
Abstract
In 2004, the International Headache Society (IHS) re-defined the diagnostic criteria of Tolosa–Hunt syndrome (THS) specifying that granuloma, demonstrated by magnetic resonance imaging (MRI) or biopsy, is required for diagnosis. We reviewed the literature on THS published from 1988 (year of publication of first IHS criteria) to 2002, analysing individual cases in relation to the new IHS criteria. One hundred and twenty-four cases were identified. As far as it was possible to discern, clinical presentation was similar in all, but 44 (35±) were reported to have inflammation on MRI or bioptic evidence of granuloma, 41/124 (33±) had normal neuroimaging findings and 39 (31±) had a specific lesion, so the THS was secondary. These data confirm that clinical criteria for THS are common to several conditions and their application alone does not guarantee a correct diagnosis. The requirement for inflammation on MRI will result in better classification of painful ophthalmoplegias; nevertheless, an MRI protocol that best defines inflammation should be specified. The status of cases which fulfil the clinical criteria but have normal MRI remains to be clarified.
Introduction
Tolosa–Hunt syndrome (THS) is a painful ophthalmoplegia characterized by recurrent unilateral orbital pain, ipsilateral oculomotor paralysis and prompt response to steroids. The clinical features of the syndrome were fully described by Tolosa in 1954 (1), while Hunt, in 1961 (2), emphasized the efficacy of steroid treatment. Histopathological studies (1, 3–5) have shown that THS is due to a non-specific granulomatous inflammation of the cavernous sinus or orbital apex.
The 1988 headache classification (6) of the International Headache Society (IHS) included THS among the cranial neuralgias (Section 12.1.5) and provided four diagnostic criteria (Table 1). The classification aroused considerable debate, as some authors considered THS to be a localizing syndrome pointing to a specific intracranial disease (7, 8), while others considered it an idiopathic granulomatous inflammation (9, 10). The 1988 IHS criteria were also criticized because their application did not always produce a correct diagnosis (9, 11).
Diagnostic criteria for Tolosa–Hunt syndrome (THS)

Other causes of painful ophthalmoplegia include tumours, vasculitis, basal meningitis, sarcoid, diabetes mellitus and ophthalmoplegic ‘migraine’.
The revised IHS headache classification (12), published in 2004, retained THS among the cranial neuralgias (now Section 13.16) and now has five diagnostic criteria (Table 1). The novelties are the requirements that granuloma be demonstrated by magnetic resonance imaging (MRI) or biopsy; that the paresis as well as the pain respond promptly to steroids; and that appropriate investigations and follow-up exclude other causes.
The most authoritative clinical monograph on THS remains that published by Bruyn and Hoes in 1986 (3). However, no studies have analysed the literature on THS in the light of the IHS diagnostic criteria. We examined papers describing THS cases published between 1988 and 2002, and reviewed the diagnoses in the light of the 2004 IHS criteria, focusing as far as possible on MRI findings.
Materials and methods
Studies on THS published from 1988 to December 2002 were identified by searching PubMed using Keywords ‘painful ophthalmoplegia’ and ‘Tolosa–Hunt syndrome’. In addition, the reference list of each paper identified was hand-searched for further papers.
The complete papers of all promising references were obtained and read by two reviewers independently. Only papers (clinical series or case reports) in which symptoms, signs and neuroimaging findings [computed tomography (CT), MRI or angiography] were clearly reported were selected for further analysis; any disagreements were resolved by discussion. Data on individual cases were extracted from the papers onto an electronic form devised for the purpose. The following items were recorded for each case: sex; age; pain site (orbital, retro-orbital, periorbital, frontal, temporal, right-sided, left-sided, bilateral, alternating); cranial nerves involved; cranial nerve palsy duration; remission of palsy; pain duration; remission of pain; duration of attack (pain plus paresis); recurrence of attacks/complete recovery; whether steroids used; type and duration of steroid treatment; CT findings; MRI findings; MR angiography (MRA) findings; other angiographic findings (including phlebography); laboratory findings including cerebrospinal fluid; histopathological findings; final diagnosis; and duration of follow-up.
From the authors’ descriptions, we classified the neuroimaging findings as: (i) normal, indicating absence of imaging alterations to the cavernous sinus or orbital apex, cases with cavernous sinus asymmetry only were also considered normal; (ii) inflammatory, indicating presence of inflammation in the region of cavernous sinus ipsilateral to ophthalmoplegia, possibly extending to contiguous regions; or (iii) symptomatic, indicating a specific intracranial lesion (cerebral tumour, etc.). We then applied the new IHS criteria for THS to each case.
Results
We initially identified 159 papers from the search criteria, but 69 of these were excluded for lack of precise diagnostic information or unavailability of publication. A total of 208 cases were abstracted from the remaining 90 papers (Fig. 1). One hundred and twenty-four cases were identified. Forty-four (35%) were reported to have inflammation on MRI or bioptic evidence of granuloma and were designated inflammatory THS; 41 (33%) had normal neuroimaging findings and were designated benign THS; 39 (31%) had a specific lesion and were designated symptomatic THS; the remaining 84 cases fulfilled neither the clinical criteria nor the imaging/bioptic criteria for THS. Table 2 lists the included studies, the number of cases contributed by each study and the classification of each case based on neuroimaging findings. Table 3 shows the diagnoses of the symptomatic forms. The most common diagnoses of symptomatic forms were recurrent cranial neuropathy (26% of symptomatic cases), lymphoma (13%) and idiopathic hypertrophic cranial pachymeningitis (13%).
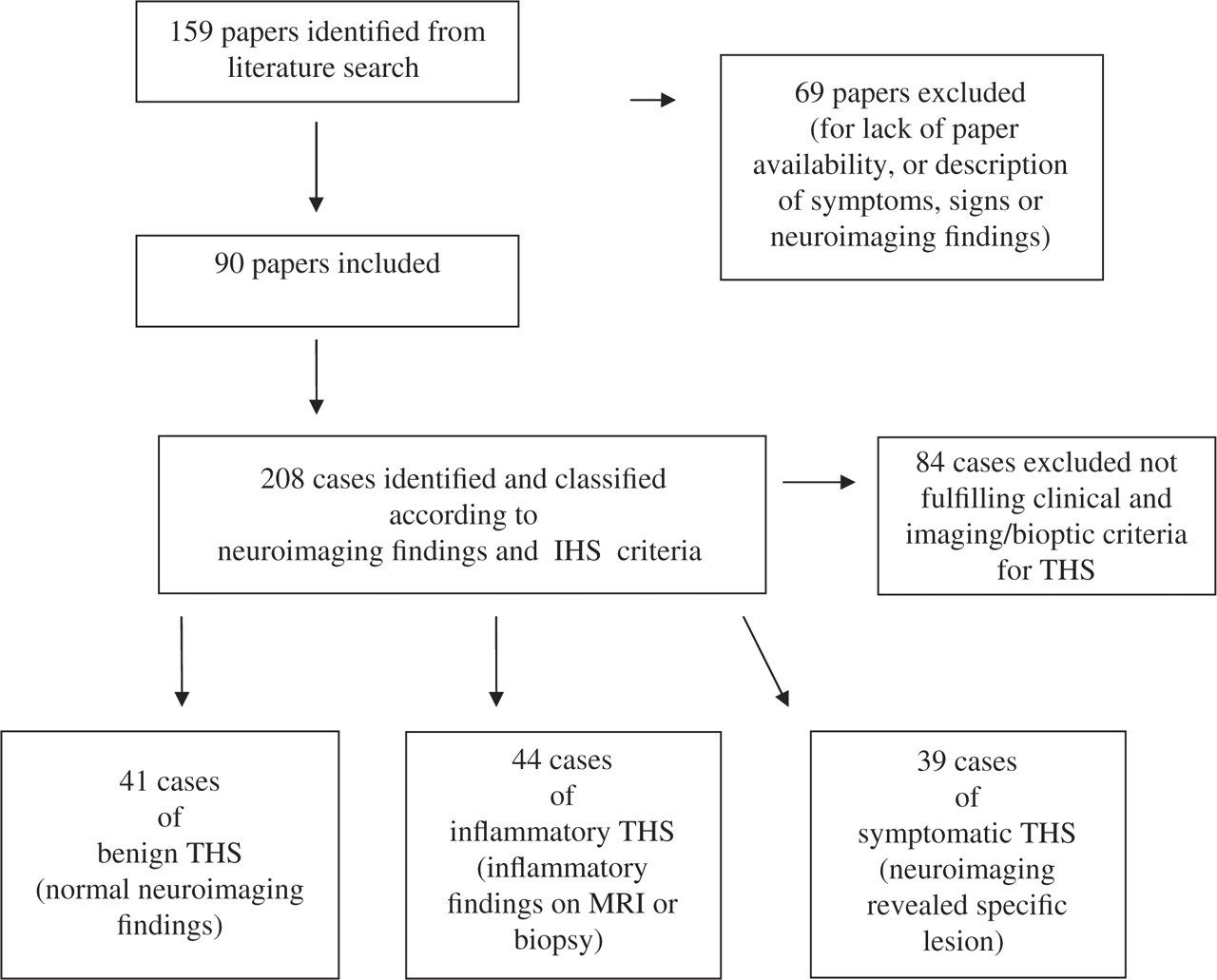
Procedure for literature review on Tolosa–Hunt syndrome, with data on cases identified
Papers on Tolosa–Hunt syndrome (THS) published between 1988 and 2002, with number of cases contributed according to diagnostic category (benign, inflammatory, symptomatic, or excluded) and reasons for exclusion



Inflammatory cases with biopsy performed.
Diseases responsible for symptomatic Tolosa–Hunt syndrome

Clinical findings
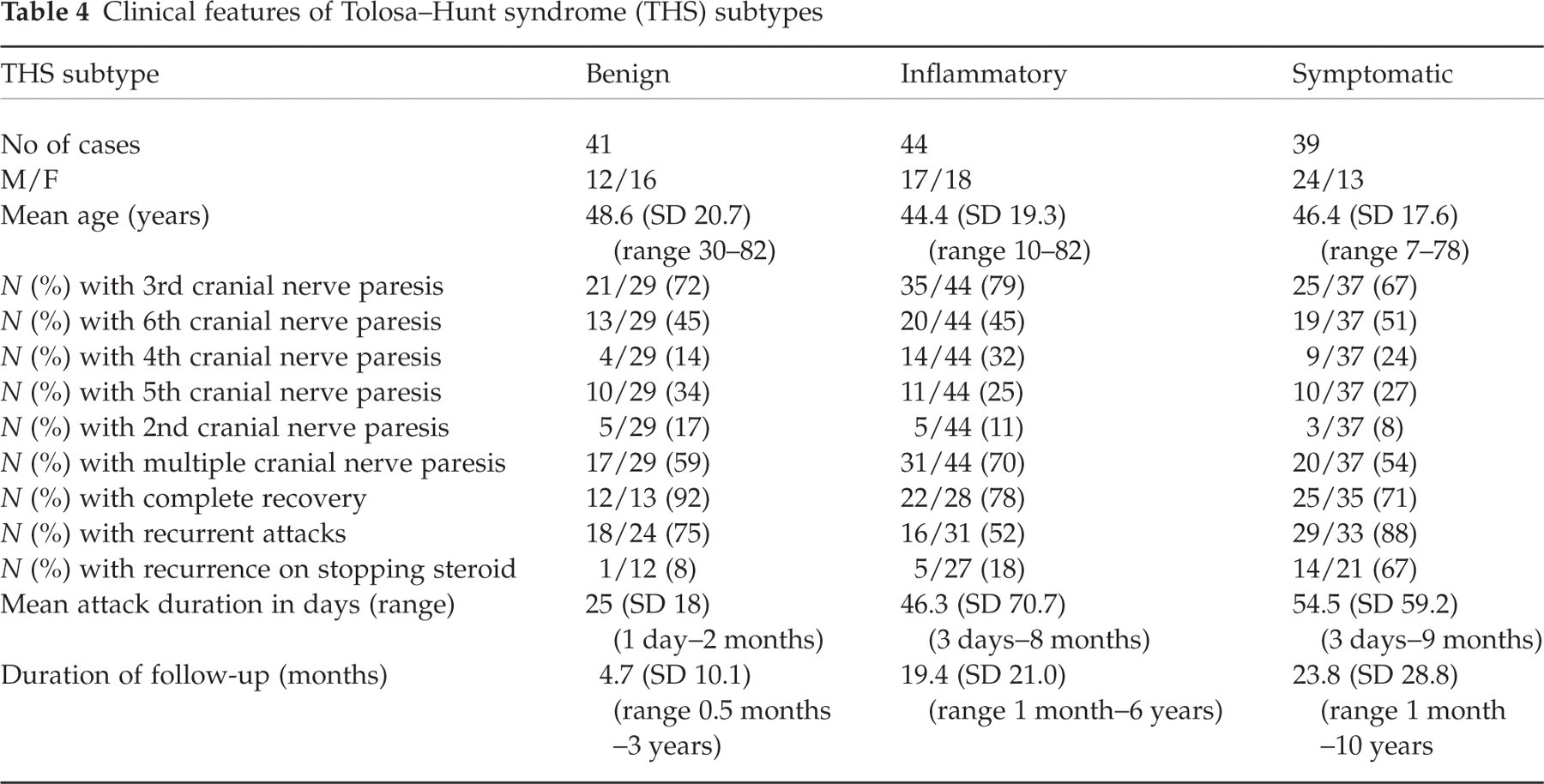
The clinical features of the three types of THS identified (benign, inflammatory and symptomatic) are summarized in Table 4 and are based on the available data clearly reported in the studies. There were no significant differences between these types in terms of sex, age or cranial nerve involvement. The third cranial nerve was most commonly involved in all groups. However, symptomatic THS cases were characterized by more frequent (88% of symptomatic cases) recrudescence on steroid withdrawal and slightly longer attack duration, than patients with benign or inflammatory forms. In most cases the data available did not specify clearly whether the paresis and pain responded to steroids within 72 h.
Clinical features of Tolosa–Hunt syndrome (THS) subtypes
Imaging and biopsy
When a lesion consistent with granuloma was revealed it was usually confined to the cavernous sinus, but could also extend to the superior orbital fissure or the orbital apex. On MRI, lesions enlarged the cavernous sinus, were isointense on T1-weighted images and enhanced markedly after contrast administration. MRI detected a lesion in seven patients with normal CT scan (47%) of the 15 cases examined with MRI and CT. The lesion diminished or disappeared during follow-up (range 1 week to 1 year) in the cases with reported follow-up. The granuloma diagnosis was confirmed by biopsy in eight cases (see Table 2).
Discussion
The new IHS diagnostic criteria for THS (Table 1) require demonstration of granuloma by MRI or biopsy. We found that only 44 (21%) of the 208 literature cases identified in the period 1988–2002 would be classified as THS according to the new criteria, in particular providing imaging or bioptic evidence of granuloma. In addition, 41 cases with clinical presentation and diagnosis of THS had normal neuroimaging findings, while another 39 had a clinical presentation suggesting THS, but neuroimaging revealed a specific intracranial lesion. These findings show that clinical features suggesting THS are not specific for that syndrome but are common to several conditions, and that their presence alone does not guarantee the correct diagnosis.
Our analysis indicated that MRI is extremely useful for expediting the diagnosis. In particular, MRI detected a lesion in about the half of CT-negative patients, presumably because MRI is able to provide better resolution of the soft tissue adjacent to the cavernous sinus. However, the criteria for demonstrating granuloma by MRI have not been defined. We suggest that the acquisition protocol should include T1 weighting, Turbo-T2, FLAIR and T1 weighting after contrast, in order to demonstrate the probable inflammatory nature of the lesion. We also feel that resolution of the inflammation should be confirmed by MRI following treatment to verify the diagnosis, as emphasized by
About a third of the cases with clinical presentation suggesting THS had normal MRI findings. Modern MR equipment, and a defined protocol, would probably reduce the proportion of such cases by identifying more lesions. However, it is probable that a certain proportion of these ‘benign’ THS cases will continue to be diagnosed: the problem of their nosography remains.
The new IHS diagnostic criteria for THS also require response of the paresis, as well as the pain, to adequate corticosteroid treatment within 72 h. Most of the cases examined in this review did not contain data on the time and extent of recovery after steroid therapy (of either the pain or the paresis); furthermore, steroid dosing schedule, whether the condition recurred after steroid removal, and attack duration, were clearly reported in only a minority of cases. It is therefore difficult to draw conclusions on these aspects from our analysis. However, it is noteworthy that the symptomatology recurred after steroid withdrawal in a considerable proportion of patients with a symptomatic condition (Table 4), suggesting that this may be a useful clinical sign pointing to secondary THS.
Forderreuther et al. (8), Drouot et al. (92) and Pascual et al. (68) have previously suggested revision of the 1988 IHS criteria for THS diagnosis, and have also emphasized the need for follow-up for at least 2 years to confirm the diagnosis. Our analysis suggests that although the IHS 2004 criteria may allow more detailed classification of painful ophthalmoplegias, they require further revision, including detailed specification of the MRI protocol necessary to reveal the diagnosis, and definition of a nosographic category to contain THS cases with normal MRI findings.
Acknowledgements
We thank Don Ward for help with the English and critically reviewing the manuscript; and Ms Alessandra Atterrato (assistant librarian) for retrieving the papers.