
Abstract
Background
Tolosa-Hunt syndrome (THS) manifests as a benign or an inflammatory type disease. The nosography differences between these types remain to be elucidated. We aimed to analyze and compare the clinical presentations of benign and inflammatory THS.
Methods
The ward patients who presented with THS from January 1990 to May 2011 were retrospectively reviewed. THS was diagnosed according to the recommendations of the International Headache Society.
Results
Of the 53 THS cases (49 patients), 30 (56.6%) were classified as benign and 23 (43.4%) as inflammatory THS. There were strong similarities between the groups in terms of clinical manifestations, laboratory findings, responses to glucocorticoid treatment, and outcomes. However, patients with inflammatory THS tended to be younger (mean age, 43.4 years; p < 0.05) and have optic nerve dysfunction (56.5%; p < 0.05) and longer disease duration (2.3 ± 1.0 months; p < 0.05) compared to those with benign THS (mean age, 56.4 years; mean disease duration, 1.6 ± 0.7 months). The patients with additional involvement of both the optic nerve and the second division of the trigeminal nerve experienced a longer disease duration (p < 0.05). Additionally, patients with orbital pseudotumors had diplopia that responded poorly to treatment with glucocorticoids (p < 0.05). High-dose (>0.5 mg/kg/day) and low-dose (≤0.5 mg/kg/day) prednisolone were equally effective in relieving symptoms in both groups (p > 0.05).
Conclusion
Benign and inflammatory THS were highly similar in terms of nosography. The responses to glucocorticoid treatment were generally good except in patients with orbital pseudotumors.
Keywords
Introduction
Tolosa-Hunt syndrome (THS) is a painful ophthalmoplegia caused by an idiopathic granulomatous inflammation of the cavernous sinus (CS) (1,2). It is characterized by recurrent unilateral orbital pain, ipsilateral ocular motor neuropathy, and a rapid response to glucocorticoid therapy (3). The advent of magnetic resonance imaging (MRI) has facilitated the identification of lesions in the parasellar and orbital areas, and the revised criteria of the International Headache Society (IHS) in 2004 included the presence of granuloma as a diagnostic criterion (4).
However, a few studies on THS have indicated that some patients with typical THS features showed normal findings in imaging studies (5–7). According to the review by La Mantia et al., the images for nearly half of the reported THS patients include no evidence of granuloma (8). This group of patients was designated as having benign THS, while granulomas that were revealed by imaging or biopsy were designated as inflammatory THS.
Although patients with benign and inflammatory THS are often identified, their clinical characteristics have not been well understood (8,9). In addition, though many reports have illustrated the MRI findings associated with inflammatory THS (10–14), the relationship of image findings to clinical manifestations has not been studied to date. In this study, we aimed to analyze the clinical presentations, cranial MRI findings, and responses to glucocorticoids in patients with benign and inflammatory THS. We also attempted to determine the correlation between image findings and clinical manifestations in inflammatory THS. These results may refine our understanding of THS.
Methods
Patients presenting with THS between January 1990 and December 2011 at Chang Gung Memorial Hospital, a tertiary referral medical center, were recruited for this study. Their in-hospital medical chart records were retrospectively collected under the approval of the institutional review board (license ID: 100-0136B). Patients who developed periorbital or hemicranial pain combined with ipsilateral oculomotor, trochlear, and/or abducens palsies were recruited for this study. Patients with head trauma, autoimmune disease, malignancy, cranial herpes zoster, Horton’s arteritis, infections with human immunodeficiency virus or other potential types of immunological compromise, ocular diabetic neuropathy, and ophthalmoplegic migraines were excluded from this study.
The diagnosis was made on the basis of the clinical presentations according to the recommendations of the IHS, second edition (2004) (4). Because symptoms of THS may resolve spontaneously without glucocorticoids (2,3), patients with self-remission within three months without glucocorticoid treatment were enrolled in the study. Because cranial nerve dysfunction may even improve after six to eight weeks of glucocorticoid treatment (11,15), patients who had pain that resolved within 72 hours (h) after treatment without an immediate improvement in their diplopia were recruited. Patients fulfilling the diagnostic criteria of THS with normal cranial MRI were classified as having benign THS, while those with demonstration of granulomas on MRI were classified as having inflammatory THS (8). All patients with a final diagnosis of THS, either benign or inflammatory, were followed by out-patient services and telephone contacts for at least six months. Cerebral vascular investigations (MR angiography or digital subtraction angiography) showed that all patients were free of vascular anomalies.
Clinical information was collected from hospitalization records and through telephonic follow-up. A typical THS involved paresis of one or more of the third (CN3), fourth (CN4) and/or sixth (CN6) cranial nerves (CN), with orbital pain along the first division of the trigeminal nerve (CN5–1) (4,16). Occasionally cases were reported with additional involvement of the trigeminal nerve, optic, facial or acoustic nerves (4). Given that specific combinations of cranial nerve palsies may highlight some important basic anatomy (17), we classified patients according to the combinations of cranial nerves involved (Figure 1). The classification was as follows: Type 1, with involvement of ocular motor nerves (CN3, CN4, and/or CN6), and CN5–1, suggesting lesions located at the superior orbital fissure (SOF) and/or anterior CS (17); Type 2, with involvement of ocular motor nerves, CN 5–1, and optic nerve (CN2), suggesting lesions located at the orbital apex (OA) (16); Type 3, with involvement of ocular motor nerves, CN5–1, and CN 5–2, suggesting lesions located at the posterior CS (17); and Type 4, with involvement of ocular motor nerves, CN 2, CN 5–1, and CN 5–2, suggesting a diffuse lesion extending from the OA to the CS.
The anatomical basis of the lesions causing multiple cranial neuropathies is illustrated above. Type 1, a lesion in superior orbital fissure (SOF)/anterior cavernous sinus (CS), causing neuropathies of the oculomotor nerve (CN3), trochlear nerve (CN4) and/or abducens nerve (CN6), and the first division of the trigeminal nerve (CN 5–1). Type 2, a lesion in the orbital apex (OA), causing neuropathies of CN3, CN4 and/or CN6, CN 5–1, and the optic nerve (CN2). Type 3, a lesion in the posterior CS, causing neuropathies of CN3, CN4 and/or CN6, CN5–1, and the second division of the trigeminal nerve (CN5–2). Type 4, a diffuse lesion extending from the OA to the CS, causing neuropathies of CN3, CN4 and/or CN6, CN 2, CN 5–1, and CN 5–2.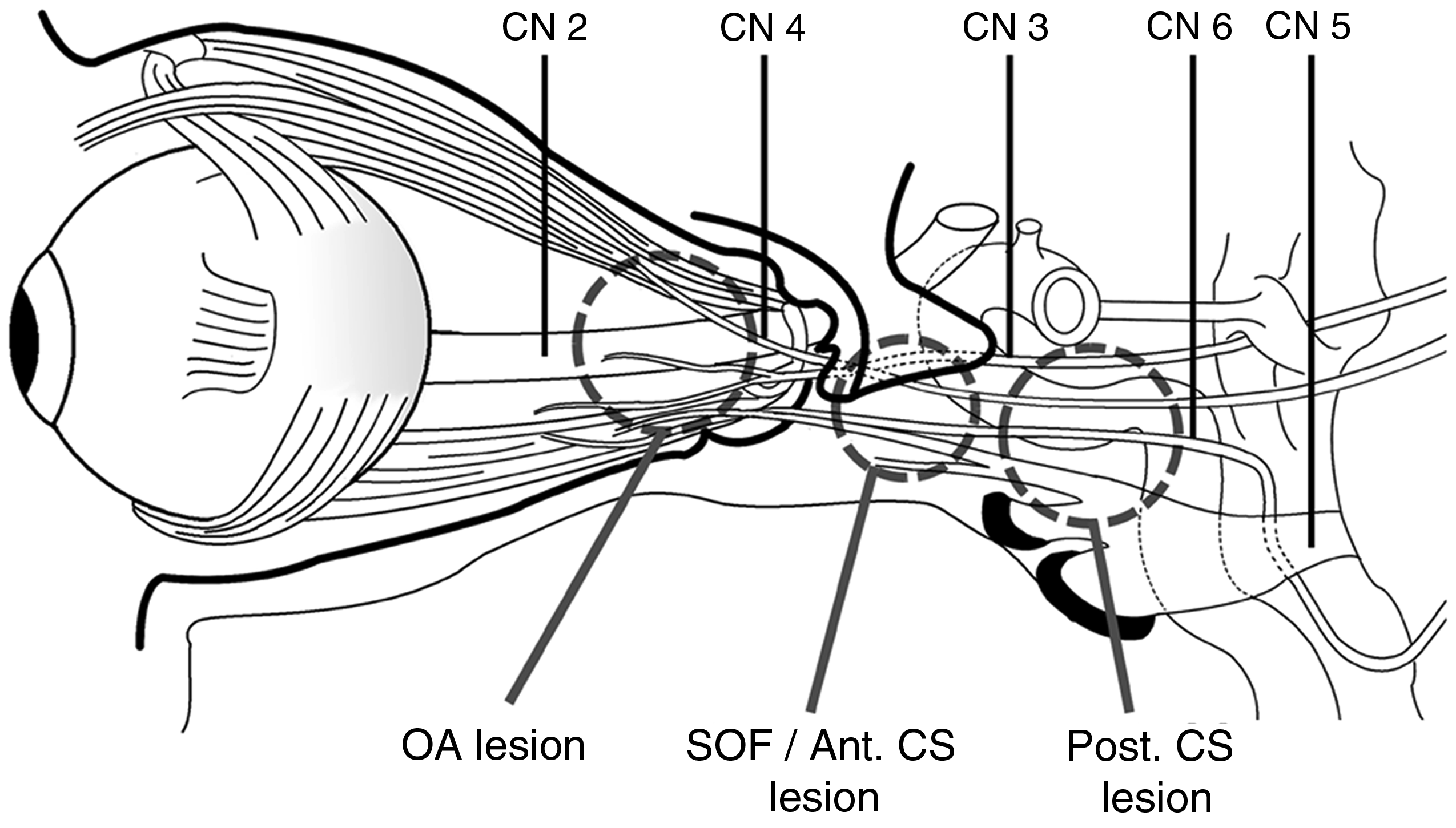
All patients underwent cranial MRI with a standard head coil on a 1.5–3 T MR scanner. Predefined parameters of the MR scans performed in this study were as follows: transverse and coronal T1-weighted spin-echo sequences (repetition time (TR) = 450–600 ms, echo time (TE) = 9.9–26 ms, field of view (FOV) = 200 × 200 mm; matrix 512 × 512) before and after the intravenous administration of gadolinium enhancement (0.2 ml/kg), transverse T2 fast spin-echo sequence (TR = 3114–4200 ms, TE = 82–90 ms, FOV = 200 × 200 mm; matrix 512 × 512), and transverse fluid-attenuated inversion recovery sequence (FLAIR, TR = 4200–9000, TE = 90–142 ms, FOV: 200 × 200 mm; matrix 512 × 512). The sections were obtained at 3 or 5 mm slice thickness.
The assessment of MRI was performed retrospectively and independently by two experienced neuroradiologists (YL Chen and YM Wu) and one neurologist (CH Hung), with the focus on the parasellar area and orbits. A positive finding required the agreement of at least two of the three reviewers.
The definition of positive findings was adapted from publications by Schuknecht (10), Cakirer (11), Jain (12), and Bone (17) et al. The positive imaging findings were defined as follows: a local increase in the size of the CS with a bulging contour due to enhanced soft lesions, dural enhancement of lesions after contrast, narrowing of the intra-cavernous portion of the internal carotid artery (ICA), enhanced lesions penetrating the CS and extending to the SOF, enhanced lesions involving OA and CN2, or enhanced lesions involving extraocular muscles (EOM).
Patients with inflammatory THS were classified into groups according to the MRI findings, as follows: Group A, lesions restricted to the CS; Group B, lesions in the CS with extension to the SOF; Group C, lesions in the CS and SOF with extensions to the OA with/without EOM; and Group D, lesions confined to the OA and/or EOM, which are known as orbital pseudotumors or idiopathic orbital inflammation (18).
The glucocorticoid dosages and patient weights were registered. A high dose of glucocorticoids was defined as a dose >0.5 mg/kg prednisolone/day (19). In contrast, a daily dose of prednisolone ≤0.5 mg/kg was defined as low-dose glucocorticoid treatment. A positive response to glucocorticoids was defined as the relief of symptoms or the improvement of neurologic signs within three days of glucocorticoid treatment (4,15,20).
Statistical analyses were performed using the Statistical Program for Social Sciences (SPSS) statistical software (version 20.0, Chicago, IL, USA). For each set of values, data were expressed as means ± standard deviation (SD). The nominal variables were compared using Pearson’s chi squared test. The cardinal variables were compared using an independent sample t test or one-way analysis of variance (ANOVA). All of the p values were two tailed. A p value <0.05 was considered statistically significant in all tests.
Results
Demographic data and clinical manifestations of Tolosa-Hunt syndrome (THS).

MRI: magnetic resonance imaging; N: number; CN: cranial nerve; ESR: elevated sedimentation rate; CN 5-2: secondary division of trigeminal nerve; N/A: no statistics available due to the constant pain responses. aStatistically significant value.
The demographic data and clinical manifestations of the 53 cases are summarized in Table 1. The mean age of patients at the onset of inflammatory THS (46.7 ± 19.4 years) was lower than that of patients with benign THS (56.4 ± 12.3 years; p = 0.031). The gender distribution was identical in both groups.
Most cases of painful ophthalmoplegia (n = 46; 86.8%) showed unilateral ophthalmoplegia. Only six cases of benign THS (20.0%) and one of inflammatory THS (4.3%) showed bilateral involvement. The most frequently involved cranial nerve was the oculomotor nerve (79.2%), followed by the trochlear nerve (62.3%) and the abducens nerve (54.7%). Optic nerve involvements were more frequently seen in the patients with inflammatory THS (56.5%) than in those with benign THS (26.7%; p = 0.028). Involvement of the second branch of the trigeminal nerve was reported in seven cases (23.3%) of benign THS and six cases (26.1%) of inflammatory THS. Multiple cranial nerve palsies were observed in a majority of both benign (66.7%) and inflammatory (65.2%) THS patients.
The erythrocyte sedimentation rates (ESRs) were grossly normal (<30 mm/h) and similar in both groups. Glucocorticoids were prescribed for 25 cases of benign THS and 20 of inflammatory THS. Four cases of benign THS had improved before glucocorticoid use and were excluded from this analysis. The mean dose of prednisolone used to treat benign and inflammatory THS was 1.83 ± 5.35 and 1.14 ± 2.24 mg prednisolone/kg/day, respectively. All patients with THS experienced immediate pain relief within 72 h of glucocorticoid treatment. Nineteen cases (90.5%) of benign THS and 14 cases (70.0%) of inflammatory THS showed immediate improvement of diplopia after glucocorticoid use.
The duration of disease in inflammatory THS patients was 2.3 ± 1.0 months, which was significantly longer than that in benign THS patients (1.6 ± 0.7 months; p = 0.041). Most of the cases (n = 51; 96.2%) reported complete recovery except for one benign (3.7%) and one inflammatory (4.3%) THS case with sequlae of double vision.
Clinical presentations of Tolosa-Hunt syndrome (THS) based on involvement of cranial nerves.

CN2: optic nerve; CN3: oculomotor nerve; CN4: trochlear nerve; CN6: abducent nerve; CN5–1: first division of trigeminal nerve; CN5-2: second division of trigeminal nerve; CNs: cranial nerves; SOF: superior orbital fissure; ant. CS: anterior cavernous sinus; post. CS: posterior cavernous sinus; OA: orbital apex; N/A: no statistics available due to the constant pain responses.
All patients underwent MRI examinations during the acute stage of the disease. The mean intervals from onset to MRI were 10.8 ± 11.5 and 13.6 ± 11.9 days in the benign and inflammatory THS groups, respectively. Representative image findings are presented in Figure 2. Contrast enhancement of the lesion was uniform. A local increase in the size of the CS was identified in 15 cases (65.2%), bulging of the dural contour of the CS in 15 (65.2%), narrowing of the ICA in one (4.3%), lesions extending to the SOF in 13 (56.5%), lesions involving the OA and optic nerve in 11 (47.8%), and lesions involving the EOM in six (26.1%). Six patients underwent follow-up MRI at intervals of 4.4 ± 2.1 months. The results obtained during follow-up showed that all lesions had resolved.
Post-gadolinium spin-echo (SE) T1-weighted transverse and coronal cranial magnetic resonance images of our cases of inflammatory Tolosa-Hunt syndrome (THS) are illustrated above. The positive findings are indicated by a white arrow in each photograph. Contrast enhancement of the lesion was uniform. (a and b) The local increase in the size of the cavernous sinus (CS) with a bulging contour due to enhanced soft lesions. (c and d) Dural enhancement of the lesions after contrast. (e and f) Narrowing of the intra-CS portion of the left internal carotid artery compared to the normal right side. (g and h) Enhanced lesions infiltrating the CS and extending to the superior orbital fissure. (i) Enhanced lesions involving the orbital apex. (j and k) Contrast enhancement of the optic nerve sheath. (l and m) An enhancing lesion within the left orbit involving orbital fat and extraocular muscles. (n) An enhancing lesion within the orbit from the sagittal view.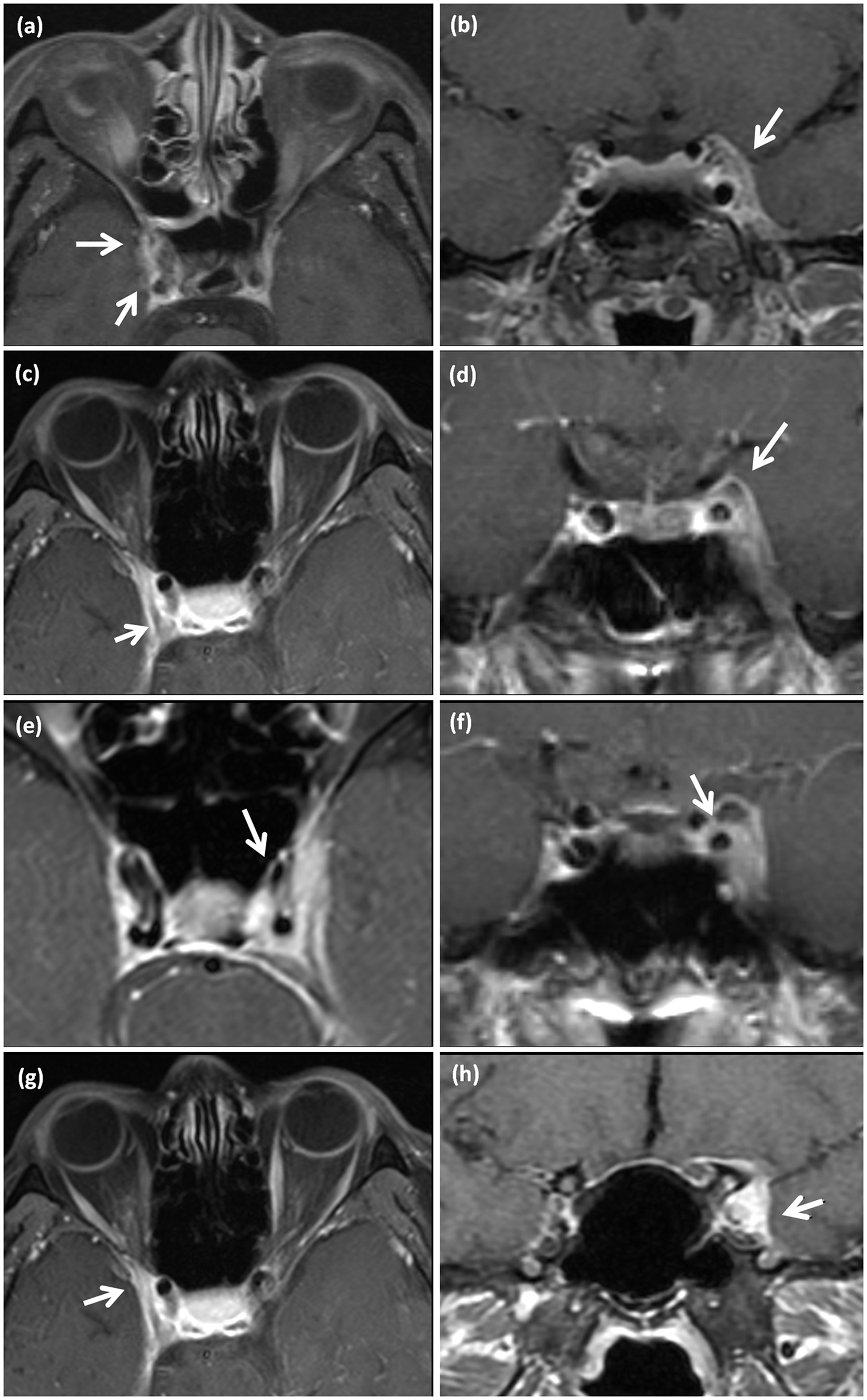
The lesions found in patients with inflammatory THS were classified into four groups according to the associated MRI findings (Table 3). Representative images are presented in Figure 3. There was no significant difference among the groups in terms of demographic data, disease duration, or outcomes. Unlike the analysis of patients classified on the basis of clinical presentations, patients with extensive lesions on MRI (Group C) were not more likely to experience an extended duration of disease. The efficacy of glucocorticoids in achieving immediate pain relief was overwhelming in all patients. However, the efficacy in resolving diplopia was relatively poor in Group D (p = 0.015). Nine benign and three inflammatory cases were not treated with glucocorticoids because of the absence of secure diagnosis at onset. The glucocorticoid treatment duration of the remaining 41 THS patients was 2.44 ± 2.91 months. Twenty-one (12 benign and nine inflammatory THS) were treated with high-dose glucocorticoids. In either benign or inflammatory THS, high-dose and low-dose glucocorticoid treatments were similarly effective in mitigating diplopia (Table 4). Although glucocorticoids provided immediate symptom relief, patients treated with glucocorticoids did not recover faster than those who were not treated with glucocorticoids in either the benign or inflammatory group (p = 0.667 and p = 0.549, respectively).
Enhanced T1-weighted transverse magnetic resonance images of patients with inflammatory Tolosa-Hunt syndrome. (a) Lesions restricted to the cavernous sinus (CS). (b) Lesions in the CS with extension to the superior orbital fissure (SOF). (c) Lesions in the CS and SOF, with extension to the orbital apex (OA). (d) Lesions confined to the OA and/or extraocular muscles, known as orbital pseudotumor or idiopathic orbital inflammation. Clinical manifestations of inflammatory THS based on image findings of cranial MRIs. THS: Tolosa-Hunt syndrome; MRIs: magnetic resonance images; lesion in CS: lesion within anterior cavernous sinus, local increase in size of the cavernous sinus, bulging of the dural contour, loss of definition of the dural border on T2 images, narrowing of internal carotid artery, or dural enhancement after contrast; SOF: lesions extending to superior orbital fissure; OA: lesions involving orbital apex or optic nerve; EOM: lesions involving ocular muscle; N/A: no statistics available due to the constant pain responses. The responsive rate of pain and diplopia between high and low-moderate dosage of glucocorticoids in benign and inflammatory Tolosa-Hunt syndrome (THS). A positive response to glucocorticoids was defined as relief of symptoms or improvement of neurologic signs within three days of glucocorticoid treatment. A high dosage of glucocorticoids was defined as dose >0.5 mg/kg prednisolone a day. A low dose of glucocorticoids: ≦0.5 mg/kg prednisolone a day. N: number; N/A: no statistics available due to the constant pain responses.


Discussion
The current study demonstrated several findings. There were strong similarities between benign and inflammatory THS in terms of clinical manifestations, laboratory findings, the response to glucocorticoids, and clinical outcomes. Patients with additional involvement of both CN2 and CN5-2 experienced a longer duration of the disease. Additionally, patients with orbital pseudotumors tended to have diplopia that responded poorly to glucocorticoids. High-dose and low-dose glucocorticoid regimens were equally effective.
The demographic data, clinical presentations, disease duration, and outcomes of benign and inflammatory THS patients reported here are comparable to those reported in a previous review (8). We noticed that the nosography of benign THS is very similar to that of inflammatory THS. The similarities between the groups suggest that inflammation may contribute to the pathogenesis of both conditions (1,2). A granulomatous inflammation is a focal accumulation of activated macrophages surrounded by leukocytes (21) and typically is a small (1–2 mm) lesion (22,23). Because the spatial resolution of 3-T MRI with contrast was 1.0–2.0 mm at best (24,25), lesions less than 1.0 mm in diameter may be undetectable by MRI. Therefore, patients with invisible inflammatory lesions on MRI might be regarded as having benign THS. Another possible explanation for misclassification as benign THS would be poorly timed MRI. However, in our study, the intervals from initial symptoms to MRI were similar in both groups.
From this perspective, inflammatory THS could be the more severe and invasive form of THS. This might help to explain the younger age at onset and longer duration of disease in patients with inflammatory THS. In addition, because the granulomas tended to be more massive in inflammatory THS, the granulomas tended to extend anteriorly to the OA, leading to compression of the optic nerve.
The involvement of additional cranial nerves suggests that lesions have invaded beyond the SOF/anterior CS (17). A combination of CN2, CN3, CN4, CN5–1, CN5–2, and CN6 neuropathies suggests more extensive lesions (extending from the OA to the posterior CS), corresponding to the longer duration of disease.
In patients with inflammatory THS, abnormal masses were identified within the ipsilateral CS in most cases (87.0%). Extension into the OA was observed in nine (39.1%) cases, similar to the findings of previous studies (range, 25% to 72.7%) (6,10,13,26). The imaging results and clinical presentations did not always correspond: Imaging evidence of OA involvement was not necessarily tied to optic nerve dysfunction; this is similar to previously published findings (10). Optic neuropathy was sometimes found in patients with lesions confined to the CS and SOF on images. Interestingly, although inflammatory THS patients with diffuse lesion-specific neuropathies (Type 4) had a longer disease duration, patients with image-based evidence of corresponding lesions (Group C) did not. The disparity between clinical presentations and image-based evidence may be a result of the limitations of MRI resolution. Clinical neurological findings may therefore be more important than imaging in predicting a patient’s clinical course.
Orbital pseudotumors accounted for only a small group of inflammatory THS patients (13.0%). The hypothesis that THS is a variant of idiopathic inflammatory orbital pseudotumor is based on similarities with respect to imaging, histopathology, and clinical presentation (27,28). Therefore, we classified orbital pseudotumor patients as inflammatory THS patients in this study. Our study demonstrated a poorer response of diplopia to glucocorticoids in these patients. A similarly poor glucocorticoid response (31%) was reported previously (29). In addition, although glucocorticoid therapy resulted in a low cure rate (37%) in retrospective studies (30–32), each patient in our study ultimately experienced complete recovery.
Although the beneficial effect of glucocorticoid therapy in THS has been documented (3), the optimal dosage of glucocorticoids remains controversial. In our study, high-dose glucocorticoid (>0.5 mg/kg prednisolone/day) treatment had a similar effect for the mitigation of diplopia as did the low-dose (≤0.5 mg/kg prednisolone/day) treatment, in benign and inflammatory THS. In view of this, we recommended low-dose glucocorticoids as treatment. In addition, no data are available in the literature as to whether treatment hastens recovery. Our study found that patients treated with glucocorticoids did not recover faster than those without treatment in either group.
A recent view by Colnaghi et al. suggested that an MRI scan should be performed with 3 mm thickness sequences (15). The choice of slice thickness is limited to the given field strength magnets of the scanner; 3 mm slices were routinely used in 3 T imaging, whereas with a field strength of 1.5 T, a 5 mm thickness is advocated to obtain sufficient signal-to-noise ratio (33). In this study, pre-defined 1.5 T/5 mm and 3 T/3 mm sequences were used, and a lower spatial resolution of 1.5 T imaging might be a limitation in detecting granulomatous lesions. However, the sensitivity in detecting sellar lesions was not significantly different between 3 T and 1–1.5 T modalities (83% and 67%, respectively) (34). In addition, patients with 1.5 T/5 mm modality didn’t have a significantly higher percentage (60.7%) of benign THS diagnosis than those with 3 mm thickness (52.9%; p=0.523) in the current study. Even so, we still recommend the 3 T/3 mm modality in THS imaging because of the superiority in detection and accurate characterization of the structural brain (33,35).
Several studies indicated specific MR sequences may facilitate the diagnosis of THS (36–38). Colnaghi et al. recommended T1 fat-suppressed weighted images with contrast (15), while other authors recommended a fat saturation technique for CS imaging (35). The fat-suppressed method increases contrast between enhancing lesions and the surrounding fat tissue, and is of particular benefit in orbital imaging (39). Occasionally, the method is also useful to identify CS lesions in obese patients or those with Cushing syndrome or receiving exogenous steroid therapy (35). Due to the limitation of a retrospective study, we are not able to evaluate the detectability of different MR sequences. A prospective study is indicated to determine the most appropriate MR sequences for THS in the future.
Our study had several limitations. First, the sample size of both groups might have been too small for adequate comparison. Second, due to the high-risk approach of biopsy, the diagnoses in our study were based on clinical presentation and MRI rather than on histopathological evidence. Third, the retrospective nature of this study did not allow us to evaluate in detail the optimal dose of glucocorticoids. A randomized controlled study of glucocorticoid therapy is indicated to establish a therapeutic protocol. Nevertheless, this study does provide useful information about the clinical features of THS in conjunction with imaging findings. As far as we know, this is the first study to compare benign and inflammatory THS and to correlate clinical manifestations with image findings. Further prospective studies are warranted to clarify the histopathology of THS and assess the optimal approach to treatment.
Clinical implications
There are strong similarities between benign and inflammatory Tolosa-Hunt syndrome (THS) in terms of clinical manifestations, laboratory findings, the response to glucocorticoids, and clinical outcomes. THS patients with additional involvement of both optic nerve (CN2) and the ocular motor nerve CN5-2 experience a longer duration of the disease, either benign or inflammatory type. Patients with orbital pseudotumors tend to have diplopia that responded poorly to glucocorticoids. High-dose and low-dose glucocorticoid regimens are equally effective in relieving symptoms. THS patients treated with glucocorticoids do not recover faster than those who were not treated with glucocorticoids.
Footnotes
Acknowledgments
We thank Hsiao-Jung Tseng, a researcher at the biostatistical center of Chang-Gung Memorial Hospital, for assistance with statistical analysis. We also thank Shao-Wei Huang for graphic design assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.