
Abstract
Background
Headache is a leading cause of disability and a major public health problem worldwide. Although most patients with headaches are managed in primary care settings, including chiropractic clinics, there are few studies describing the prevalence of headache and headache diagnoses in primary care. The present study aimed to: (1) estimate the prevalence of headache consultations in chiropractic practice; (2) estimate the prevalence of different headache diagnoses used in chiropractic practice; and (3) determine the association between the prevalence of headache consultations and chiropractor characteristics.
Methods
All chiropractors in Denmark, who were members of the Danish Chiropractic Association, (n = 695) were invited to participate. Data collection for this cross-sectional study was based on a survey and a 20-day logbook and took place in 2022. The survey collected information on various characteristics of the chiropractors who completed the logbook. The logbook recorded the total number of consultations, whether the reason for the consultation was related to headache, the type of diagnosis, the type of consultation (e.g. new patient, maintenance care), and whether the headache was the primary or secondary reason for the consultation. We used weighted linear regression analyses with robust standard errors for determining associations between prevalence and chiropractor characteristics.
Results
In total, 76 chiropractors participated, reporting a prevalence of 12% for consultations including any type of headache. The response rate was 10.9%. The prevalence of headache-related consultations per chiropractor varied from 0% to 38% (median = 12.1; interquartile range = 8.2–15.5). In 43.6% of all headache consultations, headache was the main reason for consulting a chiropractor. The most common type of headache was tension-type (36.2%), followed by combinations of headache types (34.4%), with the most common combination being tension-type and cervicogenic headache. Headaches were reported in 12% of all new consultations and 25% of all maintenance care consultations. There were no associations between the prevalence of headache consultations and chiropractor characteristics.
Conclusions
Patients with headaches, especially tension-type headaches and patients with more than one type of headache, were common in chiropractic clinics, with 12% of all consultations related to headaches. In two out of every five consultations related to headaches, the headache itself was the primary reason for visiting the chiropractor, rather than a secondary symptom accompanying another condition such as neck pain
This is a visual representation of the abstract.
Introduction
Headache is one of the leading causes of disability and a major public health concern worldwide (1–3). In the context of worldwide impact, a narrative review of 357 publications in 2022 showed that 15.8% of the world's population have a headache every day (3). The estimated global (mainly high-income countries) one-year prevalence of headache disorder was 53.5% (95% confidence interval (CI) = 48.9–55.4), with migraine affecting 15.3% and tension-type headache impacting 26.4% of the population (3). In Denmark, the impact of headaches is equally noteworthy. According to Danish nationwide surveys, almost one-third of the population have sought help from a primary care provider for headache (4) and, among people with headache, one-quarter reported that they were unable to manage their headache attacks sufficiently (5). The survey revealed low care-seeking despite a perceived need and concluded that healthcare utilisation patterns among people with headache suggested the inadequate provision of headache care in Denmark (5).
Primary care is where most patients with headache are managed, and timely, consistent and multidisciplinary management in primary care is likely to reduce costly and unnecessary examinations and referrals to specialists in secondary care (6). However, a recent study of patients with headache in Danish general practice (7) found that half the patients were referred to a secondary care neurologist; however, the recommendation was that most patients should be managed in primary care.
National guidelines on managing patients with headaches (8–11) support non-pharmacological interventions such as patient education, physical activity and exercise, and manual therapy, all of which are included in management strategies provided by chiropractors and physiotherapists in primary care. In Denmark, chiropractors are regulated by the National Health Authority and the cost of treatment for the patient is partly covered by the Danish Health Insurance System. Danish chiropractors are encouraged to follow a profession-specific clinical care standard for the assessment of headaches, developed by the Danish Society of Chiropractic (12). The care standard recommends the use of the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria for primary and secondary recurrent headaches (13) when diagnosing patients with headaches and includes recommendations for medical history, examination, diagnosis and management (12). However, it is not known which diagnoses are identified in patients with headache and to what extent clinical standards are followed.
While the effect of non-pharmacological treatments for tension-type headache, migraine and cervicogenic headache have been investigated in several studies (14–17), studies on the prevalence of headaches in primary care remain sparce. A 2018 review found headaches to be among the top 10 reasons for consulting a general practitioner (18), with point prevalence rates in general practice of 5.4% and one-year prevalence rates ranging from 1.5% to 3.2% (19–21). To our knowledge, there are no studies describing the prevalence of headaches managed in physiotherapy practice and only one Australian study in chiropractic practice (22). The Australian study reported that one in five new patients presenting to chiropractic clinics over a two-week period consulted for headache (22).
A 1999 Danish survey by Hartvigsen et al. (23), describing the characteristics of chiropractic patients in Denmark, reported that 8% of patients seen in chiropractic clinics were people suffering from headaches. However, the Danish survey study by Hartvigsen et al. (23) included only new patients and did not record specific headache diagnoses. The lack of more recent and comprehensive data highlights the need for up-to-date evidence to raise awareness among patients consulting chiropractors for headaches, and to help understand their healthcare needs. Therefore, the aims of this study were (1) to estimate the prevalence of headache consultations in chiropractic practice; (2) to estimate the prevalence of different headache diagnoses identified in chiropractic practice; and (3) to determine the association between the prevalence of headache consultations and chiropractor characteristics such as age, sex, knowledge of the Danish profession-specific clinical care standard, knowledge of the ICHD-3 criteria, and clinical experience.
Methods
The reporting of this study conforms to the STrengthening the Reporting of Observational studies in Epidemiology (STROBE) statement (24).
Study design
This study was a survey-based cross-sectional study conducted in 2022.
Setting
The study was conducted among Danish chiropractors working in private practice. In Denmark, chiropractors are independent private contractors regulated by the Danish National Health authorities (25). The health authorities have the power to influence primary care services to maintain the quality and safety of care by ensuring that health professionals practice in accordance with current national clinical guidelines on clinical competence. The terms of regulation are negotiated in a collective agreement between the Danish Chiropractic Association (DCA) and the Danish National Health authorities.
Participants
All Danish chiropractors, including chiropractors in postgraduate internship, who were members of the Danish Chiropractic Association in March 2022, were invited by personal email to participate in the data collection. Additional information about the study was provided via webinars and written materials. To identify chiropractors who did not have clinical work in primary care and therefore could not contribute to the data collection (e.g. researchers, chiropractors in public hospitals, chiropractors with university posts), the response option “do not manage patients in primary care” was included as part of the consent form. To increase awareness of the project, it was also promoted through newsletters, social media, conferences and webinars, and personal contacts.
Data collection and variables of interest
The data collection commenced in May 2022 and ended in August 2022. We utilized the newly developed Danish Headache Questionnaire (DHQ) (26), which included a questionnaire-based online survey and a 20-day logbook registration of consultations concerning headaches. The DHQ was developed through three pilot tests with Danish chiropractors, leading to the final version. The DHQ consists of an introductory page that introduces the survey, the logbook and the content, along with estimated time consumption (20–30 minutes) for the survey and information about anonymity. No incentives were offered to participate and participation was voluntary. Participants received reminders one and two weeks after receiving the survey and they also received reminders to fill out the logbook after seven and 11 weeks. A detailed description of the development and content of the DHQ has been described previously (26) and the full questionnaire is available at a website on commonly used questionnaires (27).
The survey
The following variables were included based on previous literature and clinical experience: age, gender, years in practice, knowledge of Danish profession-specific clinical care standard, and knowledge of diagnostic criteria. Gender was categorized as “male”, “female” and “other gender identity”, and years in practice as “postgraduate internship”, “1–4 years”, “5–10 years”, “11–15 years” and “more than 15 years”. Chiropractors were asked to what extent they were familiar with the content of the clinical care standards, with the response options “yes, all of it”, “most of it”, “parts of it” and “no”. Similarly, they were asked to indicate their level of familiarity with the ICHD-3 criteria using the response options “very familiar”, “moderately familiar”, “slightly familiar” and “not at all familiar”. The data collection was managed using the Research Electronic Data Capture system (REDCap) (28,29) hosted at OPEN (Open Patient data Explorative Network, Odense University Hospital, Region of Southern Denmark) (30).
The logbook
To measure the prevalence of headache consultations, both the number of headache consultations and the total number of consultations (regardless of diagnosis) were recorded in a logbook over 20 working days. The registration period was set at 20 prospective working days to accommodate variations due to holidays, part-time schedules and sickness absence. For patients with a headache diagnosis, the chiropractor recorded the patient's date of birth, headache diagnosis made by the chiropractor, consultation type, and whether the headache was the primary or secondary reason for seeking care. A secondary reason could be, for example, a headache in addition to neck pain. The response options for diagnosis were pre-specified and included tension-type headache, migraine and cervicogenic headache because these are common headaches seen in chiropractic practice (3,31,32). Participants also had the option of selecting “other” and writing the diagnosis in the text box provided. It was possible to report more than one diagnosis. If more than one diagnosis was recorded, it was defined as having co-existing headaches.
The consultation type had four pre-specified options: “new patient”, “new problem”, “existing patient” or “maintenance care”. A “new patient” was defined as someone seeking care for a headache who had not previously visited the clinic. A “new problem” referred to an individual who was already acquainted with the clinic but was now seeking care for a headache as a new issue. An “existing patient” was someone who had started treatment for headache prior to the registration period and was in a course of treatment. A “maintenance care” patient was defined as a patient who was seen on an as-needed basis and was not in a course of treatment. As the registration was consultation-based, the same patient could be registered several times during the 20-day period, whereas the category “new patient” was only used once per patient. This implies that, for a “new patient” who was seen again, the headache was registered each time, and subsequent consultations were categorized as “existing patients”.
Statistical analysis
The chiropractor characteristics were presented through absolute and relative frequencies, as well as medians with interquartile ranges. A 20-day prevalence with 95% CIs was calculated for headache consultations. If no diagnosis was registered during a consultation, it was categorized as “not reported”. The results were reported in tables or graphically as appropriate. The statistical significance of associations between prevalence and chiropractor characteristics was assessed using weighted linear regression analyses, giving greater weight to clinicians with more consultations. To address heteroskedasticity identified in model diagnostics, we applied robust standard errors to obtain valid statistical inference. The characteristics assessed were: age, sex, experience (years in practice), high knowledge of the diagnostic criteria for different headache types (dichotomized into “very familiar” versus “not at all to moderately familiar”) and high level of familiarity with the content of the Danish profession-specific clinical care standard. A stratified analysis of headache type by age using a subset of “new patients” was performed. We did not have discrete data on individual patients from the logbook registrations, only age on the person consulting, and therefore it was not possible to do an analysis on all patients. However, the proportion of “new patient” consultations involving headache can be considered a proxy for the prevalence of new headache patients because these encounters are more likely to represent unique individuals. Therefore, we were able to report age data for new patients, which we have used as a proxy to describe the age distribution of new headache presentations to chiropractors. Age by headache type for new patients was presented as mean age with 95% CI. The statistical significance of age as a predictor of headache type was assessed using a multinomial logistic regression model.
Statistical analyses were based on data from chiropractors with fully completed logbook registrations. STATA, version 17.0 (StataCorp, College Station, TX, USA) was used for data analyses. p < 0.05 was considered statistically significant.
Results
In total, 695 chiropractors were invited to participate in the study. Five hundred and thirty-nine (78%) did not respond, 38 (5%) either declined to participate or did not work in primary care and 118 (17%) agreed to participate. Three withdrew from the project, four never registered any data and, of the final 111 participants, 100 completed the questionnaire (90%). In total, 76 chiropractors returned the logbook (68% of those who agreed to participate), resulting in an overall response rate of 10.9% (95% CI = 8.6–13.3%) (Figure 1). Of the logbook registrations, 72 (65%) completed all 20 days.

Flowchart of participants. *Only responded to the questions about clinic data. **No registration of total number of consultations regardless of diagnosis.
Seventy-six chiropractors (48 female; 64%) with a median age of 41 years (interquartile range = 29–51) completed the logbook registration, with most of the respondents located in the Region of Southern Denmark (41%) (Table 1). Most chiropractors (88.2%) worked alongside at least one other chiropractor, with a median of four chiropractors per clinic. Approximately half of the chiropractors worked alongside either a physiotherapist or a massage therapist (54% and 47%, respectively). The majority of the chiropractors had more than 15 years of experience in practice (range 0–15 years) and were familiar with the Danish profession-specific clinical care standard for headaches, with only three (4%) stating that they were not. Among the chiropractors, 56 (87%) were moderately to very familiar with the ICHD-3 (33) diagnostic criteria for tension-type headache, 68 (89%) for migraine and 67 (88%) for cervicogenic headache.
Characteristics of participating chiropractors.
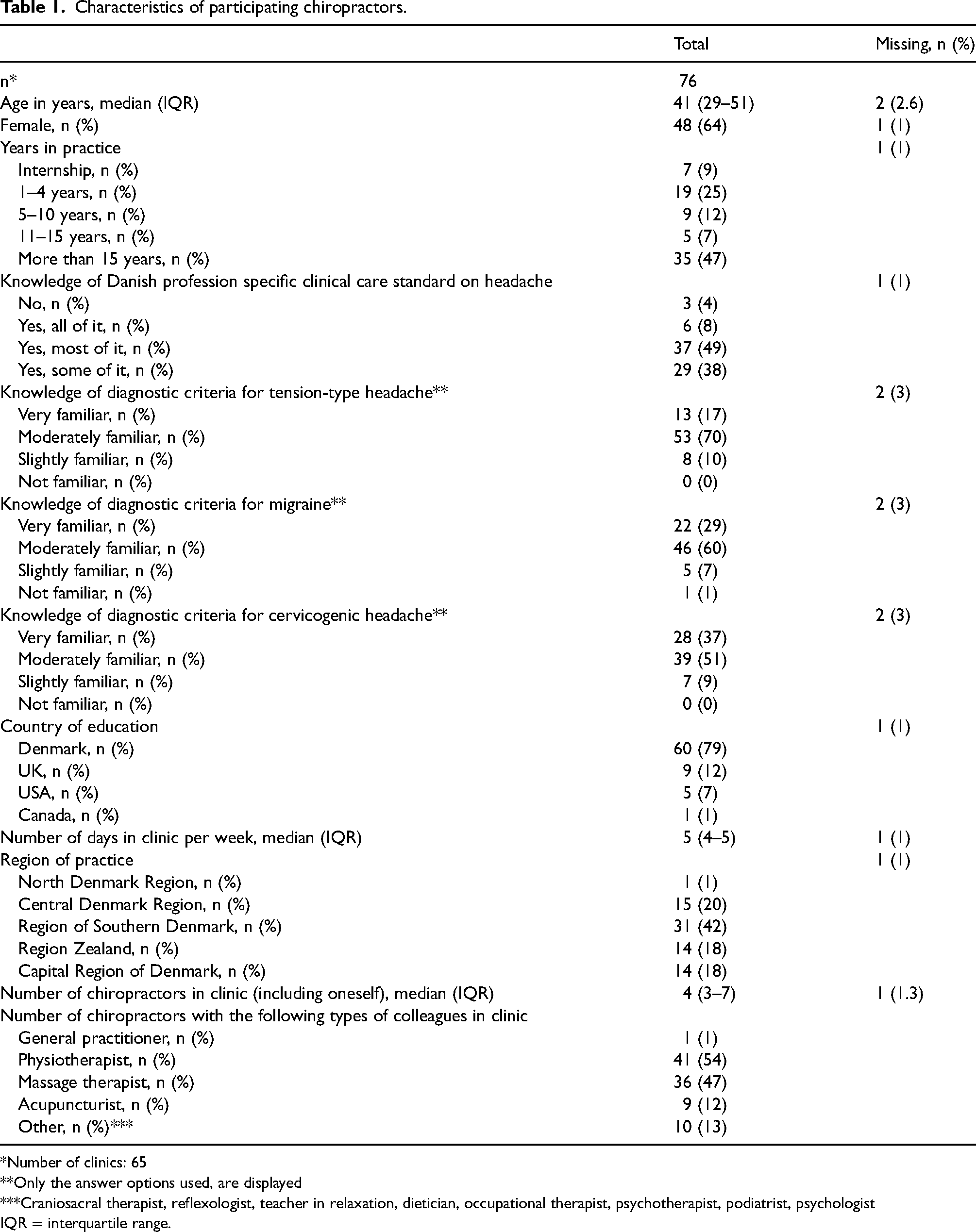
*Number of clinics: 65
**Only the answer options used, are displayed
***Craniosacral therapist, reflexologist, teacher in relaxation, dietician, occupational therapist, psychotherapist, podiatrist, psychologist
IQR = interquartile range.
During the 20-day period, there were 22,917 consultations covering all types of diagnoses. Of these, 2820 consultations were related to headaches. The mean prevalence of headache consultations was 12.6% (95% CI = 11.1–14.1) and varied from 0% to 38% between the participants (Figure 2). In 1244 (43%) of headache-related consultations, the headache was the primary complaint, rather than a secondary symptom associated with conditions such as neck pain.

Prevalence of headache consultations per chiropractor (n = 22,917).
Of the 22,917 consultations, headache was reported as the primary reason for seeking care in 1431 cases (6.2%) and as a secondary reason in 1794 cases (7.8%). The number of consultations with new patients regardless of diagnosis was 1973 (12.4%), with headache as the primary complaint in 101 (5.1%) and headache as a secondary complaint in 145 (7.3%) of new consultations.
The mean prevalence of the four different consultation types is shown in Figure 3, with 12.2% (95% CI = 10.1–14.2) of all new patients presenting with headache. Irrespective of diagnosis, most consultations were with “existing patients” (n = 16,122). One out of four “maintenance care” consultations (24.6%, 95% CI = 19.3–29.9) were related to headache. The number of “new patient” consultations with headache (12.4%) can be considered a proxy for the true prevalence of new headache patients, as these encounters are more likely to represent unique individuals. This is unlike “existing patients”, who may be registered several times during the 20-day period. The mean age of “new patients” was 38 years (95% CI = 36.4–39.9), ranging from 5 to 77 years.

Prevalence of consultation type for all diagnoses and headache diagnoses (n = 22,917).
Out of the 2820 consultations for headaches, 61% were categorized as “existing patients”, 18% were “maintenance care”, 11% were “new problems”, 9% were “new patients” and 0.7% were “not reported”.
The most prevalent type of headache registered was tension-type headache with 1795 (63.4%). Cervicogenic headache accounted for 1241 (44.0%), migraine accounted for 398 (14.1%) and “other” accounted for 493 (15.7%) (Figure 4). There was no diagnosis reported in 18 (0.6%) cases. The most frequent “other” type of headache reported was headache associated with concussion, with 221 (44.2%) cases. Excessive use of headache medication, psychological disorders such as stress and anxiety, and temporomandibular problems were some of the other causes.

Prevalence of headache types (n = 2820).
The chiropractors had the option to report more than one type of headache. Therefore, we introduced a new categorization, classifying headaches either as a single distinct type or as a combination of headaches (i.e. having more than one headache diagnosis). When assessing the prevalence of the single distinct diagnoses and the combined diagnoses, we observed a consistent pattern of prevalence compared to the overall pattern. Tension-type headache was the most common type of headache accounting for 1022 (36.2%) cases, whereas migraine was the least prevalent, with only 96 (3.4%) cases. In 971 (34.4%) cases, more than one type of headache was reported, and all types of headache combinations were noted (Table 2). The most common combination was tension-type and cervicogenic headache, with 350 (36.1%) cases.
Combination of headache types in consultations with more than one type of headache (n = 971).

*Other (e.g. concussion, excessive use of headache medication, psychological disorders, temporomandibular problems).
There were no associations between the prevalence of headache consultations and chiropractor characteristics (age, sex, knowledge of Danish profession-specific clinical care standard, knowledge of diagnostic criteria and experience) (Table 3).
Associations between the prevalence of headache consultations and chiropractor characteristics.

*Knowledge of diagnostic criteria dichotomized into very confident and less confident.
CI = confidence interval.
The mean age for new patients according to headache type was 37.3 (95% CI = 34.3–40.4) for tension-type headache, 38.0 (95% CI = 25.1–50.9) for migraine, 39.9 (95% CI = 35.8–44.0) for cervicogenic headache, 37.6 (95% CI = 34.8–40.4) for mixed headache and 40.6 (95% CI = 29.2–52.1) for other headaches. Age as a predictor of headache type was not statistically significant (p-values ranging from 0.33 to 0.95).
Discussion
Our results indicate that headache management is frequently encountered in chiropractic private practice, with approximately 12% of chiropractic consultations involving individuals with headache, of whom 43% cited headache as the primary reason for seeking care. Tension-type headache was the most common type of headache. A combination of headaches accounted for a large proportion of reported headaches, mainly tension-type and cervicogenic headaches, but all combinations occurred. Headache patients were likely to continue treatment after the initial course of treatment, as one in four maintenance care consultations were related to headache. None of the chiropractor characteristics were associated with the prevalence of headache consultations.
Moore et al. (22) conducted a study on the prevalence of headache patients in Australian chiropractic practice. The study found that one in five new patients presented with a chief complaint of headache. By contrast, the present study showed that, in Danish chiropractic practice, only one in ten consultations with new patients (255 out of 1973) were related to headache, and headache was the primary complaint in only one out of twenty new consultations (101 out of 1973). One reason for this difference could be the simple fact that Danish patients are less likely to seek chiropractic care for headaches than Australian patients. A more plausible reason could be due to differences in study design. The study by Moore et al. (22) was a two-week retrospective study, whereas our study was a 20-day prospective study, which some participants perceived as a lengthy duration for registration. This longer period may have contributed to fewer registrations due to fatigue among participating chiropractors. Another factor contributing to the discrepancy between studies may be the substantial variation in the prevalence of headache consultations reported by Danish chiropractors, which ranged from 0% to 38%. The reasons for this variation are not fully understood. Potential explanations include differences in clinic patient populations, fluctuations in patient volume during the observation period, individual chiropractors’ clinical focus or interest in managing headache cases and variation in how consistently the logbooks were completed.
Interestingly, our study recorded almost twice as many new patients regardless of diagnosis (adjusted to the same two-week prevalence) as did the study by Moore et al. (22) (mean 13 vs. 7). This could imply that the types of issues presented by the Danish population seeking chiropractic care may differ from those of the Australian population. In another 2013 cross-sectional Australian study of chiropractic encounters (34), only 3% of the diagnoses recorded were related to headache, which is much lower than both the study by Moore et al. (22) and the present study, suggesting some discrepancies in study design and a need for more detailed studies regarding headache management in chiropractic practice.
Although the prevalence of headache patients in our study was lower than in the study by Moore et al. (22), there is still a substantial number of headache patients seeking chiropractic care in Denmark. According to publicly available data from Statistics Denmark, approximately 360,600 unique patients were seen by a chiropractor in 2022. If 12% of these patient contacts were related to a case of headache, as our data suggests, this means that more than 43,000 people with headaches were seen by chiropractors. Nevertheless, there appears to be a lack of knowledge among primary care providers about the management of headache patients in chiropractic practice. In a recent study aiming to explore the management of headache patients in Danish general practice, Carlsen et al. (7), examined referral patterns of general practitioners to neurologists and imaging. They found that almost half of all headache patients were referred to a neurologist and 25% for a computed tomography or magnetic resonance imaging scan, despite recommendations that most should be managed in primary care. This underlines the need for educational activities as well as better communication and collaboration between different primary care providers. The study by Carlsen et al. (7), did not examine referrals to chiropractors, only to physiotherapists (29%), emphasizing the lack of knowledge about that referral pathway. To our knowledge, referrals to chiropractors in primary care have not been investigated. One possible explanation for this could be that chiropractors have not traditionally been involved in usual care of patients with headaches in primary care. However, as this has not been studied, it is unclear whether this is the case. Another possible explanation could be the concern among general practitioners regarding the current level of evidence supporting chiropractic management because there is a lack of high-quality trials in this area. Specifically, there is limited evidence supporting manual therapies for people with migraines, inconsistent evidence for people with tension-type headaches, and the strongest evidence for people with cervicogenic headaches (14,17,35). Chiropractic management is often associated with spinal manipulation; however, this represents only one of the several treatment modalities offered by chiropractors. Their management approach also includes mobilisation techniques, soft tissue treatment, exercise, patient education and guidance on self-management strategies, all of which are recommended by various guidelines as suggested non-pharmacological interventions (9,11) Despite these recommendations, general practitioners frequently express concerns about the safety of cervical spinal manipulation due to suggestions that it may be associated with strokes (36). However, current evidence does not indicate an increased risk of stroke following a visit to a chiropractor, and the reported associations between visits and stroke appear to be similar for both chiropractors and general practitioners (37,38). Large-scale, methodologically rigorous randomized controlled trials (RCTs) are needed to better evaluate the efficacy of chiropractic management, including manual treatment, for headaches.
In the present study, headache responses were classified as tension-type, migraine, cervicogenic headache and “others” with the possibility for the chiropractor to add a diagnosis in a text box. In the study by Carlsen et al. (7), 161 out of 367 (44%) patients with headache were diagnosed with migraine. This high number is probably because migraine is most commonly treated with medication, which needs to be managed by a general practitioner. Pharmaceutical approaches are well-supported by high-quality RCTs and systematic reviews and are part of mainstream clinical guidelines for management of migraine (8,39). Chiropractic-based management shows some promise, but there is a lack of high-quality RCTs and the evidence is inconsistent, limited and often methodologically weak (35,40). Another reason for the higher prevalence of migraine in general practice may be the diagnostic challenges of headache because a mild migraine may resemble a tension-type headache or a cervicogenic headache in terms of moderate intensity, and accompanying neck pain and/or mild nausea, and the diagnostic process can be complicated when a patient has both migraine and tension-type or cervicogenic headache (41–43).
It is important to note that some studies reporting headache prevalence do not include cervicogenic headache as a separate diagnosis (1,7) and there has been some debate about this relatively common diagnosis, the underlying mechanisms and the clinical utility of the diagnostic criteria (44,45), and the diagnosis has been in and out of the ICHD-3 classification (46). Our study included cervicogenic headache to provide a more comprehensive understanding of types of headaches seen in primary care. The chiropractors also had the option of reporting more than one diagnosis, accounting for 34.4% of the consultations. A study by Moore et al. (47) had an almost similar finding of 33%, but this was based on patient self-report. In addition, their group of patients had a higher level of disability measured by the HIT-6 test (48), compared to patients with only one diagnosis. Carlsen et al. (7) also found that having more than one headache diagnosis was associated with a higher number of referrals to a neurologist and a study by Lyngberg et al. (49) found that those with more than one headache diagnosis were more likely to be absent from work. It is therefore important to be aware of patients with multiple headache diagnoses because their management is likely more complicated, requiring individualized assessment and management strategies, which could include both pharmacological and non-pharmacological treatment. The literature is ambiguous on the nomenclature for experiencing more than one type of headache, and terminology such as multiple headache diagnoses, combination headache and co-existing or mixed headache have been used, but this has also been debated (47,49–51). The most commonly reported combination of headaches in the literature is migraine and tension-type headache; other headaches are rarely included and the challenges of distinguishing migraine from tension-type headache have been discussed (41,42).
Our results showed that one in four “maintenance care” consultations (24.6%, 95% CI = 19.3–29.9) were related to headache. Maintenance care is defined as a treatment approach in which patients receive care at regular intervals over a period. The primary goal is to prevent future episodes of the condition being treated (secondary prevention) aiming to minimize the impact of the condition over time. We do not yet know the effect of regular treatment on headache. Research concerning other pain conditions, such as low back pain, has shown that, in a selected group of patients with recurrent or persistent pain, the clinical course becomes more stable, and the number of pain-free weeks increases (52). Although the underlying mechanisms of low back pain differ from those of primary headache, these findings suggest that future investigation into similar approaches for recurrent headaches could be valuable.
Strengths and limitations
Only 10,9% of the invited chiropractors participated in the data collection. It should be noted, however, that the invitation was sent by email to all chiropractors in Denmark, including those who did not work in private practice, making it irrelevant for some because it was not possible to differentiate them from others in the email list. In comparison, Moore et al. (22) achieved a response rate of 36%, with the chiropractors representing 12% of the total chiropractic population in Australia. The participation rate in the present study seems reasonable given that participants committed to 20 days of data collection. However, the participant distribution across region, gender and age is somewhat different to the demographic profile of Danish chiropractors (53), thereby diminishing the representativeness of the sample. In the present study, the participants were generally younger and there were more females and participants from the Region of Southern Denmark than in the demographic profile of Danish chiropractors. The high proportion of female clinicians participating (64%) may be partially influenced by the higher prevalence of headaches among women in the general population. This could suggest that female clinicians are potentially more aware of, or more attentive to, headache-related symptoms in their patients.
However, it is also important to consider the possibility that those who chose to participate may have a special interest in research, and headache in particular, and therefore see more patients with headache than those who did not participate in the data collection. This may have potentially introduced selection bias that could have resulted in an inaccurately high prevalence of headache in our study.
We consider it a strength that the online survey provided a comprehensive description of the ICHD-3 classification criteria for primary and secondary headaches before asking chiropractors if they were familiar with the diagnostic criteria for the headaches listed. We therefore rely on the chiropractors to be informed of the ICHD-3 criteria before completing the 20-day data collection, including diagnosis of their patients, which would improve the quality of the data collected.
Patient characteristics were limited to age, which prevents any comparison with the existing literature. This approach was chosen to minimize the burden on chiropractors and to maintain patient anonymity. However, future research is needed to explore patient characteristics in a more robust way, including patient-level data collection. It is important to note that the present study only collected data from chiropractors and did not allow for follow-up.
We did not include more specific subtypes (e.g. episodic or chronic tension-type headaches, migraine with or without aura, or medication-overuse headache) in the survey. Although doing so could have provided a more detailed understanding of types of headaches seen in chiropractic care, we were concerned that a longer and more complex logbook registration might reduce completion rates among participants.
Perspectives
The present study is novel in its field because it uses the prospective nature of individual chiropractor encounter data. The results of this study may increase awareness among clinicians, stakeholders and researchers of the relatively high prevalence of headache patients seeking care in chiropractic practice. In addition, providing information on the distribution of diagnostic groups may help to better understand the healthcare needs of headache patients seeking care. To optimize the management of chiropractic patients with headache, it is necessary to determine the characteristics of these patients, their clinical course in chiropractic practice, and how other health conditions influence prognosis and treatment effects. It is also important to gain a better understanding of who is seeking chiropractic care for headache, why they are seeking it and their care pathways through the healthcare system. To gain more insight into this, we have initiated a cohort study in Danish chiropractic practices, in which we follow patients with headaches for one year. The study is ongoing and is expected to conclude in 2026. Establishing structured interdisciplinary collaboration with other healthcare providers could potentially improve the care of patients with headaches and help reduce the number of patients referred to secondary or tertiary care. The present study contributes to the broader field of health services utilization, which is essential for informing decisions related to health policy development, system efficiency and the equitable allocation of resources. By examining how chiropractic care is accessed and utilized for headache-related concerns, our findings provide insights into the role that chiropractors play in a primary care setting. Understanding these patterns can support future decision-making around service delivery and workforce integration in multidisciplinary care models.
Conclusions
Headaches are common in chiropractic patients, with a predominance of tension-type and having more than one type of headache. Headache was the primary reason for consulting the chiropractor in two out of five headache consultations and headache patients are likely to continue treatment after optimum benefit is reached with one in four maintenance care consultations relating specifically to headache management. No specific chiropractor characteristics were associated with the prevalence of headache consultations. Clinicians, stakeholders and researchers should take note of these results because they underscore the importance of understanding the health care needs of headache patients in chiropractic practice.
Clinical implications
Headache management is frequently encountered in chiropractic practice in Denmark, with a predominance of tension-type and having more than one type of headache.
It is necessary to determine the characteristics of patients with headache seen in chiropractic practice and their clinical course to optimize the management of patients with headache in primary care.
Chiropractic care may contribute to a multidisciplinary management in primary care, potentially reducing costly and unnecessary examinations and referrals to specialists in secondary care.
Footnotes
Acknowledgements
We thank the participating chiropractors who gave their time to collect data for this project. In addition, we thank Suzanne Capell for proofreading the manuscript. We acknowledge OPEN, Open Patient data Explorative Network, Odense University Hospital, Region of Southern Denmark, for access to the REDCap electronic data capture tool and technical support.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KBD, HWC, MMS and RKJ are supported partly or fully by the Foundation for Chiropractic Research and Postgraduate Education. KBD and MMS are in private practice treating headache patients but did not participate in the online survey or the logbook registration. There were no other potential conflicts of interests with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Foundation for Chiropractic Research and Postgraduate Education funded the study.
Author contributions
All authors contributed to the concept and design. KBD performed the analysis and outlined the draft manuscript. All authors took part in interpreting the results, drafting the manuscript, and critically reviewing and revising the manuscript. All authors read and approved the final version of the manuscript submitted for publication.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.