
Abstract
Experience with modern neuroimaging techniques, computed tomography (CT) and magnetic resonance imaging (MRI) scans, in the diagnosis of Tolosa-Hunt syndrome (THS) is reviewed. Conventional CT scan remains normal in about two-thirds of these patients. In the reported 22 patients meeting the IHS criteria for a THS diagnosis on whom an MRI study was performed, MRI revealed a convex enlargement of the symptomatic cavernous sinus by an abnormal tissue isointense with gray matter on short TR/TE images and isohypointense on long TR/TE images. This abnormal tissue markedly increases in signal intensity after contrast injection. MRI seems also to be the ideal technique to follow progressive resolution of the abnormal tissue after steroids. Therefore, normal MRI would probably exclude THS, whereas in the appropriate clinical setting of steroid-responsive painful ophthalmoplegia, MRI showing the cavernous sinus abnormality described here suggests a diagnosis of THS. From these data, we propose that the fourth IHS criterion for THS diagnosis, “Exclusion of other causative lesions by neuroimaging and (not compulsory) carotid angiogram” should be changed to “Finding by MRI of specific cavernous sinus abnormalities (with the characteristics described herein) which slowly resolve with steroid treatment”.
Tolosa-Hunt syndrome (THS) is of unknown origin and is diagnosed primarily by a process of exclusion, mainly due to the difficulty of visualizing lesions in the cavernous sinus with classic neuroradiological techniques. In fact, THS is considered by some to be not a true entity, but just a clinical picture. This syndrome was described in 1954 by the Spanish neurosurgeon Eduardo Tolosa, who published the case of a man aged 47 suffering from “pain in the left orbital region and total left ophthalmoplegia” (1). He described the typical angiographic findings of this syndrome, consisting of segmental narrowing of the left carotid artery at the cavernous sinus level. At necropsy, a granulomatous inflammation of the left carotid sinus was found, while the right side was normal (1). Seven years later, William Hunt, a neurosurgeon working in Ohio, reported six clinical cases of this syndrome (2). He became interested in this condition because his wife, who was one of the cases reported in his paper, had presented this clinical picture (Eduardo Tolosa Jr., personal communication). Hunt offered no pathological results. In fact, all the neuropathological pictures in Hunt's paper (2) correspond to the case already reported by Eduardo Tolosa (1).
Clinical diagnosis of THS
THS is a rare painful ophthalmoplegia secondary to a granulomatous inflammation in the cavernous sinus area. Its diagnosis, according to the IHS criteria, is based on the following: (i) episode(s) of unilateral orbital pain for an average of 8 weeks if untreated; (ii) association with paralysis of one or more of the third, fourth, and sixth cranial nerves, which may coincide with the onset of pain or follow it by a period of up to 2 weeks; (iii) pain relief within 72 h after initiation of corticosteroid; and (iv) exclusion of other causative lesions by neuroimaging and (not compulsory) carotid angiography. Further, according to the IHS classification, some THS cases have additional involvement of the trigeminal nerve (commonly the first division) or optic, facial, or acoustic nerves. Sympathetic innervation of the pupil occasionally occurs (3).
There are no specific traits in the clinical picture that distinguish THS from other pathologic processes in the orbitocavernous region. Although dramatic, the response of THS to steroids is not diagnostic. A response to steroids has been reported in cases of painful ophthalmoplegia due to sarcoidosis, aneurysm, actinomycosis, lymphoma, plasma-cell dyscrasia, and other solid tumors (4, 5).
Neuroradiological diagnosis of THS
Prior to computed tomography (CT) and magnetic resonance imaging (MRI), the role of classic neuroimaging techniques in THS was to rule out structural or vascular causes of painful ophthalmoplegia. Demonstration of obstruction of the superior ophthalmic vein, poor filling of the cavernous sinus, and collateral venous flow can be demonstrated by orbital phlebography in about 50% of cases (6). Angiographic abnormalities thought to be consistent with arteritis are the exception rather than the rule in apparent THS, and are not specific to this condition (7). As clinical manifestations are not specific and cranial angiography and orbital phlebography may be normal, diagnosis of THS was made according to a process of exclusion.
CT scan
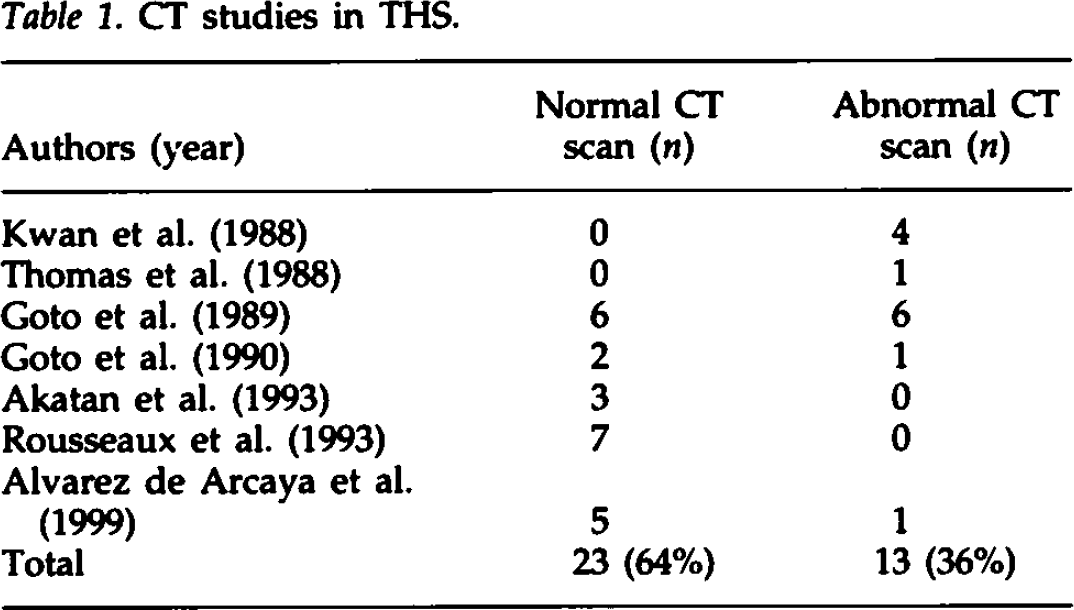
The advent of CT did not resolve the problem of THS diagnosis. We have identified 36 reported THS patients in CT scan studies (Table 1). Although high resolution techniques together with i.v. contrast infusion seemed to improve the rate of diagnosis in these patients, cavernous sinus lesions were observed in only 13 (36%) of these THS reported cases, the remaining 23 (64%) CT studies being reportedly normal. Thus, a normal CT scan does not exclude THS (7 –14).
CT studies in THS.
MRI studies
The results of cranial MRI have been reported in 24 patients with an apparent diagnosis of THS (4, 8, 9, 11 –16). In 22 of these patients, MRI showed abnormal signal mass lesions. The two cases with normal MRI had “painful third nerve palsy which resolved spontaneously” (15). In other words, they did not in fact have THS, according to current IHS criteria (3). Therefore, MRI has been shown to be abnormal in all the reported patients suffering from THS. With the advent of the MRI technique, THS seems now to be a diagnosis of inclusion.
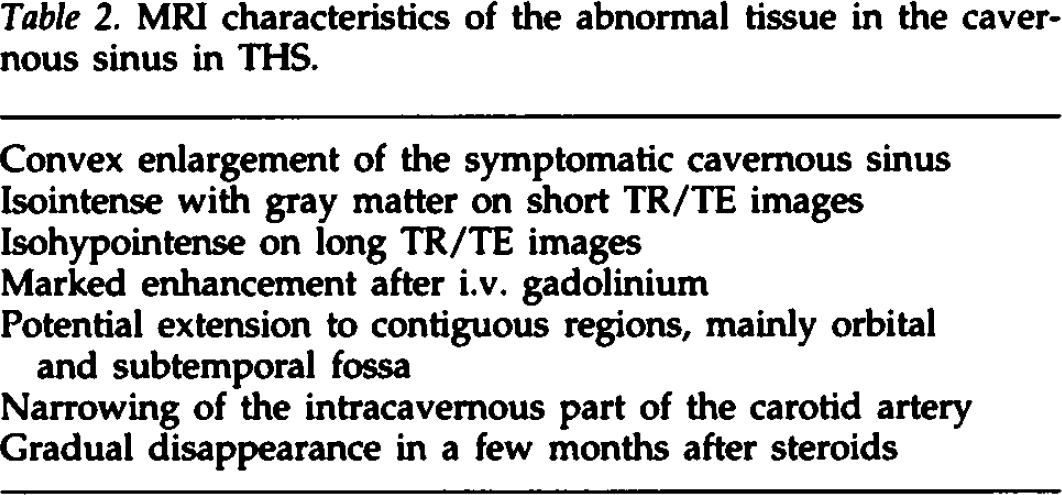
All these studies have shown enlargement of the clinically affected cavernous sinus by abnormal tissue, the outer dural margin being convex and bulging laterally (Fig. 1, Table 2) (4, 8, 9, 11 –16). The abnormal tissue is isointense with the gray matter on short TR/TE images and slightly isohypointense on long TR/TE images (Fig. 1A), and shows marked increase of signal intensity after i.v. gadolinium injection (Fig. 1B) (14, 16). MRI also detects a variable contiguous extension of the pathologic process into the ipsilateral orbital apex, the sphenoid and maxillar sinuses and the floor of the middle cranial and subtemporal fossae. MRI also discloses one of the classic angiographic findings in THS: narrowing of the intracavernous segment of the internal carotid artery (Fig. 2). We have reported MRI studies on a THS patient, before and after (6 weeks, 4 months, and 6 months) the beginning of steroid treatment. Although she was already free of symptoms and signs 3 weeks after the initiation of treatment, the abnormal attenuating tissue, despite progressively decreasing in size, only disappeared in the last MRI study performed 6 months after steroids (14). Thus, when managing such patients it should be taken into account that clinical resolution of symptoms precedes by weeks or even months the normalization of MRI studies.

MRI T1 weighted images (440TR/16TE) of one representative THS case. (A) Coronal image showing enlargement of the left cavernous sinus by abnormal tissue isointense with gray matter (arrows). The outer margin is convex and bulging laterally. (B) Contrast-enhanced coronal image. The abnormal soft tissue markedly increases in signal intensity after contrast injection (arrows). There is an enhancing soft tissue in the wall of the left sphenoid sinus.

Postcontrast coronal T1 weighted MRI in one THS patient revealing narrowing of the intracavernous portion of the left internal carotid artery (arrowheads) as compared with the normal right side.
MRI characteristics of the abnormal tissue in the cavernous sinus in THS.
Diagnostic proposal and conclusion
It seems fairly clear that a normal MRI would exclude a THS diagnosis, whereas in the appropriate clinical setting of steroid-responsive painful ophthalmoplegia, an MRI showing the cavernous sinus abnormalities described here suggests a diagnosis of THS. Among the differential diagnosis of steroid-responsive painful ophthalmoplegia, sarcoidosis, lymphoma, and meningioma may theoretically display mass signal changes like those in THS. Meningiomas, however, do not resolve with steroid therapy, and lymphoma and sarcoidosis often have other systemic or neurological symptoms. From these data, we suggest that the fourth IHS diagnostic criterion for THS, “Exclusion of other causative lesions by neuroimaging and (not compulsory) carotid angiography” should be changed to “Finding by MRI of specific cavernous sinus abnormalities (with the signal and extension characteristics described herein) which slowly resolve with steroid treatment”.