
Abstract
The prevalence of cervicogenic headache (CEH) is only vaguely known. Furthermore, it is a common belief that in migraine without aura (MwoA), neck symptoms frequently occur and that MwoA and CEH may pathogenetically be intimately related. In the Vågå study, 1838 18-65-year-old citizens (88.6± of that age group) were studied with face-to-face interviews and a thorough neck examination. For CEH, the Cervicogenic Headache International Study Group criteria were used, and for MwoA, the IHS criteria. The extent of cervical involvement was assessed by the ‘CF’ (‘features indicative of cervical abnormality’). CEH prevalence was 4.1±. ‘CF’ was 2.37 in CEH vs 0.93 in M-A. CEH criteria, e.g. mechanical attack provocation, were present many times more frequently in CEH than in MwoA. Conversely, migraine criteria, e.g. photophobia, were ≥ 2.6 times higher in MwoA than in CEH. CEH is unlikely to be a subgroup of MwoA.
Introduction
Cervicogenic headache (CEH) seems to be fairly common in hospital headache practice (1). However, prevalence among unselected population groups and based upon modern diagnostic criteria is less well known. One aim of the Vågå study was to study CEH prevalence.
There are diverging ideas as to the nosologic status of CEH. Some researchers still seem to believe that CEH is only a migraine variant, that neck symptoms and signs are as frequent in migraine-aura (MwoA) as in CEH, and even that CEH profitably can be treated with migraine drugs. Thorough questioning and systematic physical/neurological examination of the neck, head and face were routinely carried out during the Vågå study, and solitary features pertinent to the neck could be roughly quantified in every participant. With this basis, a comparison of nuchal features in the two headaches could be carried out.
Materials and methods
The number of inhabitants in Vågå, Norway, was 3907. All 18–65-year-old inhabitants were invited to participate, and 1838 (88.6% of the actual individuals) were finally included (2). The F/M ratio was 1.06.
For the diagnosis of CEH, the Cervicogenic Headache International Study Group (CHISG) criteria were used (3). The criteria are: (I) unilaterality of pain; (II) restriction, range of motion (ROM) in the neck; (III) pain provocation with awkward neck positions; (IV) pain provocation with pressure along occipital tendon insertions; (V) ipsilateral shoulder discomfort; and (VI) ipsilateral arm discomfort. The total score, with all criteria present, will accordingly be 6.0 (Table 1). Anaesthetic blockades were not an obligatory part of the first version of the criteria, in vogue at the time (3). Moreover, no blockades were carried out in the Vågå study.
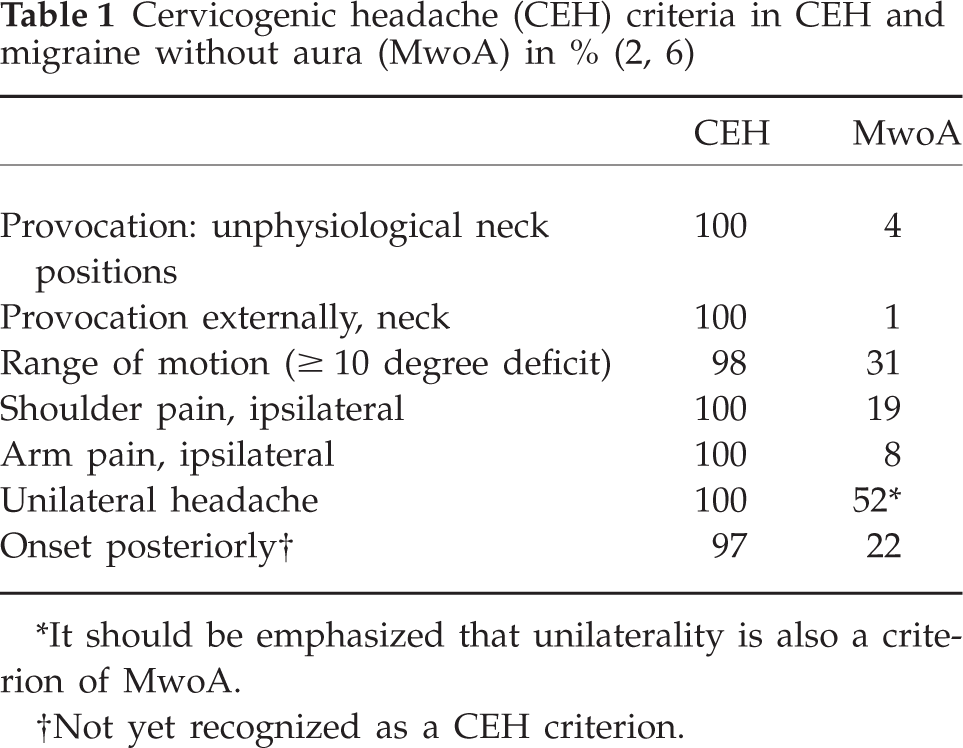
It should be emphasized that unilaterality is also a criterion of MwoA.
Not yet recognized as a CEH criterion.
The more criteria are present the more secure the diagnosis is. It was felt that as blockades were lacking, at least four of the ordinary criteria (Table 1) should be present. A ≥ 10° reduction in the capability to rotate in the neck has been taken as a token of positivity of the test. Pain provocations are an essential part of the criteria. The external force applied (criterion IV) was 3–4 kg, as recommended by the International Association for the Study of Pain (4) for diagnostic work in fibromyalgia. A force of this magnitude creates a feeling of discomfort/pain locally in most individuals. The force applied locally must be of such a magnitude that it can distinguish between presence and absence of a forward spreading of the unpleasant, local sensation. Pain sensation thresholds are not of any interest in this context. All cases fulfilling the given criteria would be characterized as proper cases of CEH.
However, for the purification of the symptomatology as such, cases of apparent coexistence of CEH with tension-type headache (TTH) and MwoA were taken out: it was realized that it would be hard, both for investigator and participant, to sort out which symptoms belonged to CEH proper in the presence of these other headaches. The diagnoses of MwoA and TTH were established according to the IHS criteria, first version (5), the one in vogue at the time. To assess the extent of cervical involvement, ‘CF’, i.e. ‘features indicative of cervical abnormality’, was calculated. CF is based on five solitary factors, i.e. ROM, skin-roll test and pressure towards various occipital/nuchal structures to elicit pain. The solitary factors are added for each individual, the maximum score being 5.0+ (2). The intensity of the pain was graded according to a 0–6 scale, the scores 3–5 corresponding to the IHS grades ‘mild’ to ‘severe’. Headache diagnoses were validated in a blinded fashion, with recheck of 100 records, and of 41 individuals (2, 6).
Results
There were 75 cases fulfilling the CEH criteria. The prevalence thus was 4.1%. The mean number of criteria in these individuals was 5.3 (range 4–6). There were 41 ‘core’ cases (i.e. without coexisting MwoA/TTH). The mean number of CEH criteria in these 41 core cases was 6.0, or close to that. There was a F/M sex ratio of 0.71, as against 1.06 in the entire Vågå series. Thus, CEH does not seem to be mainly a female disorder, as previously suspected; attacks could also be precipitated mechanically.
The mean age of onset was 32.7 years (2), which indicates that CEH is not a disorder first and foremost among the elderly. The mean intensity was 3.8 (2) vs 4.2 in MwoA (6). Posterior onset of attacks was widely more frequent in CEH (97%) than in MwoA (22%) (Table 1). Unilaterality (obligatory), ipsilateral shoulder/arm pain were invariably present in CEH. The CEH picture in the core cases was therefore a stereotyped one. In MwoA, CEH criteria were at quite another level (Table 1). Except for unilaterality, which is a criterion for both headaches, the differences amounted to a factor of 3 or more (6). The CF was 0.93 in MwoA and 2.37 in CEH. Migraine criteria showed an entirely opposite pattern (Table 2). Mean values for migraine parameters for the two headaches differed by a factor of ≥ 2.6. CEH thus seems to differ entirely from MwoA, both with regard to typical CEH traits and typical MwoA traits.

In this scale, 3 corresponds to the IHS level ‘mild’, 4 to ‘moderate’, and 5 to ‘severe’.
Discussion
The present study on CEH prevalence is as far as we know the first large one with CHISG criteria, with face-to-face technique and one sole investigator. Two previous studies showed a prevalence of 4.6% (modified CHISG criteria) and 17.8% (modified IHS criteria), respectively. The prevalence of 4.1% indicates that in Vågå CEH may be one of the three major headaches, quantitatively speaking, the other ones being MwoA with 31% and TTH with 34% (6, 7). The newly described syndrome ‘persistent neck complaint with subsequent, transient, posterior headache’ with a prevalence of 6.6% in Vågå (7) may be a challenge to the third position among the headaches. There are six workable diagnostic criteria. The anaesthetic blockades actually belong to a separate category in this respect. In several recent studies, blockades have not been made. The reasons for this may be: (i) a set-up for blockades may altogether be lacking in that particular setting; (ii) the pain level may not be high enough during the actual consultation for meaningful blockades to be carried out; and (iii) an important question is where to deposit the anaesthetic agent.
As CEH probably is a syndrome, several locations could serve as noxious foci. As of today, one must put up with the likelihood that many blockades are not done in an optimal location. Many workers in the field have realized this. Moreover, the crucial site may be out of reach with a needle (8). In recent years, the idea of noxious foci in the upper cervical area, e.g. along the major occipital nerve, may have gained too much attention. In 60 CEH cases operated upon with the Robinson-Smith stabilization technique, affection of the discs C 5–6 and C 6–7 made up 77% of the total series, only c. 6% concerning C 3–4 and above. On only one occasion, did the disc C 2–3 seem to be affected (9). The insight into the putative pain-producing loci in CEH leaves much to be desired. For these reasons, our attitude towards obligatory blockades at present is one of wait-and-see. When more information is available, routine blockades may be of invaluable benefit.
While the status of obligatory blockades may be somewhat dubious, posterior onset of pain per se may emerge as a strong, new CEH criterion (Table 1). With seven criteria available, one actually will have a formidable instrument for diagnosing CEH clinically. It has been claimed that there are many similarities between CEH and MwoA with regard to clinical picture, neck involvement, and therapy. CEH could be only a migraine variant. Frese et al. (10) have recently demonstrated that CGRP blood level in CEH attacks differs from that of MwoA attacks. If a CEH attack only served as a provocative factor for a MwoA attack, then the MwoA neuropeptide pattern should be present also during the CEH attack; but it was not. This is a strong argument in favour of a separate position for CEH as a headache. Also, the clear difference between CEH and MwoA in the response to pregnancy points strongly in favour of a dichotomy.
As demonstrated in recent works (2, 6) and detailed in Tables 1 and 2, the differences between CEH and MwoA are so marked that it seems highly unlikely that CEH can be only a MwoA variant, or just a provocative factor, and MwoA does not seem to be a CEH variant. We seem to be faced with two entirely different headache disorders.
Conflicts of interest
The author has declared no conflicts of interest.