
Abstract
Migraine is a complex neurobiological disorder that extends beyond physical symptoms to encompass profound mental, emotional and existential dimensions. Despite its prevalence, the philosophical aspects of migraine remain underexplored in scientific research. This review examines migraine through a philosophical lens, addressing questions of pain, suffering, consciousness and communication. It highlights the different perspectives of neuroscientists, clinicians and patients: the former seeks to understand migraine as a neurological dysfunction, while the latter experiences it as an intensely personal and subjective affliction, and the clinicians try to build a bridge. Bridging these perspectives requires a multidisciplinary approach, integrating neuroscience, philosophy and patient narratives. Philosophical reflections posed by Nietzsche (How should we confront suffering?), Sartre (existence precedes essence) and Camus (How can we accept the absurdity of life and still continue to embrace life fully?) provide a framework to understand the subjective experience of pain and its meaning in human existence. By considering migraine both as a subjective and objective phenomenon, this work advocates for a holistic, patient-centered approach to treatment. It argues that addressing migraine's multifaceted nature, including its physical, emotional, cultural and existential dimensions, can lead to more meaningful and effective therapeutic strategies. This interdisciplinary exploration aims to inspire clinicians to embrace a more comprehensive and empathetic framework for migraine care, a human-to-human service.
This is a visual representation of the abstract.
Introduction
Migraine is a rather prevalent complex neurobiological disorder. However, literature on the philosophical aspects are scarce in the scientific libraries. If you enter the search terms “migraine” and “philosophy” or “philosophical”, you only retrieve some publications on the medical history of Blaise Pascal, Friedrich Nietzsche or Immanuel Kant (1–3). However, even if you search for “pain” and philosophical aspects, you retrieve no more than 270 publications.
Although only few philosophers have explicitly addressed migraine, medical practitioners have frequently discussed its philosophical dimensions, highlighting its complex and multifaceted nature. More than just severe headaches, migraine attacks are neurological processes that disrupt not only physical well-being, but also a person's mental, emotional and existential experience. By exploring migraine through a philosophical lens, we can gain insights into the nature of pain, suffering, consciousness and the challenges of translating intensely personal experiences into universal language. The purpose of this review is to show the clinicians some aspects of fundamental and more contemplative questions about migraine that are often neglected in the research literature as well as in clinical dialogue, namely the philosophical ones.
Methods
This work stems from a lecture on the philosophical aspects of migraine, originally prepared by the first reviewer (MJE) over a decade ago and subsequently delivered multiple times. As previously noted, the scientific literature addressing philosophical concepts in migraine is sparse. Philosophical literature predominantly discusses pain in general, existential distress and suffering, but rarely touches upon migraine. A systematic and expanded discussion thereof would not be sensible in our context.
In the present review, we attempt to apply practical philosophical methods in order to achieve a synoptic view of the complexity of migraine. These are phenomenology – the description of experience, hermeneutics – the understanding of meanings, clarification of language and concepts, philosophical reflections, ethical considerations on norms and values, and asking Socratic questioning (4). It is the aim of this work to promote a holistic, patient-centred approach, comprising an integration of data-based and human-based medicine. This interdisciplinary pluristic perspective exploration aims to inspire clinicians to embrace a more comprehensive and empathetic framework for migraine care.
Discussion
The clinician: between objective neurobiology and subjective experience
Whoever uses the term “migraine” recognizes that a lot has to be prepared in language for the mere naming to make sense (5,6). From the external perspective of the neuroscientists, this term refers to a widespread, complex, neurobiological dysfunction of the pain-regulating systems of the brain, meninges and blood vessels. They define, what is migraine (objective knowledge)? From the patients’ internal perspective, the term means a painful, subjective suffering with unpleasant accompanying symptoms. They ask about the experience, how does a migraine feel like (subjective experience)? The clinicians stand between these two worlds, which face each other but are not comparable (Figure 2). They search for methodological approaches and philosophical reflections to build a bridge between the two perspectives with the intention of deriving a therapeutically meaningful convergence. And they are looking for a smart way to find the right (treatment) decision.

Migraine in a complex system: a transdisciplinary approach, theories, explanation and reflection.
The clinician is challenged with the problem of consciousness, as formulated by the Australian philosopher David Chalmers (7). He argues that the subjective dimension is not explained simply by describing neural processes. Even if we knew how the brain processes stimuli, the question of why and how such processes are associated with subjective experience remains unanswered. There appears to be an explanatory gap between the physical description of the brain (e.g. biochemical processes, electrical signals) and the explanation of why these processes give rise to subjective experience in the first place.
After all, when pain and anxiety are high, contemplation is essential (8). To understand the sufferer's experience, knowledge about migraine in general is necessary but not sufficient because the dimension of personal experience has to be added. Migraine pain is an intense, intimate experience, an affective distress, often accompanied by sensory disturbance and nausea, as well as the uncertainty and worry that something bad might be happening.
Suffering prompts individuals to confront the limits of their endurance and to search for meaning in adversity. Some might find solace in the notion that suffering builds character or fosters empathy, while others may feel that chronic pain serves no purpose and only detracts from the quality of life. Interestingly, a recent study showed that both high and low headache frequencies facilitate adaptation to the disorder, with a higher satisfaction or happiness in life (9). It was hypothesized that this non-linear relationship between happiness and headache frequency might be due to “hedonic habituation” and implies that headache calendars do not necessarily correctly reflect patients difficulty to feel well despite the disorder.
Fuchs goes one-step further by saying that the reality of “my pain” is of a fundamentally different nature than the reality of objective physiological facts; namely, a holistic, subjective state of experience, an expression of life and a reaction of the entire organism to a stimulus (10). It is not the anatomical body, but the lived body that forms the basis for all our life processes. The lived body is the place of perception, cognition and behaviour through which we experience the world as an embodied self.
As early as 1961, in his philosophical anthropology, Helmuth Plessner described the strain between an inner and outer body perspective as the basic condition of being human (11). Humankind is thrown back on his bodily existence, while at the same time trying to find meaning and significance for the suffering from an eccentric perspective.
What strategies does the clinician have to transform the apparent contradiction between measurable facts and personal experience into a meaningful, understandable dialogue with the patient?
The power of language: between inner pain and outer reality
The link between the internal and external perspective is communication. Painful sensations and disturbing thoughts, although difficult, must be clothed in words to be communicable, and feelings are thus externalized (12,13). Language is our common life practice. According to Watzlawick et al. (14), every linguistic and non-linguistic communication has a content and a relationship aspect. They ask what is being said and how it is being said. Through the statements, the person affected can communicate cognitively and emotionally (communicated emotions versus emotional communication) and thus expand the solitary reflection into a joint discussion (8). Those who tell their migraine story are therefore no longer alone. However, because migraine is often an “invisible” illness, sufferers may encounter scepticism or rejection from others, including healthcare professionals (15). This lack of recognition can add to the suffering of migraine sufferers as they are pressurized to “prove” their pain or downplay its impact on their lives (16).
The clinicians must realize that patients always tell their own truth, which they believe in, which they have the courage to do. Alternatively, they perceive language as a “private matter”, as Wittgenstein described it in his Philosophical Investigations and conceal essential information in the taking the history, for whatever reason (5). They may remain silent, repressed and hidden. The process of narration, the narrative, thus becomes a bridge between the subjective and objective perspective and may not only have a therapeutic effect, but also enrich the interpretative framework.
The narrative dimension of my migraine: personal reflections
I am Mark, a migraine sufferer for years, and I have learned that my life is inseparably intertwined with the story I tell about my pain. In the darkest moments, when migraine and its accompanying symptoms strike me with relentless intensity, I recall how crucial it is to narrate my suffering in order to be understood. Language, my storytelling, then opens up a space where many, not just one, responses become possible. Within this space, my suffering gains a voice, acknowledgment, and solace.
At times, I employ metaphors and imagery to give tangible form to my pain, making it relatable to others. This figurative language unlocks avenues where my migraine can not only be communicated but also metaphorically represented. Thus, storytelling itself becomes an act of liberation, a validation of my experience.
The path to alleviating migraine pain does not solely lead to medical or non-medical treatments, but also to narrating one's personal, intimate story – a practice that, as Plato hinted, can break through negative thinking. By expressing my pain, I discover opportunities that help me overcome darkness and seek new paths.
This is who I am – with my migraine, yet also with the strength to share my story and the hope to be allowed to do so. For it is in the sharing of my suffering that lies the opportunity not only to be understood, but also to find a way to a life where my migraine and my hope are interwoven.
***
I am Praxedis, a migraine sufferer. In phases of pain, I am all migraine, with every fibre of my being, it shapes me, it dominates me, it turns me off and it prevents me (translated with DeepL®) (17). It puts me back. In good phases, which hardly ever last longer than a week, I refuse to talk about migraine, I try to put a spell on it, banish it to a knothole in my existence and keep it silent. I am a journalist, I have spent 50 years of my life working in varying degrees of intensity, I have earned my living by writing. I've written about heaven knows what. But never a word about hell in my head.
I am lying in bed in the bedroom, my husband and the children are downstairs in the parlour, it is the weekend, he is looking after them. He goes shopping with them, he takes them for walks, he keeps them playing outside in the garden. He does homework with the eldest, he takes them to visit his mother-in-law. She cooks for everyone because I can't get up. Do you have a headache today, the children ask when I wake them up in the morning. Do you have a headache today, I asked my mum every morning as a child.
But then, in the middle of an attack, when I am hanging my face over the toilet bowl, when I slump back into bed half unconscious from the pain, sometimes a voice inside me asks: What am I being punished for? Who is beating me from afar and why? The presence of this pain, which consumes almost half of my time, has something biblical about it, it is an archaic narrative that echoes in the dark corridors of human existence. In the past, … I might have been considered possessed.
How can the process of storytelling – as a transformative force, the narrative sharing of one's own “pain story” – translate isolated, subjective suffering into a shared discourse?
Emotions and the search for a meaning
Every experience of pain with all its consequences and every narrative about it is emotionally based (18). Negative emotions often arise, such as fear (uncertainty), anger (perceived helplessness or injustice of the situation), shame (feeling of weakness or inadequacy), sadness, resignation (in the case of persistent stress) or feelings of guilt (having caused the pain through one's own behaviour or omissions). It is not only the pain that worries, but also above all the thoughts and emotions of possible causes and their uncertain consequences. This confrontation can lead to a downward spiral, a vicious circle: the uncertainty, the helplessness and the feeling of guilt intensify the fear, anger and resignation, and in return intensify the feeling of pain. The more important in such a situation is the empathic, attentive dialogue of the clinician. Philosophers such as Virginia Woolf, who herself suffered from migraine, have noted that society often does not take “invisible” suffering seriously and emphasize the need for more empathy and understanding (19). Empathy is about the ability to recognize and understand other people's pain, thoughts and feelings, and it is about “mutual being-for-one-another” (20).
Migraine confronts the sufferer with the borderline experience of their own physicality and their ability to endure this experience, the limits of language, the possibility of reflection, resilience and reasonableness, physical exhaustion, aura as a surreal state, and pain as a break with normality (21). Every clinician knows the situation when patients lose their speech before or during a migraine attack, what remains is a blank stare, tears and silence. With chronic migraine in particular, it is no longer just about the headache and its accompanying symptoms, but about suffering, about the question of meaning for everyday life, about the question of meaningfulness, meaninglessness. This makes philosophical reflections all the more important.
If we define philosophising as pausing and reflecting, as contemplation, as asking for meaning and connections, this leads us to Friedrich Nietzsche: it was not the suffering itself that was the problem, but the fact that there was no answer to the cry of the question “why suffer?” (22). Perhaps because there is no adequate explanation for the pain because headaches are beyond the interpretation and treatment possibilities of modern medicine, because even esoteric explanations seem implausible and are therefore useless, and because malice and violence lead to headache and silence is demanded. The unpredictability of migraine brings up existential questions about control, vulnerability and the human condition (23,24). Migraine is unforeseeable, with sufferers unable to know if, when or where an attack will strike. This uncertainty forces individuals to confront the limits of their control over their own body and live, a theme central to existential philosophy.
An existential question was already emphasized by Jean-Paul Sartre through the concept of facticity, or “being thrown”, that human is thrown into a world whose conditions he/she has not chosen (25). The recurring headache can represent an existential confrontation with absurdity, as Albert Camus also described in his essay The Myth of Sisyphus (26). He shows us that, although suffering may be unavoidable, people always have the opportunity to develop an inner attitude towards it – an attitude of defiance, dignity and solidarity.
For us clinicians, it is therefore not just a matter of alleviating pain, but also of accompanying the patient in his existential dialogue and giving him space to develop his own individual attitude. Many migraine sufferers develop a heightened awareness of their body and a sense of gratitude for pain-free days, finding meaning in the contrast between illness and health. A newer concept that may unravel quality of life measures (27).
How does the emotional experience of pain influence the self-perception and quality of life of those affected?
Migraine between spirituality and value systems
Those who cannot answer the question of why the pain and why the suffering, neither alone nor in their social environment, who fear the real headache and cannot recognize any meaning in it, can at best turn to a supernatural authority, to a spiritual power that can explain what modern medicine is not capable of (28). In spiritual or religious systems, suffering is often interpreted as a test, as preparation for a higher goal. Such ideas can offer the sufferer comfort and a broader perspective by embedding the suffering in a cosmic or divine order. A migraine attack could therefore provide access to transcendental experiences, from which religious and spiritual-philosophical observation and treatment options can be derived.
Although scientific, data-based medicine has a claimed access to migraine, this must not be exclusive. It is – as shown – obvious and therefore necessary to consider the subject-orientated approach on an equal access, knowing well that migraine is primarily a subjective, painful condition. Only by recognizing and consequently explaining the individual parts of migraine – the internal and external perspective – it is possible to understand the overall context (see Tables 1 and 2). In other words, we are confronted here with a hermeneutic circle, which, according to Heidegger, makes it clear that understanding is not a linear process, but develops from a constant interplay between the part and the whole (29). This results in a continuous movement: from the individual to the whole: to understand migraine, one must first understand its individual components. From the whole to the individual: simultaneously, the individual aspects of migraine can only be properly interpreted when one knows the entire clinical picture. The whole and the parts influence and deepen each other.
What influences do secular, spiritual, religious, cultural or ethical value systems have on the interpretation of migraine?
The complexity of migraine: from molecular mechanisms to cultural dimensions
Every clinician understands that migraine represents a complex system, comprehended only in fragments (Figure 1). At the molecular level, calcium channels and neuropeptides, such as calcitonin gene-related peptide (CGRP), play a pathophysiological role. At the biological level, neurogenic inflammation, vascular alterations, mitochondrial dysfunction and hormonal influences are significant. At the cultural level, factors such as stigma, gender dynamics, socioeconomic status and social pressures hold significance (30). In addition, there are often fundamental questions such as the fear of the finiteness of one's own human existence, and many value-philosophical aspects, as discussed above (31).
Since such a complex system cannot be completely reduced causally, it can and must, according to Riedl, only be explained and understood by means of a combination or, at best, a hierarchy of theories (32). Each migraine theory (neurovascular theory, genetic theory, inflammation theory, dysfunctional pain processing, biopsychosocial model, chronification theory, etc.) sheds light on different aspects of migraine. Consequently, only a panoptic, transdisciplinary view can reveal the diversity of migraine, from which a variety of therapeutic consequences can be derived, which can be prioritized and applied in a patient-oriented manner.
How can we meaningfully integrate the various levels of migraine – from molecular mechanisms and biological processes to cultural and other fundamental aspects – into an interdisciplinary dialogue that fosters a holistic understanding?
The philosophical exploration of migraine remains inconclusive. Instead, the Socratic method is intended to foster a lively discourse that comprehensively captures the complex dimensions of the condition. Through deliberate, critical and probing questions, not only scientific and clinical assumptions are challenged, but also connections between biological, psychological, social and cultural perspectives are established. This approach facilitates a deeper and more comprehensive understanding of migraine as a multifaceted phenomenon (Figure 1 and Table 3).
Philosophical discussion of different value systems. The phenomenon of migraine receives its evidence through discussion of the various systems of interpretation; important and concrete questions can be derived from this.

The patient's perception of migraine symptoms in an expanded context.

The Socratic questioning method is intended to foster a lively discourse that comprehensively captures the complex dimensions of a condition, as depicted in Figure 2. Through deliberate, critical and probing questions, not only are scientific and clinical assumptions challenged, but also connections between biological, psychological, social and cultural perspectives are established.

Evaluation and outlook
This review endeavours to illustrate how a transdisciplinary perspective – the integration of insights from the natural sciences, philosophical reflections, and narrative medicine – could lead to a holistic, patient-centered approach in the treatment of migraine. The central guiding principle is: migraine treatment is a human-to-human service. This signifies that migraine should be viewed not as an objectively measurable, neurobiological phenomenon, but rather as a complex, subjective and existential event that is rooted in an individual's biography as well as their social, historical and cultural context.
Integration of knowledge domains and clinical responsibility
Bridging perspectives on migraine illustrates how the integration of knowledge, action, experience, and the search for meaning enables a comprehensive decision-making process (Figure 2). In accompanying the patient, the clinician assumes a central role as a bridge builder between the objective data of the neurosciences and the patient's subjective experience. The clinician's challenging task is to identify and implement – and only implement – those diagnostic and therapeutic measures that are effective, meaningful, appropriate and significant.
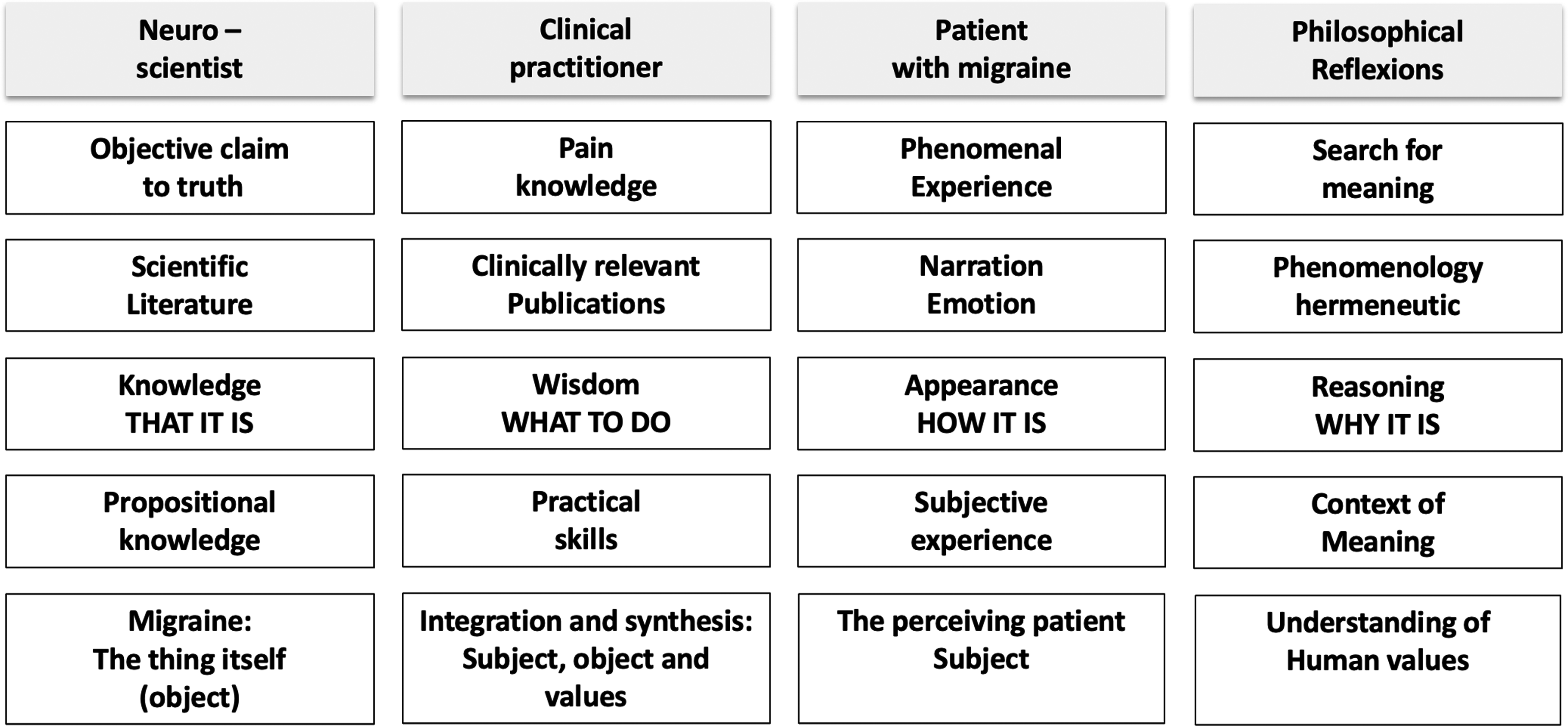
Bridging perspectives on migraine. Neuroscientists see migraine as a neurobiological dysfunction, while patients experience it as a subjective suffering. Clinicians have to mediate between these views, seeking approaches to connect scientific knowledge with the patient's experience.
The advancement of narrative medicine
Emphasizes the essential role of an empathetic dialogue between clinician and patient. This approach – and our recommendation for practical application – focuses not only on the illness itself but also, more importantly, on the patient's individual life story, including their emotions, hopes and concerns related to migraine. As deeply explored by Rita Charon in her influential work Narrative Medicine (33), this method fosters a comprehensive understanding of the biological, psychosocial, biographical, cultural and, crucially, emotional dimensions of the disease.
Narrative medicine offers the opportunity to honour and recognize the patient by attentively listening to their individual story, capturing their subjective experience of migraine in detail – both what is expressed and what remains unsaid. This process of narrative medicine promotes a deeper understanding of the multifaceted nature of migraine, encompassing its biological, psychosocial, biographical, cultural and emotional dimensions.
Promotion of transdisciplinary collaboration and its limitation
An interdisciplinary collaboration involving general practitioners, neurologists, scientists, psychologists, philosophers and other specialists enables a comprehensive understanding of the multifaceted nature of migraine. The objective is to develop a holistic perspective that not only facilitates targeted therapeutic interventions, but also incorporates philosophical considerations and paves the way for further research inquiries.
It is important to note, however, that a comprehensive, holistic evaluation is not always necessary or practicable – especially in cases of acute or chronic migraine where diagnostic clarity and therapeutic efficacy are already established. While psychosocial factors may influence the course of the disease and treatment adherence, they do not invariably constitute the primary focus.
Therefore, a multidisciplinary approach should be implemented in a selective and needs-based manner – particularly when conventional, standardized procedures and interventions prove insufficient, when there are high demands or explicit requests for a more integrated evaluation, or when specific psychological, social and cultural conditions are present that necessitate an interdisciplinary response. Moreover, the substantial time investment and associated costs of a holistic analysis must also be duly considered.
Mixed-methods research and data triangulation
Their potential combination allows for a comprehensive analysis of individual treatment approaches. By systematically linking quantitative and qualitative methods- such as objective measurement data, patient interviews, migraine diaries and clinical findings – and integrating diverse data sources, more precise personalized treatment strategies can be developed while reducing methodological biases.
Socratic questioning in the holistic assessment of migraine
Socratic questioning plays a central role in the holistic evaluation of migraine by fostering critical reflection on individual beliefs, subjective perceptions and emotional responses (4). Furthermore, it opens a philosophical discourse on the nature of suffering and the search for meaning within the patient's lived experience. This approach allows migraine to be understood not merely as a neurobiological phenomenon, but also as a complex, existential experience encompassing psychosocial and cognitive dimensions (Figure 1 and Table 3).
In clinical practice, Socratic questioning facilitates a structured dialogue between patient and clinician, integrating objective findings with subjectively experienced symptoms. This approach helps reconcile seemingly contradictory perspectives between clinical evidence and personal experience. Ultimately, it supports the development of highly individualized diagnostic and therapeutic strategies that are both evidence-based and deeply embedded in the patient's existential and psychosocial context.
From migraine to medicine: the necessity of philosophical reflection
What applies to migraine – namely, that philosophical aspects broaden and deepen our understanding of the condition – can and should be extended to the entire field of medicine. According to Beat Gerber's thesis, medicine remains incomplete without sound philosophical reflection (34). This perspective calls for the adoption of interdisciplinary approaches not solely in the realm of headache disorders, but also across all medical disciplines, thereby contributing to a more comprehensive, patient-centered care strategy.
Conclusions
To summarize, the clinician is always faced with the crucial and challenging task of working with the migraine patient to identify and initiate those diagnostic and therapeutic measures that are effective, meaningful, reasonable and appropriate. To be up to this task, migraine must be understood as a phenomenological, subjective and objective ontological event that raises questions about pain and suffering, consciousness, language and human existence (some practical implications are shown in Figure 3). The experience of migraine headaches pushes the boundaries of what it means to suffer and challenges sufferers to find ways to navigate in a world that may not fully understand or accommodate their pain.

Practical considerations. Both the natural sciences and philosophy contribute significantly to understanding migraine and pain in all its complexity. This has a direct impact on the objective and subjective phenomenology of migraine and consequently on the overall understanding of the patient with migraine to result in a “human-to-human service”. CGRP = calcitonin gene-related peptide.
By carefully combining neurological insights, philosophical thoughts and interdisciplinary perspectives, we can recognize connections and explore their impact on the psychosocial, biographical, spiritual and cultural environment. These connections help create order, meaning and value, guiding optimal, patient-centred treatment. A hermeneutic approach, the art of interpretation, makes it possible to search for a context of meaning not only to explain the pain causally, but also to understand the suffering, this individual challenge in its meaning (35). The philosophical reflections should be understood as an orientation aid to integrate the fragments of individual knowledge into a larger context.
Ultimately, the aim is for us clinicians to accompany the migraine patient in their illness and recovery in a meaningful and thus powerful way. Care and treatment of migraine patients are and remain a “human-to-human service”.
To arrive at a holistic understanding of migraine, philosophical reflections should be understood as an orientation aid to integrate fragments into a larger context Clinicians should accompany the migraine patient in their illness and recovery in a meaningful holistic way. Care and treatment of migraine patients are and remain a “human-to-human service”.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251343225 - Supplemental material for Philosophical aspects of migraine: Headache treatment is a human-to-human service
Supplemental material, sj-docx-1-cep-10.1177_03331024251343225 for Philosophical aspects of migraine: Headache treatment is a human-to-human service by Mark J. Emmenegger and Andreas R. Gantenbein in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.