
Abstract
Background
To examine national trends in medication-overuse headache (MOH) hospitalisation rates, length of hospital stays, and patient demographics in Australia in the context of evolving access to medications implicated in MOH.
Methods
A retrospective analysis of national hospital admissions data from the Australian Institute of Health and Welfare (AIHW), focusing on cases with a principal diagnosis of MOH from 2009 to 2024. MOH hospitalisation rates per 100,000 population and length of hospital stay were analysed over time and stratified by age group and sex.
Results
A total of 2480 MOH cases were identified over 16 years, including 1661 (67%) females and 954 (38.5%) individuals aged > 60 years. Overall MOH-related hospitalisation rates declined (IRR: 0.97; 95% CI: 0.96–0.98), as did the average length of stay per admission (−0.035 days/year; p = 0.036). Females were more likely to be admitted (IRR: 1.95; 95% CI: 1.79–2.12), as were older patients (IRR: 8.08; 95% CI: 6.77–9.65); however, longer stays were observed only among older patients (mean [SD]: 2.74 [0.48] vs. 2.21 [0.37] days; p = 0.005).
Conclusion
This trend, occurring alongside rising migraine-related hospitalisations, the phasing out of ergotamine, and increased triptan use, may be partially attributed to the 2018 codeine rescheduling. Future studies using detailed prescription data are warranted to assess the long-term impact of medication policy changes on MOH trends.
This is a visual representation of the abstract.
Introduction
Medication Overuse Headache (MOH), as defined by the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria (1), includes cases with (i) a headache occurring on 15 or more days per month, (ii) a pre-existing headache disorder, and (iii) regular overuse of acute headache medications for more than three months, where no better diagnosis explains the clinical presentation. MOH significantly impairs quality of life, reduces productivity, and increases healthcare utilisation in both high- and low-income countries (2,3).
Globally, MOH represents a substantial public health concern. A systematic review of studies from 16 countries reported that MOH affects approximately 1–2% of the general population, with estimates ranging from 0.5% to 7.2% (4,5). The 2016 Global Burden of Disease (GBD) study ranked migraine as the second leading cause of disability, in part due to MOH being considered a sequela of both migraine and tension-type headache (3). In a population-based study from Greece, MOH was reported in 50.5% of individuals with chronic migraine and 45.9% with chronic tension-type headache (6). Similarly, a study from Germany found that approximately 50% of patients with chronic migraine met criteria for MOH (7). Yet, despite the high estimated incidence and burden, few population-based studies have investigated the incidence of MOH. One study involving patients with episodic migraine reported a 14% one-year incidence of chronic headache, and 10% of them reported overuse of headache medications (8).
In clinical settings, MOH accounts for up to 30% of cases in European headache centres and over 50% in the US (9). The most severe cases often require hospital admission, posing a substantial burden on both patients and the healthcare system (10). The proportion and complexity of these admissions (e.g., hospital length of stay) are influenced by factors such as the type of overused medication and the underlying primary headache disorder (11,12).
Triptans, ergotamines, and opioids such as codeine are all associated with MOH (13–15). Long-term use and overuse of opioids are associated with a higher risk of developing MOH and poorer clinical outcomes compared to triptans or ergotamines (16,17). While there is limited evidence that codeine alone poses a higher risk for MOH compared to other opioids, use of combination analgesics containing codeine is identified as a significant risk factor (14). Codeine is frequently combined with paracetamol for headache management and was available over the counter in Australia until its rescheduling in 2018. This greater accessibility may have contributed to increased use and potential overuse, thereby raising the risk of MOH. One study in Australia also found that 90% of patients admitted for MOH had a prior history of migraine, with codeine implicated in 80% of analgesic rebound headaches and ergotamine in 24% (18). The types of acute medications used to treat MOH vary significantly between countries (19).
Migraine is the leading cause of disability in Australia, affecting approximately 4.9 million people (20). According to 2019 estimates, approximately 250,000 Australians experience MOH (21). Self-medication with over-the-counter (OTC) codeine in Australia has contributed significantly to the MOH burden (22). In recent years, Australia has made significant changes to the availability of medications associated with MOH, including the 2018 restriction of OTC codeine, the effective phase-out of ergotamine-containing products by 2015 and the introduction of OTC triptans from 2021 (23–25). Hospital admissions are one key indicator for evaluating the potential impact of these changes in medication access. Analysing trends across the population and within specific subgroups can help reveal the effects of such policy changes (5,26). It is therefore timely to examine trends in hospital admissions for MOH.
This study aimed to evaluate the temporal trends of MOH hospitalisation rates, duration of hospital stays, and demographics, given the changes in access to medications implicated in MOH over the past 16 years in Australia.
Methods
Study design and data source
A retrospective study was conducted using 16 years of hospital admission data for MOH in Australia from 2009 to 2024. Data were retrieved from the Australian Institute of Health and Welfare (AIHW), which provides aggregated and de-identified publicly accessible retrospective health datasets covering hospital admissions, aged care, and mental health (27). These datasets are updated periodically, including demographics, diagnoses, services, and outcomes. The use of publicly available, aggregated, and de-identified data was considered exempt from requiring ethics approval, as confirmed by the Monash University Ethics Committee.
Participants
We identified admissions with a diagnosis of MOH during the study period using the International Classification of Diseases, 10th Revision (ICD-10) code G44.4, “Drug-induced headache, not elsewhere classified.” Yearly MOH hospital admissions data were extracted and stratified by age group, sex, and length of hospital stay. Only patients with MOH recorded as a primary diagnosis were included in the analysis to ensure accurate identification of cases. The yearly total population of Australia by age group and sex from the same period was extracted from the Australian Bureau of Statistics (ABS) website (28) and used as denominators to calculate the hospitalisation rate based on age group and sex. Admission age was categorized into four groups: under 20 years, 20–39 years, 40–59 years, and 60 years and above.
Outcomes
The primary outcome was the trend in MOH hospitalisation rate per 100,000 population over time. MOH admission rates per 100,000 population were calculated by dividing the number of admissions each year by the total population for that year. The secondary outcome was the mean length of hospital stay, calculated by dividing the total yearly hospital stays by the number of admissions.
Statistical analysis
All admissions with a diagnosis of MOH during the study period were included, and as the sample represented a complete national dataset, no a priori sample size calculation was performed. As data were aggregated, missing values were not reported.
Yearly rates of MOH per 100,000 population and the proportion of hospital stays that were same-day discharges versus multiple-day admissions were plotted and stratified by age and sex. Poisson regression was used to analyse the overall trends in MOH hospitalisation rates, adjusted by age group and sex. A generalised linear model with a binomial distribution was used to estimate yearly changes in the proportion of discharge type over time. Additional linear regression was employed to examine yearly changes in the length of hospital stay over time.
The Shapiro–Wilk test was used to assess the normality of the length of hospital stay across age groups and sexes. Since the data were normally distributed, independent t-tests were conducted to compare the mean length of hospital stay across age groups and sexes, with results presented as mean ± standard deviation (SD). A two-sided p-value of <0.05 was considered statistically significant. Data analysis and visualisation were performed in RStudio (R 4.4.2).
Results
We identified 2480 hospital admissions with the diagnosis of MOH between 2009 and 2024. Of these, 1661 (67%) admissions were represented by females, and 954 (38.5%) admissions involved people aged over 60 years (Online Supplementary Table S1). As shown in Figure 1, admission rates increased steadily to a peak of over 0.85 per 100,000 in 2012 and 2014, followed by a sharp decline to 0.48 per 100,000 in 2015. A marked increase in MOH hospitalisation was observed in 2021 and 2022, with rates reaching 0.84 and 0.76 per 100,000, respectively. These values fell outside the 95% confidence interval of the overall trend line and likely reflect the impact of the COVID-19 pandemic during that period. Thereafter, the rates of hospital admission showed a significant downward trend, with the rate dropping to its lowest points of 0.37 and 0.34 per 100,000 in 2023 and 2024, respectively (Figure 1). Although the trends appeared to fluctuate over the years, Poisson regression analysis indicated a significant decrease in overall annual MOH hospitalisation rates over time (IRR = 0.97; 95% CI: 0.96–0.98), corresponding to an average 3.1% reduction in rates per year, with a modest model fit (McFadden R² = 0.15). Overall, MOH hospitalisation rates were significantly higher across all other age groups compared with those <20 years (Figure 2). Rates were over threefold higher in the 20–39 group ([IRR] = 3.54; 95% CI: 2.95–4.24), nearly sixfold higher in the 40–59 group (IRR = 5.88; 95% CI: 4.93–7.04), and more than eightfold higher in the 60 + group (IRR = 8.08; 95% CI: 6.77–9.65) (Online Supplementary Table S2). Female patients had nearly twice the rate of MOH hospitalisations compared with males (IRR = 1.95; 95% CI: 1.79–2.12), although rates in both sexes declined over the study period (Figure 3, Online Supplementary Table S2).

Trends in medication overuse headache (MOH) hospitalisation rate per 100,000 population in Australia, 2009–2024.

Medication overuse headache (MOH) hospitalisation rate by age groups per population over time, 2009–2024.
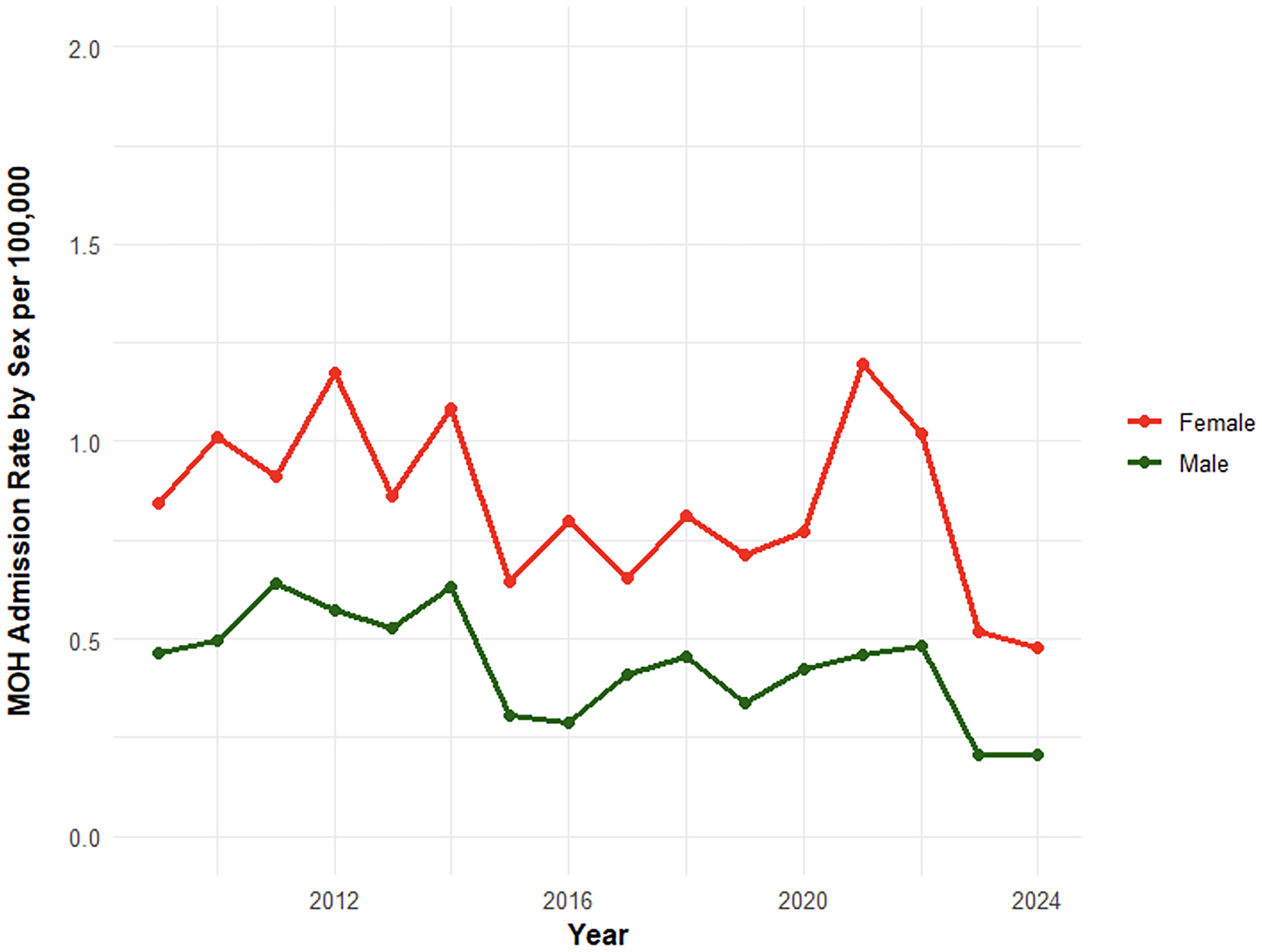
Medication overuse headache (MOH) hospital admission rate by sex over time per population, 2009–2024.
The average length of hospital stays for MOH admission was 2.40 days (SD = 0.31) during the study period (Online Supplementary Figure S1). Hospital stays per MOH admission significantly declined over time, with an average decrease of 0.035 days per year (p = 0.036). Individuals aged >60 had a significantly longer average hospital stay per MOH admission compared to those aged <60 (mean [SD]: 2.74 [0.48] vs. 2.21 [0.37] days; t (28.24) = -3.05, p = 0.005). However, the difference in average hospital stay was not statistically significant between females and males (mean [SD]: 2.47 [0.48] vs. 2.33 [0.32] days; t (27.3) = 1.06, p = 0.300) (Online Supplementary Figure S2, Table S3). The proportion of patients with multiple-day admissions showed an overall significant decreasing trend (log-odds slope = −0.0504 per year, p < 0.001), while same-day discharges exhibited a significant increasing trend (log-odds slope = + 0.0504 per year, p = 0.002) (Figure 4, Online Supplementary Table S4).

Discharge types for medication overuse headache hospitalisations over time, based on same-day and overnight admissions, 2009–2024.
Discussion
This study examined 16-year trends in hospitalisations for MOH in Australia, focusing on the length of hospital stay and demographic changes over time. We observed an overall decline in MOH hospitalisation rates, despite a peak in 2021 and 2022. Concurrently, the average length of stay decreased over time, driven by an increase in same-day discharges and a reduction in multiple-day admissions.
Multiple factors may have contributed to these patterns. Historically, codeine was the primary agent implicated in 80% of MOH hospitalisations and was associated with longer admissions (18,29). The observed reductions in MOH hospitalisation rates and length of stay may be partly attributed to the codeine rescheduling. Evidence indicates that following the rescheduling, there was a decline in codeine prescribing, codeine-related poisoning calls, and hospital presentations (22,30,31). These reductions occurred alongside increased national use of triptans (25) and a concurrent rise in migraine-related hospitalisations over time (32).
A recent study revealed an increase in codeine prescriptions among females and migraine patients after rescheduling, potentially explaining the delayed hospital admissions as patients transitioned from OTC to prescribed codeine (33). However, establishing a direct association between MOH hospitalisation and codeine rescheduling is complex due to the presence of multiple confounders. First, the pathophysiology of MOH remains poorly understood, yet it is known to develop gradually, meaning that any impact of medication changes may take several years to appear rather than occurring at a specific time point soon after a change in codeine availability (26,34). Second, the period following the 2018 codeine rescheduling overlapped with the COVID-19 pandemic, which was associated with increased migraine and MOH hospitalisations due to heightened stress, anxiety, and disrupted access to healthcare services (35,36). The spike in admissions during COVID may reflect ineffective self-management attempts due to reduced access to routine care (37,38). Third, while codeine is a major contributor to MOH, other medications such as ergotamine and triptans also contribute to MOH, and access to these medications has changed meaningfully over the past two decades (39). Another factor that probably contributes to reduced requirements for admission over time is greater access to highly effective prophylaxis, such as OnabotulinumtoxinA (listed on the Pharmaceutical Benefits Scheme (PBS) in 2014) and CGRP (calcitonin gene-related peptide) antibodies (listed on the PBS in 2021) in Australia (40,41). The overall declining trends in MOH hospitalisations and length of stays, occurring alongside the phasing out of ergotamine and increased triptans use in Australia (25), suggest that the policy shift on codeine may have contributed to these trends, but there may have been multiple contributing factors. These complex trends highlight the need for further research to identify current MOH-contributing medications in Australia and to evaluate the long-term effects of regulatory changes.
MOH is most commonly reported among females and individuals aged 30 to 50 years, with a lower incidence in males and older adults (42,43). However, contrary to prior assumptions that MOH peaks in midlife and declines thereafter, our study found an age-related increase in MOH-related hospitalisations, with over one-third of admissions occurring in patients over 60 years. This may reflect the impact of comorbidities, polypharmacy, and delayed or atypical presentations in older adults, all of which complicate outpatient management and necessitate inpatient care (44–46). We also found that longer stays due to MOH were more common among individuals over 60 years old, likely reflecting both higher admission rates and greater illness severity in older adulthood. Longer hospital stays in older MOH patients may partly reflect unrelated comorbidities. Interventions such as geriatric assessment, multidisciplinary care, and individualised medication review may help optimise management and reduce length of stay.
The observed reduction in length of stay over time may reflect not only the impact of medication policy changes, but also increased education and understanding of the disease (47), as well as broader systemic pressures within the hospital setting. While such factors could not be directly assessed in this study, our findings support the notion that more detailed research is warranted, including future studies incorporating hospital-level data to better understand their role in shaping LOS trends for MOH-related admissions.
Consistent with previous studies, MOH-related hospitalisations were more common in females than in males (35,43). In our study, the female-to-male incidence rate ratio for MOH hospitalisations was higher. This aligns with previous research reporting a similar female predominance in both MOH and migraine, with female-to-male ratios typically ranging from 2:1 to 5:1 (43,45,48). The consistency in sex distribution supports the hypothesis that MOH often arises as a sequelae of migraine. Although sex-based differences in MOH-related hospitalisation are not well characterised, potential explanations include sex-related differences in comorbidity burden, migraine pathophysiology, sex-specific differences in pain perception, and differences in healthcare-seeking behaviour (48–50).
Strengths and limitations of the study
A key strength of this study is the use of nationally representative data from the Australian Institute of Health and Welfare (AIHW), which enhances the generalisability of the findings. To our knowledge, this is the first study to examine national trends in hospital admission rates and lengths of hospital stay for MOH. Although exact percentages are not well documented, evidence indicates that most cases of MOH are managed in outpatient settings (51,52). As hospitalisation and prolonged inpatient stays are generally considered indicators of outpatient management failure or severity of illness (11), the cases in this series likely represent only a fraction of the total burden of MOH. Yet, examining the most severe cases provides important insights into emerging trends and highlights priority areas for intervention.
As with all studies using population-level administrative data, this study has several limitations. First, the analysis is limited to inpatient admissions and does not capture MOH treatment in outpatient settings. Second, the data were presented in aggregate format, restricting the ability to examine variability in individual hospital stays, particularly those of longer duration. Third, no existing dataset provides detailed information on the specific medications or drug classes overused, which prevented us from conducting subgroup analyses (e.g., opioids vs non-opioids, triptans vs non-specific agents). While we were not able to analyse changes in individual medicine types, an analysis of PBS data and published literature revealed that the supply of triptans increased over the study period (25,53). From 2010 to 2020, dispensing increased by approximately 1.4% per month before 2021. After the down-scheduling in 2021, PBS dispensing continued to rise, but at a slower rate of about 0.6% per month. The supply of codeine was high from 2010 to 2017, with a temporary rise noted immediately following codeine rescheduling, but it has been in gradual decline since 2020 (54,55). Future studies using linked prescription data may offer greater insight into these patterns. Lastly, case identification was based on ICD codes, which may be impacted by misclassification. To minimise confounding from unrelated comorbidities, only admissions with medication-overuse headache (MOH) recorded as the primary diagnosis were included. Due to limitations in the ICD-10 coding granularity available within the dataset, MOH could not be isolated using the specific code G44.41. Instead, the broader code G44.4 (“Drug-induced headache, not elsewhere classified”) was used as a proxy. This may have included other types of drug-induced headache, introducing misclassification bias. While all MOH cases are drug-induced, not all drug-induced headaches are due to medication overuse. Although specific epidemiological data on the prevalence of MOH within drug-induced headaches are lacking, MOH is generally considered the most common subtype and is often used interchangeably with the broader term ‘drug-induced headache’ in clinical practice and the literature (5,45). Further, there is no clear reason to suspect that misclassification varied systematically over time or across specific population subgroups. Therefore, the observed trends among identified cases are likely to remain valid indicators of broader patterns.
Conclusion
Hospitalisation rates and lengths of stay for medication-overuse headache (MOH) have declined over time, potentially reflecting changes in community-level access to medications associated with MOH. These findings highlight that MOH presentations are not static, with considerable temporal trends in patient characteristics. Hospitalisations—representing the most severe MOH cases—were more common among females and adults over 60; however, only older adults experienced longer hospital stays. Targeted interventions focusing on these populations could help reduce the burden of MOH on the healthcare system.
The decline in MOH hospitalisations may reflect the phasing out of ergotamine, increased access to triptans through scheduling changes, and the impact of codeine rescheduling, highlighting how medication policy changes can shape MOH trends and healthcare utilisation. Females and individuals aged 60 and above were consistently overrepresented, underscoring key demographic variations relevant for targeted interventions.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251404451 - Supplemental material for Medication-overuse headache hospitalisations in Australia, 2009–2024: A national study of a preventable condition
Supplemental material, sj-docx-1-cep-10.1177_03331024251404451 for Medication-overuse headache hospitalisations in Australia, 2009–2024: A national study of a preventable condition by Dereje Zewdu Assefa, Ting Xia, Richard J. Stark and Suzanne Nielsen in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024251404451 - Supplemental material for Medication-overuse headache hospitalisations in Australia, 2009–2024: A national study of a preventable condition
Supplemental material, sj-docx-2-cep-10.1177_03331024251404451 for Medication-overuse headache hospitalisations in Australia, 2009–2024: A national study of a preventable condition by Dereje Zewdu Assefa, Ting Xia, Richard J. Stark and Suzanne Nielsen in Cephalalgia
Footnotes
Author contributions
DZA: Conceptualization, Data curation, Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing; TX: Data curation, Formal Analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing; RJS: Conceptualization, Writing – original draft, Writing – review & editing; SN: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing
Data availability statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The use of publicly available, aggregated, and non-identifiable data was considered exempt from requiring ethics approval, as confirmed by the Monash University Ethics Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DZA is supported for his PhD study by the Monash Graduate Scholarship (MGS) and Monash International Tuition Scholarship (MITS). SN is the recipient of a National Health and Medical Research Council (NHMRC) Investigator Grant Fellowship (#2025894).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.