
Abstract
Background
Evidence on the medium-term clinical course of recurrent headaches is scarce. This study explored the six-month course and factors associated with non-improvement in migraine compared with tension-type headache and cervicogenic headache.
Methods
In this longitudinal cohort study, the six-month course of headaches was prospectively examined in participants (n = 37 with migraine; n = 42 with tension-type or cervicogenic headache). Participants underwent physical examination for cervical musculoskeletal impairments at baseline. Participants also completed questionnaires on pain, disability and other self-report measures at baseline and follow-up, and kept an electronic diary for 6 months. Course of headaches was examined using mixed within-between analyses of variance and Markov chain modeling. Multiple factors were evaluated as possible factors associated with non-improvement using regression analysis.
Results
Headache frequency, intensity, and activity interference in migraine and non-migraine headaches were generally stable over 6 months but showed month-to-month variations. Day-to-day variations were more volatile in the migraine than the non-migraine group, with the highest probability of transitioning from any headache state to no headache (probability = 0.82–0.85). The odds of non-improvement in disability was nearly six times higher with cervical joint dysfunction (odds ratio [95% CI] = 5.58 [1.14–27.42]).
Conclusions
Headache frequency, intensity, and activity interference change over 6 months, with day-to-day variation being more volatile in migraine than non-migraine headaches. Cervical joint dysfunction appears to be associated with non-improvement for disability in 6 months. These results may contribute to strategies for educating patients to help align their expectations with the nature of their headaches.
Introduction
Migraine and other common recurrent headaches such as tension-type headache (TTH) and cervicogenic headache (CGH) may present as episodic attacks, yet persist over time (1–3). To date, knowledge of how these headaches change over time is not fully understood. Evidence from a few longitudinal population-based and clinic-based studies has demonstrated the variable clinical course of migraine and TTH, in particular, over the long term. Specifically, migraine and TTH have been shown to remit in most people, follow a stable course in others, and progress to higher frequency episodes or other poorer outcomes in a few (4–6). For those cases in whom headaches progressed, the following have been identified as predictors: age at onset younger than 20, female, low education and socioeconomic status, white, head injury, high attack frequency, obesity, medication overuse, stressful life events, caffeine overuse, sleeping problems, and other pain syndromes (6–8). Correspondingly, predictors for remission or recovery from headache have been identified, including less severe headaches at baseline, absence of anxiety and sleep problems (8), episodes not triggered by alcohol, absence of associated symptoms (4), and short headache duration (5).
However, less is known about how recurrent headaches change and their associated factors in the medium term, which is often considered more important to patients. One longitudinal observational study has shown that clinical characteristics of migraine remain stable over 3 months, with a general trend toward improvement in disability (9). Additionally, improved disability had a moderate positive association with headache frequency in 3 months. Further evidence is required to build on these findings by identifying the short- to medium-term variations in headaches. Specifically, information regarding day-to-day variation in headaches will be relevant to patients with recurrent episodic headaches such as migraine and non-migraine headaches that present frequently to primary care (TTH and CGH). For many of these patients, daily function is disrupted even on non-headache days because of the unpredictability of their headaches (10) despite undergoing treatment (9).
Knowledge of the medium-term course of common recurrent headaches such as migraine, TTH and CGH will further characterize these headaches and, ultimately, contribute to a greater understanding of their entire clinical course. By knowing the behavior of their headaches in the medium term, patients could form realistic expectations accordingly, which, in turn, could positively influence the way they manage their headaches and reduce their disability. Characterization of migraine and non-migraine headaches could be further broadened when physical impairments that have been reported to be present and treated in these headaches, such as cervical musculoskeletal impairments (11–14), are considered. For example, upper cervical joint dysfunction, as conceivably suggested by the presence of light-headedness, was associated with poor outcome in CGH after one year of active treatment (15). This might be the case for migraine as well; however, this has not been demonstrated. Understanding which factors are associated with poorer short- or medium-term outcomes could assist in mediating or managing these factors toward a more favorable clinical course (7).
Therefore, the primary aim of this study was to describe and compare the medium-term clinical course of migraine and non-migraine headaches in terms of headache frequency, intensity, and interference with activity. A secondary aim was to explore factors that are associated with non-improvement in perceived disability, and headache frequency and intensity in the medium term.
Methods
Design
In this longitudinal observational cohort study, we investigated the clinical course of different headache types and factors that predicted this clinical course by following groups of people with migraine and non-migraine headaches for a period of 6 months. This research was granted ethics approval by the Human Research Ethics Committee of The University of Sydney (Project Number 2014/536).
Participants
We recruited volunteers aged 18–65 with recurrent headache through advertisements posted at community bulletins, social media, and primary and specialist care clinics. Participants were included if they had had headaches for at least one year and had at least one headache episode in the previous month. Participants were excluded if they had known secondary headache classifications (e.g. tumor, substance withdrawal, and so on) or psychiatric disorders. Participants were then classified into the migraine group (fulfilling the criteria for migraine only and not those for other headache types) or non-migraine group (with primary diagnosis of TTH and/or CGH, with or without comorbid migraine) using the ICHD-3 beta criteria (14).
Procedure
All participants underwent initial telephone screening to confirm their eligibility. All eligible participants provided written informed consent prior to participation. Eligible participants then completed questionnaires at baseline regarding demographic and headache characteristics, as well as patient-reported outcomes such as multidimensional pain, disability, and other health measures. Multidimensional pain and disability assessment included the Short-form McGill Pain Questionnaire-2 (SF-MPQ-2) (16), Central Sensitization Inventory (CSI) (17), Henry Ford Headache Disability Inventory (HDI) (18), Headache Disability Questionnaire (HDQ) (19), Headache Impact Test-6 (HIT-6) (20), and World Health Organization Disability Assessment Schedule 2.0 (WHODAS) (21). Other health measures comprised those previously shown to predict the long-term course of headaches. These included the Depression Anxiety Stress Scales-21 (DASS-21) (22) to assess negative emotional states, the Self-Administered Comorbidity Questionnaire (SCQ) (23) to assess comorbidities (4), the Pittsburgh Sleep Quality Index (PSQI) (24) to assess sleep (6), and the International Physical Activity Questionnaire (IPAQ) (25) to measure physical activity (4).
Participants then attended one assessment for interview and physical examination, in which headaches were classified and data for cervical musculoskeletal impairments were collected. Headache classification used ICHD-3 beta criteria (14) independently done by two researchers. Cervical musculoskeletal impairment data comprised joint dysfunction and cervical muscle behavior. These impairments were shown to be different between migraine and non-migraine headache groups in our previous cross-sectional work. Joint dysfunction was assessed through manual examination of the upper cervical spine with passive accessory intervertebral movements (PAIVMs) (26) and the flexion-rotation test (27). Manual examination of the cervical spine was deemed positive if headache was provoked. The flexion rotation test was deemed positive if headache was provoked and the range of movement was ≤32°. Cervical muscle behavior was assessed using the extensor under load test, a new technique that measures changes in thickness of the deep cervical extensor during low load using ultrasound imaging (28).
Participants then filled out an electronic diary daily for 6 months, beginning the day after their physical examination. Participants recorded the presence of headaches daily and provided information on headache intensity using the numerical rating scale (NRS: with anchors at 0 and 10: 0 = no headache, 10 = worst headache possible), and interference of the headache with normal daily activities on a scale of not at all (0), a little bit (1), moderately (2), quite a bit (3), and extremely (4). The diary was administered and data were collected and managed using the Research Electronic Data Capture (REDCap) application (Research Electronic Data Capture, Nashville, Tennessee, USA) (29) hosted at The University of Sydney. Participants also completed the pain and disability questionnaires at 1 month, 3 months, and 6 months after their physical examination.
Statistical analysis
The sample size of the present study was based on the sample size of our previous cross-sectional study (currently under review) (n = 40 per group). This sample size was powered to detect group differences in cervical musculoskeletal impairments, which was the focus of the cross-sectional study.
Distributions of data were examined through visual inspection by a statistician and using the Shapiro-Wilk test. Accordingly, demographic and headache characteristics, and questionnaire scores were summarized as mean and standard deviation (SD). Additionally, baseline clinical characteristics between the migraine and non-migraine groups were compared using Student’s t test, (for continuous variables) or Chi square test (for categorical variables). The month-to-month variation in the clinical course of headaches over 6 months and between-group comparisons were examined using mixed within-between analyses of variance (ANOVA). The day-to-day variation in the clinical course of headaches over 6 months was examined using Markov chain modeling (30). Details of the day-to-day variations derived from Markov chain modeling included the probabilities of transitioning from a given headache intensity and activity interference state to another or the same state on the next day. This approach models the randomness in headache behavior. For Markov chain modeling, intensity was described as ‘no headache’ (NRS 0/10), ‘mild’ (NRS 1–3/10), ‘moderate’ (NRS 4–6/10), or ‘severe’ (NRS ≥ 7/10) to simplify the categories. Markov chain modeling also generated simulated models of the clinical course of headache intensity and activity interference in 30 days in hypothetical individuals with headaches.
The relationship between the dependent variable, absence of clinically-meaningful improvement (i.e. non-improvement of headaches) and independent variables, namely demographic and headache characteristics, cervical musculoskeletal impairments, and scores on multidimensional pain, disability, and other health measures were explored using logistic regression analyses. In the absence of a standard definition of non-improvement of headaches, we defined the primary dependent variable, for the purpose of regression analyses, to be <2.5 point reduction in HIT-6 scores (disability) (31). Secondary dependent variables were <50% reduction in headache frequency (32) and <15% reduction in headache intensity (33). The relationship between dependent and independent variables was initially explored using univariate logistic regression analyses. Independent variables, with p < 0.2 based on the Wald Chi square statistic on univariate analyses, were entered into multiple regression analyses using the ‘enter’ method. In all analyses, headache group was added as an independent variable. Dependent variables were presented as short-term changes (Month 3 minus Month 1) and medium-term changes (Month 6 minus Month 1). Month 1 was considered as the baseline for the change scores in dependent variables; this allowed collection of prospective data from the headache diary for 1 month to serve as baseline data for headache characteristics.
Statistical analyses were conducted using R studio version 3.3.0 2016 (R Foundation for Statistical Computing, Vienna, Austria) and Statistical Package for Social Sciences® statistical software, version 23 (SPSS Inc., Chicago, Illinois, USA) for Windows. Significance level for statistical analyses other than univariate logistic regression was set at 0.05.
Results
Participants
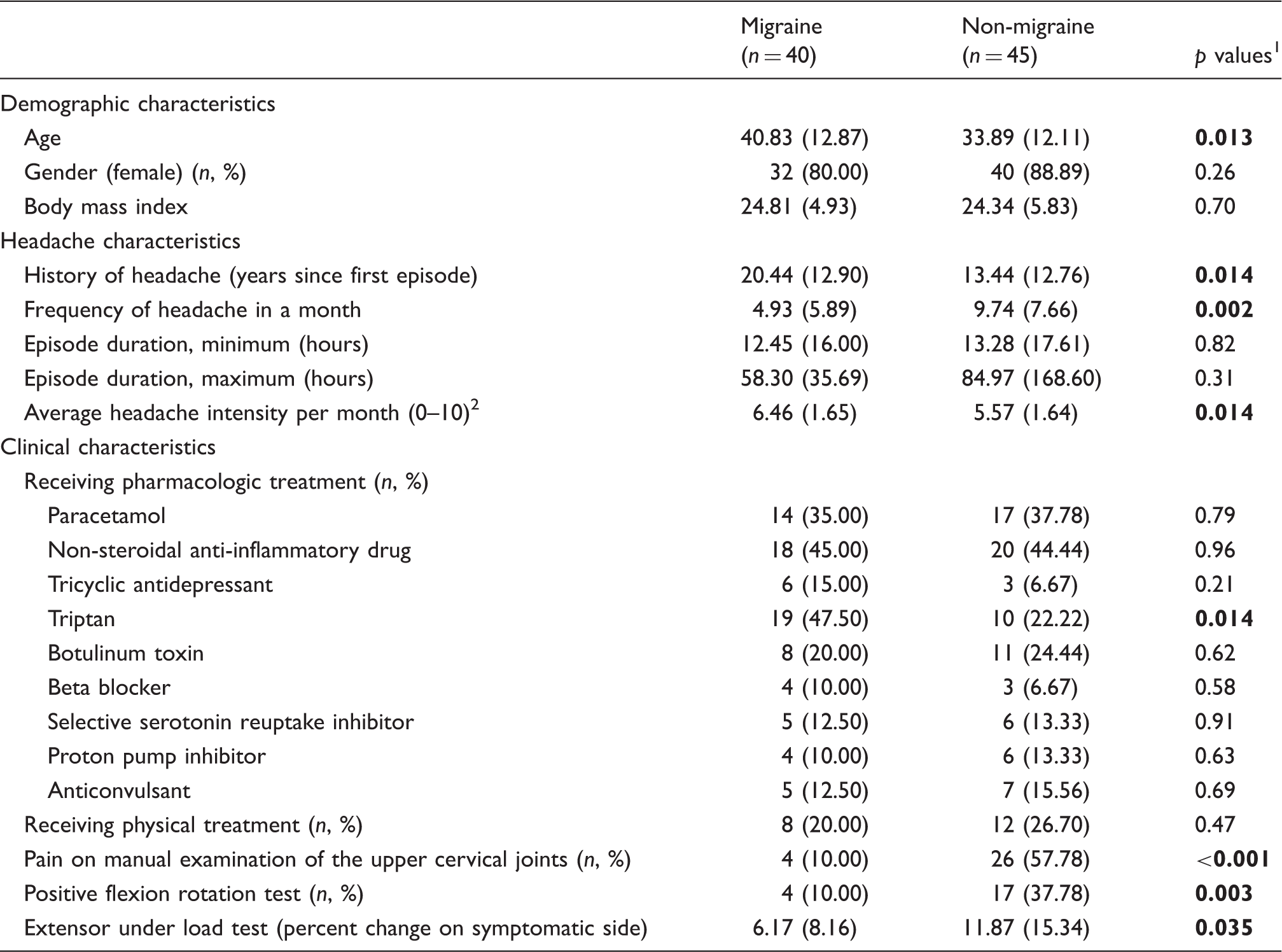
Forty people with migraine and 45 people with non-migraine headache (mean age [standard deviation] = 37.15 [12.88] years) participated in this study. The flow of participants through the study and reasons for exclusion from analyses are shown in Figure 1. Demographic, headache and clinical characteristics of participants at baseline are presented in Table 1. The migraine group had a longer history of headache (mean [SD] 20.44 [12.90] years versus 13.44 [12.76] years; p = 0.014), less frequent headaches in a month (4.93 [5.89] versus 9.74 [7.66]; p = 0.002), and higher average headache intensity per month (6.46 [1.65] versus 5.57 [1.64]; p = 0.014) than the non-migraine group. More participants in the migraine group were taking triptan than the non-migraine group (n [%] 19 [47.50] versus 10 [22.22%] participants; p = 0.014). Fewer participants in the migraine group had cervical musculoskeletal impairments than the non-migraine group. For example, four (10.00%) participants from the migraine group reported pain on manual examination of the upper cervical joints compared to 26 (57.78%) participants from the non-migraine group.
Flow of participants through the study. Baseline characteristics of participants (mean [SD] or n [%] where indicated) (n = 85). Note: Bold numbers indicate statistical significance (p < 0.05). p-values for Student’s t-test for continuous variables; p-values for Chi-square test for categorical variables. Headache intensity: Numerical rating scale 0–10; 0 = no pain, 10 = worst possible pain.
Clinical course of migraine and non-migraine headaches
Headache characteristics changed over 6 months for both headache groups without fully remitting or progressing (Figure 2). Headache frequency fluctuated from month to month in both headache groups (Figure 2(a); p = 0.001), with the migraine group showing more fluctuations than the non-migraine group (p = 0.005). The migraine group consistently had fewer headaches per month than the non-migraine group.
Month-to-month variation in headache characteristics in migraine and non-migraine groups. (a) Frequency of headaches. (b) Average headache intensity. (c) Average activity interference due to headache.
Transition matrices of headache intensity showing the probability of transitioning from a current headache intensity state (denoted by rows) to the next-day headache intensity state (denoted by columns). (a) Migraine group. (b) Non-migraine group (p < 0.001).

In contrast, the day-to-day transition between headache intensity states of the non-migraine group ranged from a probability of 0.04 (from no or mild headache to severe headache the next day) to 0.76 (from no headache to remaining without headache the next day) (Table 2(b)). The migraine group generally had the greatest probabilities of transition from any headache state to no headache. The transition probabilities for headache intensity differed significantly between the headache groups (p < 0.001), with the migraine group showing more volatility. Based on the transition probabilities, any headache intensity would have higher probabilities to have no headache the following day in migraine. In contrast, any headache intensity would have higher probabilities of staying the same or having no headache the following day in non-migraine headaches. The day-to-day volatility of headache intensity in the migraine group was highlighted when modeled using Markov chains (Figure 3).
Simulated day-to-day clinical course of headache intensity of 12 hypothetical individuals with headaches over 30 days (numerical rating scale; 0, no headache, to 3, severe headache. (a) Migraine group. (b) Non-migraine group (p < 0.001).
Transition matrices of activity interference caused by headache for migraine group showing the probability of transitioning from a current activity interference state (denoted by rows) to the next-day activity interference state (denoted by columns). (a) Migraine group. (b) Non-migraine group (p < 0.001).


Simulated day-to-day clinical course of activity interference of 12 hypothetical individuals with headaches over 30 days (activity interference rated using a scale; 0, not at all, to 4, extremely. (a) Migraine group. (b) Non-migraine group (p < 0.001).
Factors associated with non-improvement of migraine and non-migraine headaches as to headache-related disability, headache frequency and intensity
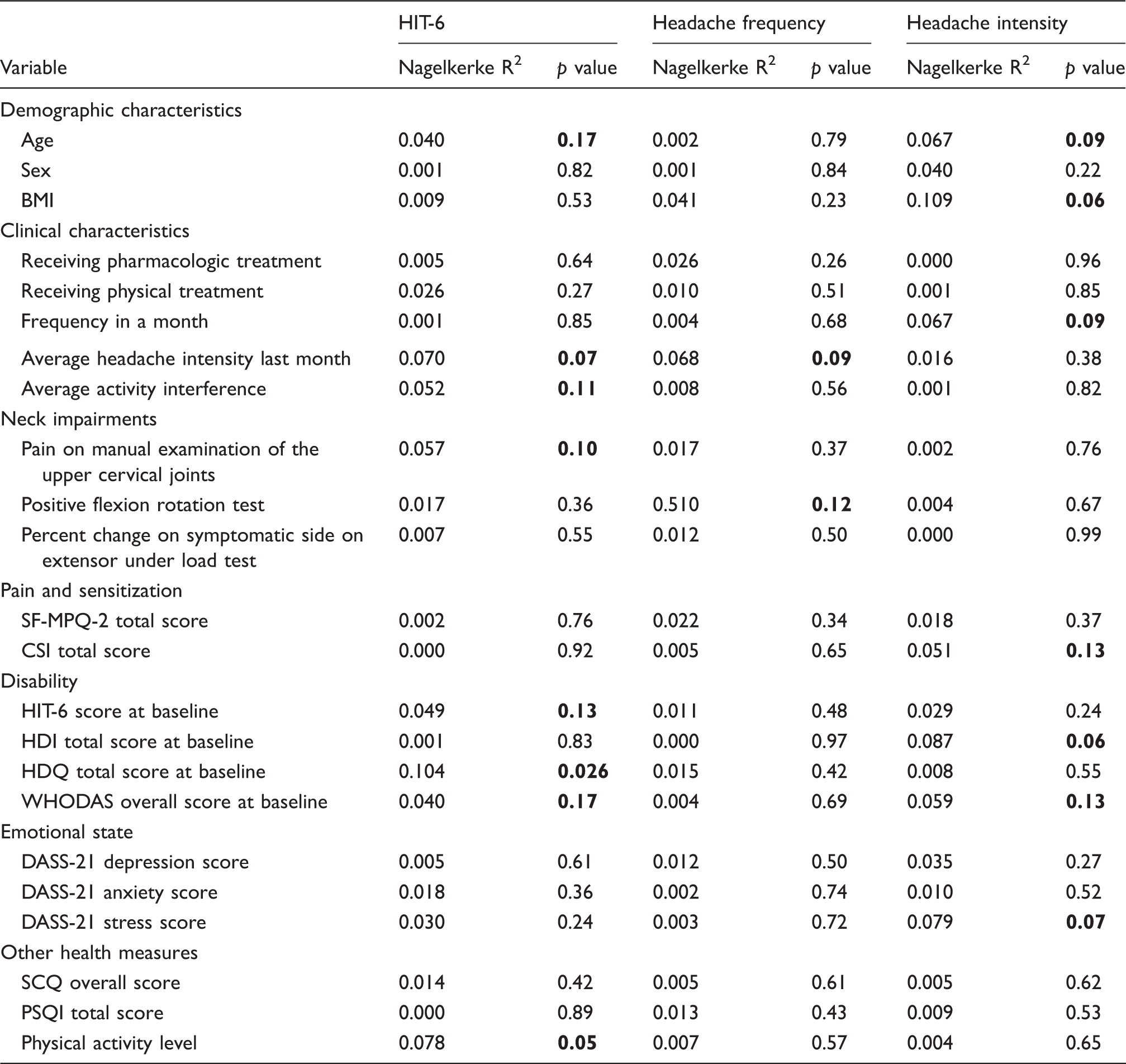
Univariate logistic regression analysis showing relationships between possible predictors of non-improvement in headache characteristics in the short term.

Abbreviations: BMI: body mass index; CSI: Central Sensitization Inventory; DASS-21: Depression Anxiety Stress Scales-21; HDI: The Henry Ford Headache Disability Inventory; HDQ: Headache Disability Questionnaire; HIT-6: Headache Impact Test-6; PSQI: Pittsburgh Sleep Quality Index; SCQ: the Self-Administered Comorbidity Questionnaire; SF-MPQ-2: Short-form McGill Pain Questionnaire-2; WHODAS: World Health Organization Disability Assessment Schedule.
Note: Bold numbers indicate possible predictors with p < 0.2.
Univariate logistic regression analysis showing relationships between possible predictors of non-improvement in headache characteristics in the medium term.
Abbreviations: BMI: body mass index; CSI: Central Sensitization Inventory; DASS-21: Depression Anxiety Stress Scales-21; HDI: The Henry Ford Headache Disability Inventory; HDQ: Headache Disability Questionnaire; HIT-6: Headache Impact Test-6; PSQI: Pittsburgh Sleep Quality Index; SCQ: the Self-Administered Comorbidity Questionnaire; SF-MPQ-2: Short-form McGill Pain Questionnaire-2; WHODAS: World Health Organization Disability Assessment Schedule 2.0.
Note: Bold numbers indicate possible predictors with p < 0.2.
Multivariate logistic regression predicting likelihood of non-improvement in headache characteristics in the short term.

Abbreviations: BMI: body mass index; CSI: Central Sensitization Inventory; DASS-21: Depression Anxiety Stress Scales-21; HDQ: Headache Disability Questionnaire; HIT-6: Headache Impact Test-6; WHODAS: World Health Organization Disability Assessment Schedule 2.0.
Note: Bold numbers indicate statistical significance (p < 0.05).
Multivariate logistic regression predicting likelihood of non-improvement in headache characteristics in the medium term.

Abbreviations: BMI: body mass index; CSI: Central Sensitization Inventory; DASS: Depression Anxiety Stress Scales-21; HDI: The Henry Ford Headache Disability Inventory; HDQ: Headache Disability Questionnaire; HIT-6: Headache Impact Test-6; WHODAS: World Health Organization Disability Assessment Schedule 2.0.
Note: Bold numbers indicate statistical significance (p < 0.05).
Discussion
This study demonstrated three main findings on the 6-month clinical course and factors associated with outcome in migraine and non-migraine headaches. First, the clinical course of headache characteristics in migraine and non-migraine headaches showed month-to-month variability, but generally did not remit nor progress. Second, day-to-day variations in headache intensity and activity interference were more volatile in the migraine group than the non-migraine group. Third, a number of demographic, clinical and patient-related factors were associated with persistent disability over 3 and 6 months. These findings further characterize and differentiate migraine and non-migraine headaches, thus informing clinical practice and research.
The month-to-month variation in headache frequency, intensity, and interference in activity in migraine and non-migraine headaches changed, but did not fully remit nor progress. These results are consistent with existing evidence for the 3-month clinical course of migraine (9) and show a similar trend to the prevailing knowledge on the long-term clinical course of changes in migraine (4,34). Headache intensity fluctuated around moderate intensity for both headache groups, challenging the typical picture of migraine as a more severe headache than non-migraine headaches (14). Analogously, activity interference caused by headaches over 6 months hovered between little to moderate interference for both headache groups. This range of activity interference contrasts with the high levels of disability associated especially with migraine and TTH (35). On closer consideration, such disparities in intensity and activity limitation ratings are understandable, and may be partly attributed to measuring intensity and activity interference prospectively using a headache diary. First, retrospective rating by patients tends to overestimate headache intensities compared with information from diaries (36). Second, the perceived impact of the headache on daily activities measured each day could be lower compared to perceived disability over extended periods as captured by self-report questionnaires.
This study also presents new evidence that characterizes the day-to-day variation in headache intensity and activity interference as being more volatile in migraine than in non-migraine headaches. This greater volatility in migraine, as demonstrated by Markov chain analyses, is related to the higher probability of having no headache on the following day regardless of the current headache state. Further, the different possible scenarios of transitioning between headache states imply that the extent of volatility may be different between individuals with similar headache diagnoses, undergoing their usual treatment, and having the same level of headache intensity and activity interference on a particular day.
This study also presents preliminary evidence that factors influencing non-improvement in disability in 6 months include headache features, cervical joint dysfunction, disability, and physical activity. This preliminary evidence presents prospective directions for future research. Of note is cervical joint dysfunction, which appears to be associated with non-improvement in disability in both migraine and non-migraine groups yet was less frequent in the former (10.00% versus 57.78%). The lack of factors significantly associated with non-improvement in frequency and intensity may most likely be indicative that no factor significantly influences those outcomes in the short-to medium-term. The same can be said for non-improvement in disability in the short term. However, the multifactorial model for disability explains 27.7% and 32.3% of the variability in the model in the short and medium term, respectively. The association of these factors with disability needs to be further investigated in larger cohort studies with pure headache groups. Prospective studies may also explore other factors that would influence non-improvement in disability.
Results of this study inform headache management. First, information about the month-to-month and day-to-day variation in features of migraine and non-migraine headaches can form part of patient education. Importantly, educating patients about the most likely behavior of their headaches will help them align their expectations. This information could also be reassuring for patients who perceive the unpredictability of their headaches as disabling and disquieting (10,37). Second, the small but statistically-significant month-to-month variation in headache characteristics over 6 months justifies continued monitoring of symptoms as part of headache management. Third, the association of cervical joint dysfunction with non-improvement in headache-related disability in 6 months reveals the usefulness of cervical joint assessment and, if necessary, targeting any impairments to help reduce disability in the short to medium term.
The study aimed to describe the shorter-term clinical course of migraine and non-migraine headaches with participants having their usual headache management, when interventions were not standardized. As such, we did not control for intervention and other possible confounding factors that could influence the course of headaches. Prospective clinical trials are indicated to investigate those other factors, to build on evidence from this study. Such trials can also use evidence presented here concerning the 6-month clinical course of migraine and non-migraine headaches when selecting outcome measures. Further studies involving pure headache groups and collecting longitudinal data on possible variables influencing non-improvement are also required to validate our results. Investigating the underlying mechanisms explaining the difference in month-to-month and day-to-day variation between migraine and non-migraine headaches also remains an area for future investigation.
In conclusion, headache frequency, intensity, and activity interference show month-to-month and day-to-day variations over 6 months in individuals with migraine and non-migraine headaches who are already receiving treatment. Day-to-day variations in headache intensity and activity interference are more volatile in migraine compared with non-migraine headaches. Cervical joint dysfunction measured using manual examination appears to be associated with non-improvement in headache-related disability in 6 months. These results will contribute to strategies for patient education regarding the nature of their headaches, and carry implications for outcome measure selection in prospective clinical trials.
Clinical implications
Headache frequency, intensity and activity interference show variations over 6 months, but generally do not fully remit nor progress in individuals with migraine and non-migraine headaches. Day-to-day variation in headache intensity and activity interference is more volatile in migraine than non-migraine headaches. Individuals with migraine or non-migraine headaches who have cervical spine dysfunction are nearly 6 times more likely not to recover in terms of headache-related disability within 6 months. These results contribute to strategies for educating patients on the nature of their headaches. The need to consider volatility of headache characteristics when selecting outcome measures for prospective clinical trials is highlighted.
Footnotes
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. We thank all the participants for their cooperation, and the staff of the Sydney Specialist Physiotherapy Centre for their support during the conduct of this study. We also thank the following for their help in recruiting participants: Headache Australia, Australian Pain Society, Australian Pain Management Association, Painaustralia, the editorial team of Ang Kalatas Australia, and Dr Craig Moore and the staff of Spinal Solution. We also acknowledge Dr Jillian Clarke for her technical assistance with setting up the parameters for real-time ultrasound imaging.
Maria-Eliza Aguila was supported by a fellowship through the Doctoral Studies Fund under the Expanded Modernization Program of the University of the Philippines. Trudy Rebbeck was supported by a fellowship from the Australian National Health and Medical Research Council (NHMRC).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.