit. 11
In this observational study, it has been revealed that there was some improvement (although not up to the mark) of wasting status (WHZ); however, this improvement was somehow better than that of underweight (WAZ) status. Because wasting is the marker of acute malnutrition, improvement in WHZ is usually seen first compared to other anthropometric indices. Underweight is related to both acute and chronic malnutrition, thus, it usually takes a longer time to improve. Similarly, we did not find any improvement in stunting status (results of longer term/chronic undernutrition) expressed by HAZ, which was almost static. The promotion of linear catchup growth in the stunted children requires prolonged period of ponderal catchup often not totally achievable in the environment in which the children are recovering. Earlier studies 13,14 found and suggest that children usually gain height after they have reached around 85% of their targeted weight-for-height. Though the actual height/length of the children increased significantly from the baseline, it could not cover the previous shortage of height/length. So, we can postulate that the improvement of anthropometric indices/growth may take more than 3 months time period or it may be related to other factors.
We found that many children had different types of morbidities during the previous weeks or at the time of each follow-up period. However, this was not a surprising observation because previous study at same institution also reported the same findings 15 and thus warranted the importance of NFU in such population. Respiratory illnesses were the most common morbidities in our study that might have some contributing role to keep the static condition of stunting status, though the pathophysiology is unknown. A study in Africa showed that the acute respiratory illness has an odd of 1.21 (95% CI: 1.15-1.27) for stunting. 16 Moreover, our study children had multiple episodes of morbidities which may contributed for unchanged stunting status and not becoming moderate underweight from severe state which was similar in few earlier studies. 17,18 In Bangladesh, pneumonia and diarrhea are the lead killer diseases among U-5 children like other developing countries, 19 and these increase the odds of death when coupled with malnutrition. 20 However, among all comorbidities respiratory infection was found as the top most cause during this follow-up period than diarrhea, whereas almost all patients had diarrhea before they were enrolled in NFU. Relatively lower rate of diarrhea can be explained by the improvement of health and hygiene along with handwashing practice by the caregivers which was counseled and demonstrated by the health workers during hospital stay and at each follow-up visits that eventually might reduce the transmission of diarrhea of their children. It also warrants for effective health education on how to maintain personal hygiene of the children to reduced skin infections that were also observed in our study in a significant percentage.
Although supplementary food may be helpful, in our study population, due to lack of appropriate strategy/guidelines we could not provide any dietary supplementation during the nutritional follow-up period. A previous study in children with moderate wasting with no access to supplementary feeding program also experienced high rates of deterioration and no improvement in anthropometric indices. 21 With proper dietary advice and micronutrient supplementation, weight gain may be possible to some extent within short period of time.
On the basis of this study, we may come to a consensus that severely wasted/SAM children who completed 3 months nutritional follow-up had some improvement of weight and length/height and their corresponding wasting indices (WHZ). However, stunting status was almost static at the end of this 3 months follow-up. To mitigate this situation, the clinicians or policy-makers may give more emphasis on the reduction of comorbidities, especially respiratory tract infections and diarrhea, during the follow-up period. Moreover, to get the desired changes in all nutritional indices and increased rate of weight gain, further improvement of the components of NFUs, especially the addition of an affordable dietary supplementation for the severely wasted children (as advised by WHO) may be needed.
Footnotes
Authors’ Note
All authors conceived and designed the study, and wrote the paper. M.I.H. and S.H. contributed to data collection and analyses. None of the authors/investigators has any financial interests that might be affected by the results of this study.
Acknowledgment
This research study was funded by core donors who provide unrestricted support to icddr, b for its operations and research. Current donors providing unrestricted support include Government of Bangladesh, Canada; Sweden; and the United Kingdom. The authors gratefully acknowledge these donors for their support and commitment to icddr, b’s research efforts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant support: icddr, b core fund.