
Abstract
Cervicogenic headache (CEH) is a neck-generated headache syndrome. Attacks may be similar to migraine (M) or tension-type headache (TTH). In order to test the accuracy of the IHS diagnostic criteria for M and episodic TTH and of the criteria for CEH of Sjaastad et al., 33 CEH, 65 M, and 29 TTH were evaluated according to the CEH criteria, and CEH patients were tested for M and TTH according to the IHS criteria. Only 30% of the CEH patients met the criteria for M, 3% met the criteria for TTH, and 66% were neither M nor TTH. The mean number of criteria met, sex, age, and age of onset were also analysed, and the results indicate an inequality among these three headache types. The most important differentiating aspects were the site and radiation of the pain, the temporal pattern, and the induction of attacks from neck posture, movements, and/or digital pressure. CEH clearly differs from M and TTH. Existing criteria adequately distinguish the three headaches.
Although it is generally accepted that some headaches may originate in the neck—existing data seem to support the concept of neck-generated headaches (1 –7)—cervicogenic headache (CEH) has been controversial (8 –11). The lack of objective diagnostic markers and the diversity of the reported clinical materials contribute to this uncertainty.
Various authors have identified CEH. Previous descriptions of the “céphalée cervicale” (6, 12, 13) are similar to the picture described by Sjaastad, who believes CEH is a well-defined reaction pattern (14, 15). The pain typically starts in the occipitalnuchal area and spreads to the ipsilateral forehead, where it becomes intense, and if the pain is predominantly unilateral, it is always on the same side. Attacks may be provoked by neck movements and/or digital pressure over trigger points, such as the greater occipital nerve (GON) or the C2 area. A diffuse, ipsilateral arm pain or discomfort may also occur. Females are more affected than males, and a trauma may precede the onset of the syndrome, although many patients have no neck or head injury.
Various cervical lesions may be involved in CEH. Kerr observed that stimulation of different rootlets (C1 and C2) in patients operated under local anesthesia evoked pain in frontal areas (16). Permanent or intermittent hemicranial headache attacks have been related to upper cervical root compression (17), and decompression of C2 has been described as successful in CEH (17, 18). In the so-called “third occipital headache”, the pain may be abated by anesthesia on the third cervical root (19). One patient with a C6-C7 disk herniation had a long history of unilateral headaches that vanished after decompression of the C7 root (20).
Migraine (M) may be similar to CEH (2, 11). Both are paroxysmal and unilateral headaches, affecting mainly females, which may be accompanied by nausea, vomiting, phono- and/or photophobia. On the other hand, cases with moderate pain of pressing quality without other M traits can be similar to tension-type headache (TTH).
If CEH is a distinct entity and if existing diagnostic criteria are adequate, it should be possible to separate this disorder from the other two headaches on this basis. However, if CEH is not a separate disorder, many CEH patients would be expected to meet the criteria for the most frequent primary headaches.
The objective of this work was to compare cervicogenic headache (14) with M (21) and TTH (21) on the basis of the classification criteria.
Materials and methods
Thirty-three cervicogenic headache patients, diagnosed according to the criteria of Sjaastad et al. (14), and 29 episodic TTH and 65 M without aura patients, diagnosed according to the IHS criteria (21) examined in our outpatients unit (1993–1995) were selected for this study. TTH sufferers with intermittent M attacks and migraineurs with frequent interictal TTH were not included. All CEH patients had strictly unilateral headache attacks without side shift. The inclusion criteria used in this study are summarized in Tables 1 and 2.
Diagnostic criteria for cervicogenic headache according to Sjaastad et al. (14).

Diagnostic criteria for migraine and tension-type headache according to the IHS (21).

CEH patients were tested for M and TTH according to the IHS criteria (21), and M and TTH patients were tested for CEH according to the CEH diagnostic criteria. Blockades of the greater occipital nerve (22) were performed in 25 CEH patients with 1–2 ml 0.5% bupivacaine, and were considered effective if anesthesia over the GON distribution (tested with a needle) was obtained. The blockade was considered ineffective if the pain in the forehead was not totally or was only partially abated. M and TTH patients were not blocked. The cervical range of movement was considered abnormal if the subject was unable to rotate the head up to 90°, making the chin in line with the shoulder; was unable to extend the head until the forehead was horizontal; or was unable to flex the head until the chin was close to the chest (CEH criterion IIC). The chi-square test or the Fisher test was used to compare the diagnostic criteria. Analysis of variance (ANOVA) was used for comparing the total number of criteria for CEH, age, and age of onset (data shown as mean ± standard deviation (SD)) among the three groups. The number of criteria for TTH and M were compared using the Mann-Whitney U test. The criteria differentiating best among the three headache types were selected using logistic regression analysis. Differences with p < 0.05 were considered significant.
Results
The female sex was predominant in all headaches (CEH: 87.8%; M: 73.8%; TTH: 82.7%), and the differences were not statistically significant. CEH patients were comparatively older than M patients (CEH: 45.21 ± 13.67 years; M: 34.35 ± 13.44 years; p = 0.003, ANOVA), but not significantly older than TTH patients (38.2 + 17.5 years). Concerning the age of onset, M started earlier than the other two headaches (CEH: 35.06 ± 17.53 years; M: 18.4 ± 10.3 years; TTH: 29.0 ± 13.8 years; p = 0.0001).
Criteria for CEH according to Sjaastad et al. (14)
Fig. 1 shows the percentage of CEH, M and TTH patients meeting the diagnostic criteria for CEH. All CEH criteria except two (criteria III and XIV) differed clearly between CEH patients and M patients (p < 0.05). As shown in Fig. 1, few M patients met the major criteria of Sjaastad et al. (14) for CEH. Only 4 (6.15%) had unilateral headache without side shift (criterion I). None of the M patients met any of the CEH criteria in group II (symptoms and signs of neck involvement). According to logistic regression analysis, the best differentiating criteria were IV (pain with varying duration or fluctuating continuous pain), and IIa1 (similar pain triggered by neck movement and/or sustained awkward head positioning). CEH patients met 10.51 (±2.14) criteria out of the 18 tested criteria, whereas M patients met very few (3.85 ± 0.94; p = 0.0001, ANOVA). To differentiate M and CEH patients with 100% sensitivity and specificity would require at least seven of the CEH criteria listed in Table 1.
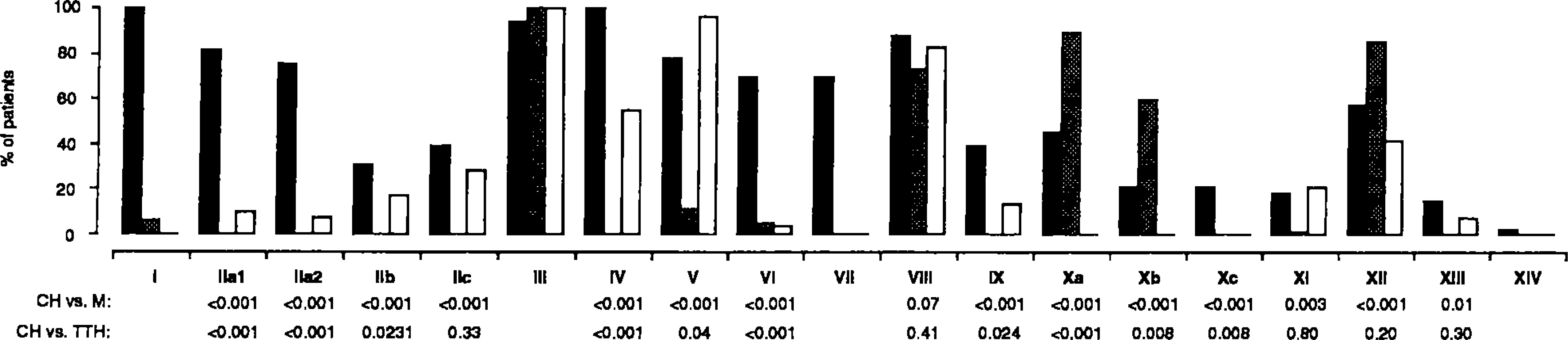
Percentage of cervicogenic (black bars), migraine (gray bars), and tension-type headache (white bars) patients fulfilling the diagnostic criteria for cervicogenic headache according to Sjaastad et al. (14). p-values comparing cervicogenic headache with the other two headaches are shown where applicable or feasible.
All CEH criteria except two (criteria IIc and VIII) differed clearly between CEH patients and TTH patients (p < 0.05). No TTH patient met major criterion I of Sjaastad et al. (14) (unilaterality without side shift). Three (10.34%) met criterion IIa1 (similar pain triggered by neck movement and/ or sustained awkward position); 2 (6.9%) met criterion IIa2 (pain triggered by pressure over the ipsilateral upper, posterior neck region or occipital region); 5 (17.24%) met criterion IIb (ipsilateral nonradicular neck, shoulder and arm pain); and 8 (27.59%) met criterion IIc (reduced range of motion of the cervical spine). In a logistic regression model the best differentiating criteria were I (unilaterality without side shift), VI (pain starting in the neck, eventually spreading to frontal areas), and IIa1 (similar pain triggered by neck movement and/or sustained awkward position). Of the 19 CEH criteria, TTH patients met 4.89 ± 1.57 (CEH patients: 10.51±2.14; p = 0.0001). The number of CEH criteria met did not differ (ANOVA) between M and TTH patients (4.89 ± 1.57). Thus, we may conclude that seven or more criteria for CEH may distinguish CEH and TTH patients with 100% sensitivity and 86.2% specificity.
Criteria for M without aura according to the IHS
Fig. 2 (upper panel) shows the percentage of CEH and M patients meeting the IHS criteria for M. All values were statistically different (p ± 0.001). Except for C1 (unilateral location), there were more M patients than CEH patients as regards all criteria. M patients met comparatively more criteria than CEH patients (6.88 ± 0.87 and 3.82 ± 1.61, respectively, p = 0.0001). No CEH patient met all 8 criteria for M (max: 7). Eleven (33.3%) of 33 CEH patients met the IHS criteria for M. Only one of the 22 CEH patients not meeting the criteria for M was a TTH sufferer according to the IHS criteria. With logistic regression models, the best differentiating criteria were A (at least 5 attacks meeting criteria B-D), C3 (moderate or severe pain), and C1 (unilaterality). Thus, we may conclude that five or more criteria would differentiate M and CEH with 100% sensitivity and 63.6% specificity.
Criteria for episodic TTH according to the IHS
Fig. 2 (lower panel) shows the percentage of CEH and TTH patients meeting the IHS criteria for TTH. The statistically different items were A, B, C2, C3, D1, and D2 (p ± 0.002). Except for C2 (mild or moderate intensity), there were more TTH patients than CEH patients as regards each criterion. TTH patients met considerably more criteria than CEH patients (6.93 ± 0.79 and 3.85 ± 1.42, respectively; p = 0.0001). No CEH patient met all 8 criteria for TTH (max: 6). Only 1 (3%) CEH patient met the IHS criteria for TTH. Only 11 of the 32 CEH patients that did not meet the criteria for TTH would have met the criteria for M. Thus, 22 (66.6%) of the CEH patients could not be diagnosed as suffering from the other two headache types. The best differentiating criteria were A (at least 10 previous headache episodes meeting criteria B-D), C3 (bilateral location), and B (headache lasting 30 min-7 days, logistic regression analysis). Thus, we may conclude that to differentiate TTH and CEH with 100% sensitivity and 81.8% specificity, 6 or more TTH criteria are required.
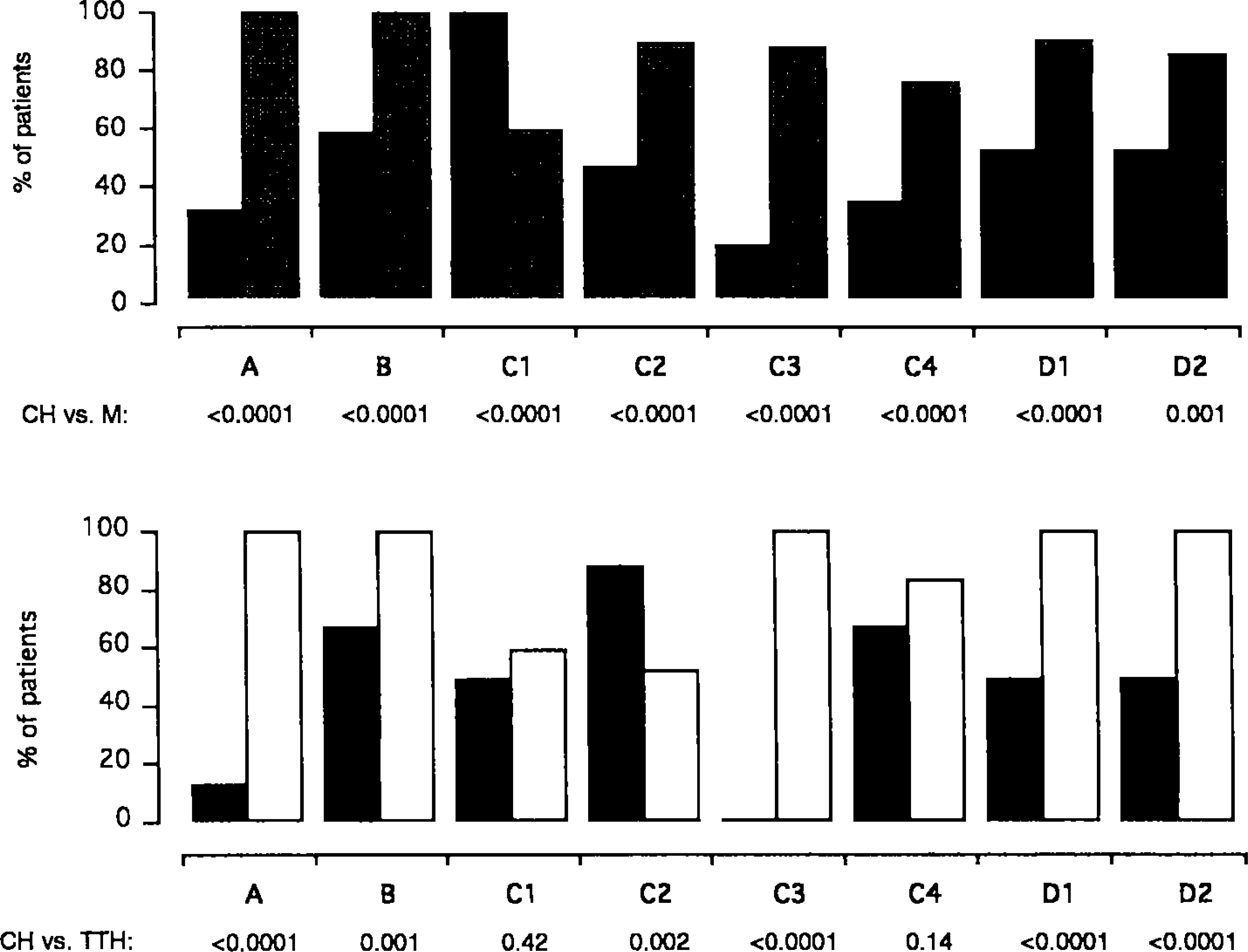
Upper panel: Percentage of cervicogenic (black bars) and migraine (gray bars) patients fulfilling the diagnostic criteria for migraine according to the IHS (21). Lower panel: Percentage of cervicogenic (black bars) and episodic tension-type headache (white bars) patients fulfilling the diagnostic criteria for episodic tension-type headache according to the IHS (21). Criteria for both headaches are listed in Table 2. p-values comparing the criteria individually are shown.
Discussion
To classify headaches is a difficult task, partially due to the lack of objective diagnostic markers. “Splitters and lumpers” still discuss whether M with aura and M without aura are a single entity (23 –25), the same occurring with M and TTH (26, 27). The previously used headache classification criteria considered cluster headache and M parts of the same “vascular headache” group (28), but now they are classified separately (21).
Sjaastad et al. popularized the term “cervicogenic headache” (9, 15, 29), described the condition in detail, and proposed diagnostic criteria for this condition (14). According to this group, CEH is a unilateral headache affecting mainly females with signs and/or symptoms of neck involvement, such as attacks provoked by cervical movements or awkward positions. Since this syndrome may have traits in common with other primary headaches, especially M, the differential diagnosis may be intricate. The interesting question of whether CEH is actually M stemming from the neck also deserves consideration. Although it is easy to state that headaches may be neck-generated, to classify and differentiate CEH from other disorders is not simple. In the present study, CEH was first compared with M on the basis of the current diagnostic criteria.
The main characteristics of M according to the IHS classification are unilaterality, pulsating quality, intensity, nausea, vomiting, photo- and phonophobia. As for the site of pain, in our material only 6.1% of M patients had strict unilateral headaches without side shift, and 58.4% reported unilateral headaches with side shift. In contrast, strict unilaterality was an inclusion criterion for CEH. This is accordance with the findings in the study of 32 M patients of Sjaastad et al., in which only a minority (16%) presented with unilaterality without side shift (30). D'Amico et al. identified 20.8% side-locked unilaterality in M and 12.5% in TTH (31). Among 31 “classic migraine” patients, only 1 had side-locked unilaterality (32). Nick and Ziegler suggest that headaches stemming from the neck are usually unilateral and triggered by a certain head position, but they do not clearly state that they are side-locked or that stress pain must be located in the occipital area (5, 10). Martin and Aubert (according to (33)) wrote in 1951 about periocular pain induced by pressure on the first and second cervical roots, but laterality is not mentioned. According to Maigne, fronto-orbital pain may spread to the contralateral side if very intense, but otherwise is side-locked (6, 12). On the other hand, Bärtschi-Rochaix wrote that cervically generated headaches tend to be unilateral in cases of mainly traumatic etiology, but bilateral or alternating with arteriosclerosis or degenerative changes (4). However, based on the high frequency of both alternating head pain and cervical degenerative disorders, this statement may be regarded as speculative. Unilaterality without considering the side change seems to be insufficient for differentiating M and CEH (2, 34).
According to the present material, nausea (45.5% in CEH, 89.2% in M), vomiting, (21.2% in CEH, 60% in M), and photo- and phonophobia (57.6% in CEH, 86.2% in M) may also be present in CEH to a certain extent. In Pikus and Phillips' series of 35 CEH cases, nausea/vomiting was seen in 7 (20%) and even fewer had photophobia (5.7%) (18). In Sjaastad's series, nausea/vomiting occurred in 70–85% of the M patients and in 55% of the CEH group (2). Maigne considered that there is a migrainous form of CEH, but in this case the pain is nonalternating (6). In the present material, no CEH patient had aura-like phenomena. However, Bärtschi-Rochaix considered that visual symptoms are common in headaches of cervical origin, including colored or black and white scotomata, zigzag lines or fortification spectra (4). We believe that until clear evidence favoring this possibility is found, such visual abnormality should be considered indicative of M. In general, migrainous traits are far less common in CEH than in migraine itself.
If CEH were a subgroup of M, most CEH patients would meet the IHS criteria for M. This is not the case. As only 30% of CEH patients would be considered migraineurs according to the present criteria, the possibility of CEH being a subgroup of M is unlikely. Sjaastad et al.'s figures are also similar, as only 20% of their CEH patients meet the criteria for M (30). Even considering that some M patients could be coded 1.7 (migrainous disorder not fulfilling the above criteria), the difference between M and CEH still remains evident. It is also noteworthy that M patients are younger and have the onset of pain earlier in life. In all three headache types the female sex was predominant. However, this criterion is not adequate for differential diagnostic screening.
Sometimes CEH may present as a mild, nonthrobbing, episodic pain. We decided therefore to check how many CEH patients would be coded as episodic TTH according to the HIS criteria, and vice versa. In fact, with regard to two important IHS criteria (pressing quality and no aggravation by physical routine activity), there were no differences between TTH and CEH. Using the IHS criteria, only one CEH patient would be considered as suffering from episodic TTH. This indicates that although CEH and TTH may be similar to a certain extent, the present criteria for TTH seem to distinguish these two headaches appropriately. The criteria for chronic TTH are fairly similar to the list of items for episodic TTH, and were met by 4 CEH patients (12.1%, data not shown). These patients could not be classified as episodic TTH, mostly due to the first criterion (headache frequency ≥ 15 days/month). The present data suggest that CEH is closer to M than to TTH as far as the clinical picture is concerned.
Item 11 of the IHS classification groups the headaches associated with cranial structures, including the neck. CEH not meeting criteria 11.2 and 11.3 are not sufficiently validated, according to the IHS (21). Despite the fact that radiological abnormalities are required by the IHS, in our material most patients with CEH had no particular changes upon x-ray examination or MRI (data not shown), which is in accordance with previous studies (3, 35). Maigne had already mentioned that characteristic radiological abnormalities should not be expected in CEH (12). Changes in neck muscle contour, texture, tone, or response to active and passive stretching and contraction (item C2) are not frequent in our estimation, and should not be part of the criteria for CEH. However, a link between CEH and myofascial pain has been suggested (36). The IHS says that the pain is located in the neck and occipital region, and may project to the forehead, orbital region, temples, vertex, or ears. We suggest that the radiation to the forehead should rather be considered as typical of CEH. This radiation was present in 69.7% of the CEH patients, in contrast to 4.6% in M and 3.4% in TTH. Other authors (6, 14) have stressed this pattern of radiation.
Trauma, mostly of the whiplash type, has been considered important in CEH pathophysiology (29). In Pikus and Phillips' series (18), 80% of the patients had experienced trauma. Four out of five cases with probable cervicogenic headache had experienced trauma, according to D'Amico et al. (31). Maigne considered that trauma is “frequent”, but may have occurred far before pain onset and may be mild (12). In the present series, 8 (24.2%) of the CEH patients referred a previous trauma related to the onset of the disease. It may be difficult to assess the importance of trauma, as patients may forget or may not relate trauma to the onset of the pain. Despite reports on whiplash-related headaches (37), such injury may have less influence in head or neck pain than hitherto suspected (38, 39). Post-traumatic headache may not be a distinct disorder, as most patients meet the criteria for M and/or TTH (40). This suggests that trauma could instead be just a trigger phenomenon and not a separate cause of headache in itself. It is possible that trauma plays a role in the pathogenesis of some CEH cases.
The present data reveal that CEH seems to manifest itself differently from TTH and M, and that existing criteria seem to be adequate for distinguishing them. The site and radiation of the pain, temporal pattern and induction of attacks from neck posture, movements, and/or digital pressure are the most important differentiating aspects. Further research may help in classifying these three disorders more precisely. The IHS criteria for CEH need improvement.
Footnotes
Acknowledgements.—
The authors are indebted to Rosangela Noé and Raquel Gomes for statistical support and to Professor Ottar Sjaastad for his valuable comments.