
Abstract
Whiplash is a controversial concept. The real nature and prevalence of whiplash-related headaches are not known. To address this issue, the history of severe trauma was collected from occipital/nuchal headache-cervicogenic headache, migraine and tension-type headache patients attending a neurology office. The two last groups of patients had significantly less history of trauma in their medical records, with longer time span between the injury and the headache onset. Whiplash may induce preferably cervicogenic and tension-type headaches.
Introduction
Harold Crowe coined the term ‘whiplash’ in 1928 at the Western Orthopaedic Association meeting in San Francisco, during a presentation of eight cases of neck injuries following traffic accidents. Crowe wrote himself in 1964 (1): ‘I used the unfortunate term whiplash. This expression was intended to be a description of motion, but it has been accepted by physicians, patients and attorneys as the name of a disease’. Whiplash and its corresponding expression ‘WAD’ (whiplash-associated disorders) have remained as controversial concepts ever since (2, 3), among other reasons, mainly because of: the relative lack of objective biomarkers allowing precise diagnoses; the paucity of studies; the methodological constraints; and the influence of medico-legal issues. Previous studies have suggested that headache following whiplash would occur mostly in connection with legal compensation (4). The important questions to be answered are whether whiplash really induces a de novo headache, and what is its most frequent clinical picture. To address this matter, a series of primary headache patients was investigated correlating previous trauma events with the subsequent headache picture.
Patients and methods
Records from a series of 2771 patients personally examined by the author between 1993 and 2006 were reviewed. Informed data on previous trauma (severe enough to require medical care, mostly car accidents) was collected from the files and correlated with the headache picture. Three groups of headache patients were focused on in particular: migraine (M), tension-type headache (TTH), both diagnosed according to the 1988 IHS criteria (5), and cervicogenic headache (CEH), diagnosed according to Sjaastad et al.'s criteria (6). Patients with mixed or unclassifiable headache syndromes were excluded. Subjects suffering from occipital/nuchal pain not fulfilling the diagnostic criteria of cervicogenic headache were considered together with CEH patients (Neck/CEH) for data analysis. P-values < 0.05 were considered significant (chi-square and
Results
Among 2771 patients, 1429 were diagnosed as migraine, 400 had TTH and 93 suffered from Neck/CEH. Previous trauma was reported by 19
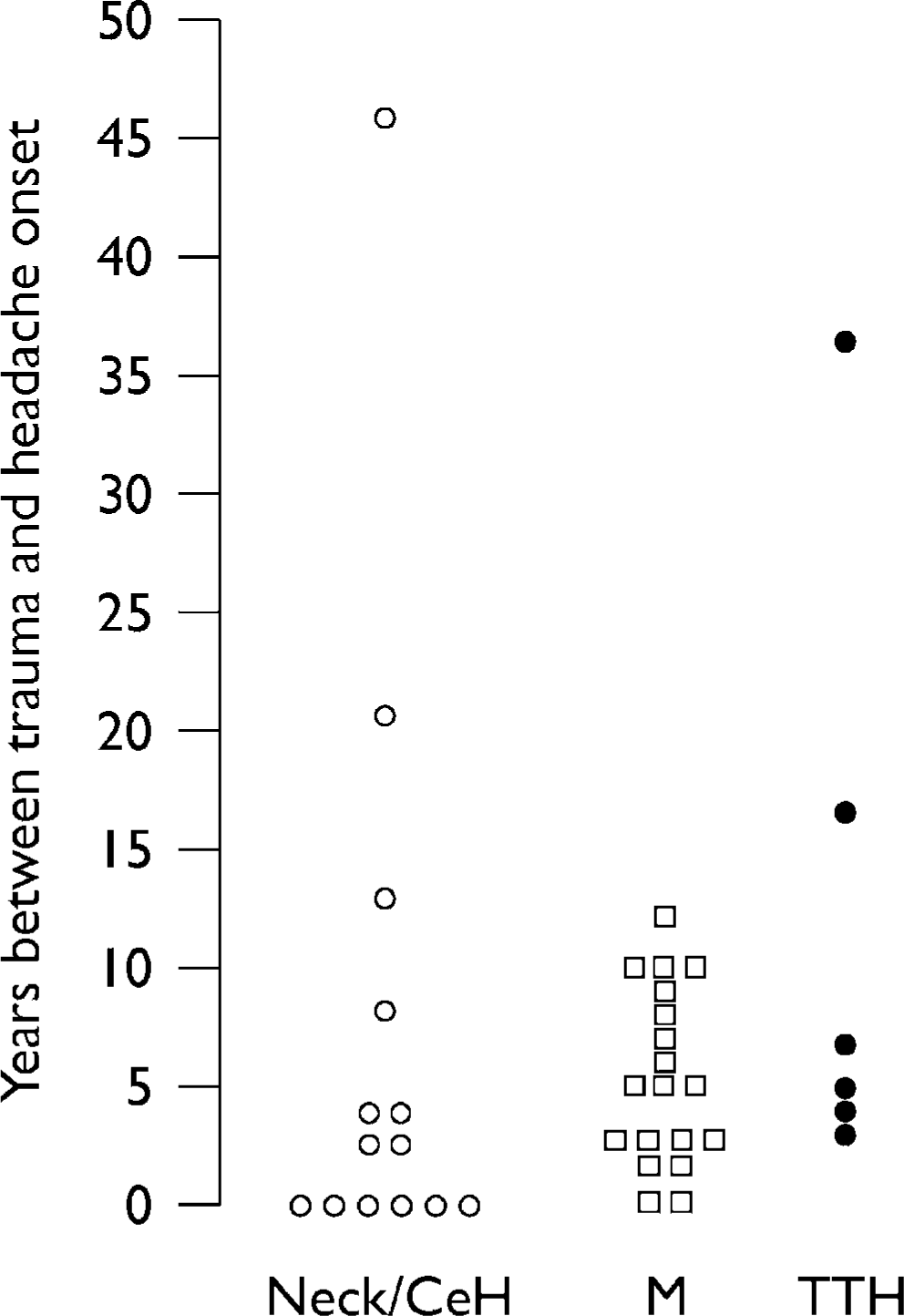
Time span (years) between trauma and headache onset in patients with occipital-nuchal headache or cervicogenic headache (Neck/CeH, n = 14, open circles); migraine (M, n = 19, squares) and tension-type headache (TTH, n = 6, filled circles).
Discussion
Contrary to headache studies based on whiplash/trauma cohorts (4, 7, 8), the present analysis looked for history of trauma in patients who came to the office because of headache, irrespectively of past injury or compensation demands. Although recall may have interfered with the results, a severe trauma is expected to be remembered forever. Some of the accidents reported in this series could not have been of the whiplash type. Although precise information on the type of accident was not available, the nature of the accidents, however, most probably involved a whiplash-type of movement.
Data show that Neck/CEH patients had suffered more frequently a severe trauma as compared with M and TTH patients. As some headache patients were examined many years after the headache onset, it is possible that the injuries induced permanent headaches in at least some subjects. In addition, the headache onset was significantly closer to the injury in the Neck/CEH group. This suggests that the trauma could have had no implication for the development of pain in the M and TTH groups, at least in some of the patients. A substantial number of individuals with CEH, neck and/or occipital headache (89%) had not suffered a previous serious accident, indicating that injuries are not a requisite for such pain. Besides, many whiplash patients will never develop a headache. Obelieniene et al. found that whiplash is not related to chronic headache (4), in opposition to other studies (7).
Theoretically, the headache–whiplash interrelation should be considered in many ways. Trauma may happen in patients already suffering from a primary headache. In this case, the accident could either worsen or simply modify an existing pain. Another possibility is the development of a new trauma-induced headache as an add-on pain. An injury-related headache in a symptom-free subject may present with different clinical pictures. In all cases, the pain may start close in time to the trauma or not; it may be either short, long lasting or permanent. The headache could also occur just by coincidence, with no cause–effect relationship with the previous trauma. Therefore, the present data do not indicate that trauma necessarily induced the headache in all the subjects, but do suggest that when there is pain following trauma, it is (i) less frequently of the migrainous type, and (ii) tends to start right after the injury, if it is in the posterior part of the head or of the CEH type.
Medico-legal issues have been implicated in the WAD context (9). The trauma-related headaches in the present material were not influenced by any compensation, as all the patients were examined specifically because of their pain complaints. No one required reports for legal reasons or mentioned involvement with any type of legal actions. This is not in accordance with previous data suggesting that outside the legal circumstance whiplash-induced headaches would occur much less frequently.
A trauma-induced headache may be short or long lasting. If long lasting, it seems plausible to believe that the trauma produces a permanent injury that maintains the pain. If short lasting, the trauma could just reduce temporarily the pain threshold without a permanent lesion, as suggested in Pearce's material (8). Functional changes have been observed following whiplash, with reduced cervical motion (10). Alar ligaments were found to be particularly injured after whiplash (11), but such findings remain to be confirmed with modern imaging techniques. The actual nature of the whiplash-related lesion responsible for long-lasting head pain is not known.
Migraine may be dependent on a predisposition, probably genetic (12). Speculatively, there are three scenarios for a post-whiplash headache in a given patient as far as previous migraine predisposition is concerned: (i) no migraine predisposition; (ii) migraine predisposition but no manifest migraine; and (iii) clinically active migraine. It is possible that a whiplash trauma induces different pictures according to these three scenarios. Accordingly, the whiplash-related headache could be, respectively: (i) cervicogenic headache; (ii) cervicogenic headache with migrainous features such as nausea, photo- and phonophobia; and (iii) cervicogenic headache coexisting with migraine, or worsening of the previous migrainous pain. If taken into consideration, different backgrounds in terms of migraine predisposition could explain the existence of several nuances in post-whiplash headaches, and why some of them would be so similar to migraine as in opposition to others. This could help the understanding of the sometimes so-considered inaccurate boundary between migraine and neck-generated headaches.
To conclude, based on the present study and available data, whiplash may induce short lasting as well as chronic headaches, mostly CEH and/or tension-type, the latter located preferably to the back of the head and nuchal areas. New headaches following whiplash may coexist with previous headache disorders or modify their course. The clinical picture may depend on individual predisposition to headache, as well as perhaps age, type of accident, among other factors. It is possible that cultural and legal issues interfere with the expression of WAD in terms of headache to some extent, but most probably do not justify head pain in all the cases.
Conflicts of interest
The author has not declared any conflicts of interest.