
Abstract
Objective
To systematically review clinical studies investigating the involvement of adenosine and its receptors in migraine pathophysiology.
Background
Adenosine is a purinergic signaling molecule, clinically used in cardiac imaging during stress tests. Headache is a frequent adverse event after intravenous adenosine administration. Migraine headache relief is reported after intake of adenosine receptor antagonist, caffeine. These findings suggest a possible involvement of adenosine signaling in migraine pathophysiology and its potential as a drug target.
Methods
A search through PubMed and EMBASE was undertaken for clinical studies investigating the role of adenosine and its receptors in migraine, published until September 2021.
Results
A total of 2510 studies were screened by title and abstract. Of these, seven clinical studies were included. The main findings were that adenosine infusion induced headache, and plasma adenosine levels were elevated during ictal compared to interictal periods in migraine patients.
Conclusion
The present systematic review emphasizes a potentially important role of adenosine signaling in migraine pathogenesis. Further randomized and placebo-controlled clinical investigations applying adenosine receptors modulators in migraine patients are needed to further understand the adenosine involvement in migraine.
Introduction
Signaling pathways underlying migraine pathophysiology are complex and may include interplay between several vasoactive amines and peptides released in the trigeminovascular system (1). Adenosine, a by-product of hydrolysis of adenosine monophosphate (AMP) or S-adenosylhomocysteine (SAH) (2), is a vasoactive amine involved in inflammatory response and metabolic stress including hypoxia and ischemic damage (2). Adenosine binds to four G-protein coupled receptors (A1, A2A, A2B and A3 receptors) with a unique profile of tissue distribution, signaling pathways (Figure 1 and 2) and function (Table 1) (3,4). Due to functional diversity, adenosine receptors are therapeutic targets for a wide spectrum of disorders including inflammatory diseases, cancer, myocardial perfusions scintigraphy (3–5) and for termination of paroxysmal supraventricular arrythmias (5). The most common adverse reaction related to adenosine administration is headache (6–8). Similar adverse events were reported upon administration of adenosine reuptake and deaminase inhibitors (9–12). In addition, adenosine receptor antagonist, caffeine, is known to relieve headache (9,13), and is a useful monotherapy against some headache types (14). These observations and the finding that serum adenosine level is elevated during migraine attacks (15,16) indicate a possible implication of adenosine and its receptors in migraine pathophysiology. In this systematic review, we present clinical studies on the role of adenosine signaling pathway in headache and migraine and discuss whether targeting adenosine may represent a novel strategy for the treatment of migraine.

Adenosine signaling pathway through protein kinase A.

Adenosine signaling pathway through protein kinase C.
Adenosine receptors and their functions.

cAMP, cyclic adenosine monophosphate; IP3, inositol 1,4,5-triphosphate; MAPK, mitogen-activated protein kinase; PLC, phospholipase C; PLD, phospholipase D.
Presented molecules targeting adenosine receptors. Only caffeine is currently approved for treatment.

Method
Data source
We searched PubMed and Embase for clinical articles on adenosine in relation to headache and migraine. The search was conducted on 5 September 2021. The first search string was “(“adenosine”[MeSH Terms] OR “adenosine”[All Fields] OR “adenosin”[All Fields] OR “adenosine s”[All Fields] OR “adenosines”[All Fields]) AND (“migrain” [All Fields] OR “migraine disorders”[MeSH Terms] OR (“migraine”[All Fields] AND “disorders”[All Fields]) OR “migraine disorders”[All Fields] OR “migraine”[All Fields] OR “migraines”[All Fields] OR “migraine s”[All Fields] OR “migraineous”[All Fields] OR “migrainers”[All Fields] OR “migrainous”[All Fields])”. The second search string was “(“adenosine”[MeSH Terms] OR “adenosine”[All Fields] OR “adenosin”[All Fields] OR “adenosine s”[All Fields] OR “adenosines”[All Fields]) AND (“headache”[MeSH Terms] OR “headache”[All Fields] OR “headaches”[All Fields] OR “headache s”[All Fields])”.
Selection criteria and study inclusion
Articles were restricted to English language and screened by two investigators (J.T. and L.K.) independently, first by title and abstract and then full text to confirm eligibility for this review. References of the included studies were screened to include studies missed by the search. Any disagreements were resolved through discussion by the two investigators (J.T. and L.K.). If the conflict remained, a third investigator (M.M.K) made the final decision. We included clinical studies investigating the involvement of adenosine, adenosine agonist, adenosine antagonist, adenosine deaminase, adenosine deaminase inhibitor and adenosine reuptake inhibitors in headache and migraine pathophysiology. We excluded reviews, meta-analysis, conference proceedings and case reports. For each included study, aim, method, main outcome, conclusion, and limitations were extracted by two investigators (J.T. and L.K.)
Results
The database search identified 3209 citations of which 701 were duplicates (Figure 3). An additional two studies were included through a manual search of identified primary articles. A total of 2510 studies were screened by title and abstract. Of these, 20 studies were included: 13 preclinical studies and 7 clinical studies (Table 3). Pre-clinical findings are reported in a separate article.

Flow chart of search strategy.
Summary of the clinical studies.
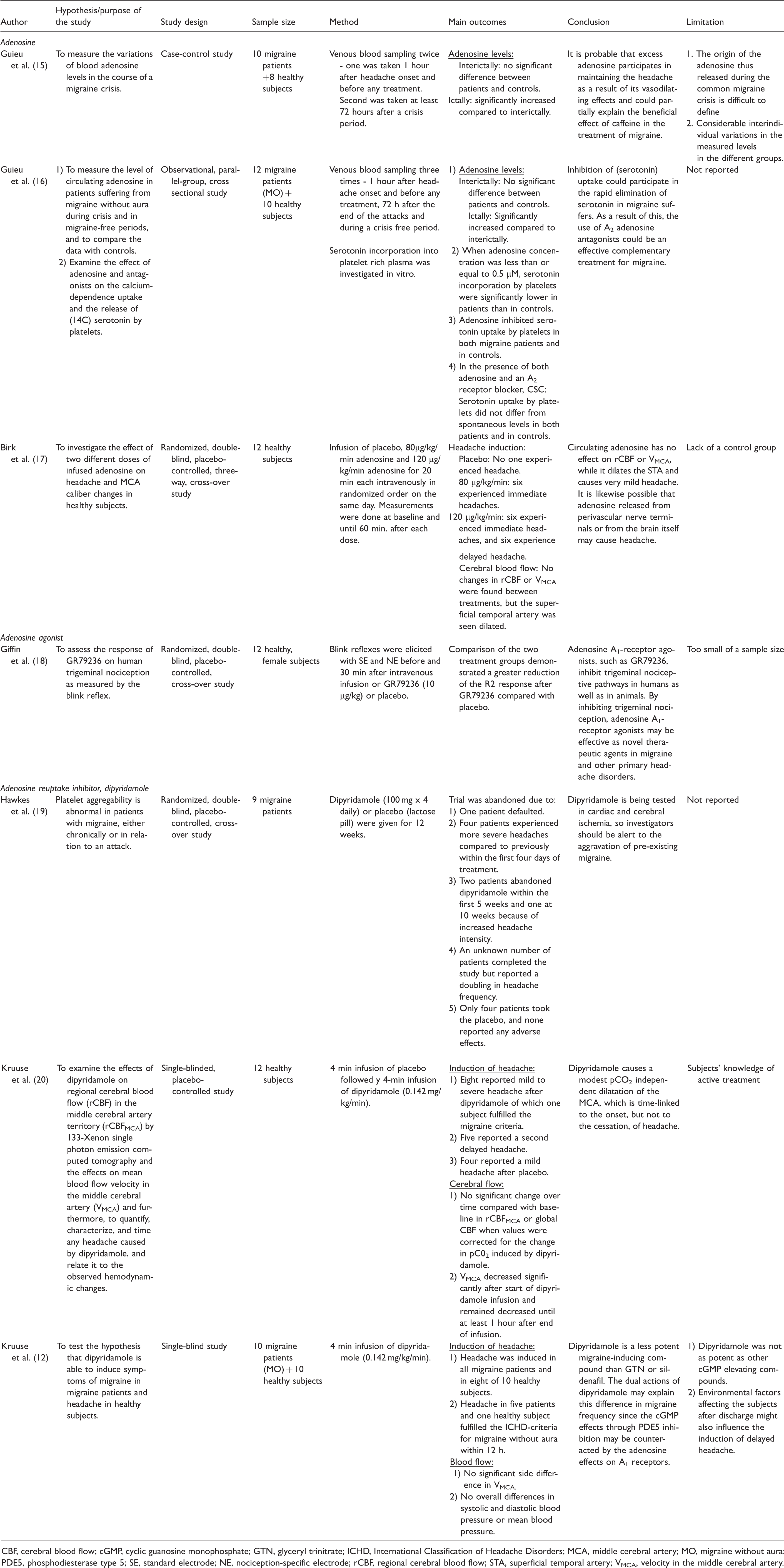
CBF, cerebral blood flow; cGMP, cyclic guanosine monophosphate; GTN, glyceryl trinitrate; ICHD, International Classification of Headache Disorders; MCA, middle cerebral artery; MO, migraine without aura; PDE5, phosphodiesterase type 5; SE, standard electrode; NE, nociception-specific electrode; rCBF, regional cerebral blood flow; STA, superficial temporal artery; VMCA, velocity in the middle cerebral artery.
Narrative Summary
Guieu et al. (15) assessed levels of circulating adenosine in migraine patients and healthy participants. Blood samples were drawn within 1 hour of migraine attack onset and 72 hours following a migraine attack. Adenosine was significantly increased ictally compared to interictally in migraine patients, while no difference was reported between migraine patients (interictally) and healthy controls.
Guieu et al. (16) investigated a possible interaction between adenosine and serotonin in migraine patients and healthy participants. The effect of adenosine and adenosine agonists on the uptake and release of serotonin were assessed in platelet-rich plasma solutions in vitro. Adenosine A2 receptor agonist led to a dose-dependent inhibition of serotonin uptake by platelets in both migraine patients and healthy controls. Furthermore, adenosine was elevated ictally compared to interictally in migraine patients, while no difference was reported between migraine patients (interictally) and healthy controls.
Birk et al. (17) compared intravenous infusion of adenosine over 20 minutes to saline in healthy participants. Single-photon emission computed tomography (SPECT) and transcranial doppler were used to measure regional cerebral blood flow (rCBF) and velocity in the middle cerebral artery (VMCA), respectively. Headache was rated on a verbal scale (1–10). Headache induction and dilation of the superficial temporal artery (STA) was significantly higher after adenosine infusion compared to saline. No difference was observed on rCBF and VMCA between the two study days.
Giffin et al. (18) compared intravenous infusion of adenosine A1-receptor agonist, GR79236 (Table 2), to placebo in healthy female volunteers. Blink reflexes were elicited with standard (SE) and nociception specific electrodes (NE) before and 30 minutes after the infusion (GR79236 or placebo) to evaluate trigeminal nociception. GR79236 partially attenuated the blink reflex when meased by NE. The reduction was significant contralaterally but not ipsilaterally.
Hawkes et al. (19) compared the effect of daily dipyridamole to placebo in migraine patients over 12 weeks. The trial was abandoned, as patients on dipyridamole experienced severe headaches, while no patient on placebo reported any adverse event.
Kruuse et al. (20) compared intravenous infusion of dipyridamole over four minutes to saline in healthy subjects. SPECT and transcranial doppler were used to measure cerebral blood flow and VMCA respectively. Headache was rated on a verbal scale (1–10). Dipyridamole infusion decreased VMCA significantly and caused more headache compared to placebo infusion. No difference was observed in global and region cerebral blood flow between the two study arms.
Kruuse et al. (12) used intravenous infusion of dipyridamole over four minutes in migraine patients and healthy subjects. Transcranial doppler was used to measure VMCA. Headache was rated on a verbal scale (1–10). There was no difference in headache and migraine induction rate between the two study groups. VMCA decreased significantly following dipyridamole infusion and no difference was observed between healthy participants and migraine patients.
Discussion
The present systematic review implicates adenosine and its signaling pathways in the pathophysiology of headache and migraine (Table 3).
Adenosine
Increased adenosine levels during a migraine attack compared to interictally, and to healthy participants suggest that adenosine is involved in triggering and maintaining migraine headache due to its vasodilating properties (15,16). Adenosine levels did not differ between migraine patients interictally compared to healthy volunteers, suggesting that the increase seen during an attack was related to migraine attack as seen with other substances (15,16). It is hypothesized that adenosine is a bi-product to an increase in adenosine triphosphate (ATP) levels during the first few hours of an attack (21). Another explanation is that increased adenosine levels were due to a possible hypoperfusion (16). Finally, it has been proposed that mitochondrial dysfunction causes an increase in extracellular adenosine in migraine patients, which activates AMP-activated protein kinase that affects pain processing (9). It has been difficult to define the origin of adenosine released during an attack (15), and it remains unclear whether the increase appears prior to the headache or secondarily to the migraine attack (16).
Considerable interindividual variations in adenosine levels were reported, possibly due to changes related to circadian rhythm (15,22).
Dipyridamole
Three studies included in the current review concern dipyridamole (12,19,20). Dipyridamole is an adenosine reuptake inhibitor causing accumulation of adenosine. Furthermore, dipyridamole is a phosphodiesterase inhibitor that increases cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP) (23). Clinical studies have shown that substances (e.g. calcitonin gene related peptide, pituitary adenylate cyclase-activation peptide and glyceryl trinitrate) that increase cAMP and cGMP have the potential to induce migraine in migraine patients, implicating them in migraine pathophysiology (1). Presented data suggest that dipyridamole causes headache in healthy volunteers and migraine in patients with migraine (12,19,20). At present, it is unknown whether the headache and migraine induction is a direct result of adenosine elevation, or cAMP and cGMP elevation. Intravenous infusion of dipyridamole increases adenosine and cAMP acutely in humans and rabbits (24,25). In rats, the increase in adenosine was biphasic with an increase during infusion and secondly, 20 minutes after the dipyridamole injection. Meanwhile, cAMP reached its highest level 20 minutes after the injection (25), questioning a direct adenosine mediated headache induction in both studies with intravenous dipyridamole (12,20). Adenosine is also increased following oral administration of dipyridamole over two days (26), which could be the cause of exacerbated headache intensity following daily intake of dipyridamole (19). A study has shown that continuous intake of oral dipyridamole leads to increased headache frequency followed by a decrease in headache frequency, severity and duration (27), The finding was suggested to be related to tolerance to dipyridamole induced headache (27), which questions dipyridamole’s role in the exacerbation of headache intensity (19).
Adenosine receptors as a pharmacological target for migraine
Adenosine has four G-protein coupled receptors (A1, A2A, A2B and A3 receptors) mainly expressed at cerebrum (A1) (5), hippocampus and cerebellum (A1 and A3) (5), pre- and postsynaptic nerve terminals (A2A) (5,28) and some internal organs (A2B) (5). Preclinical studies report expression of adenosine A1 and A2A receptors in the trigeminal ganglion (TG) and trigeminal nucleus caudalis (TNC) in the trigeminal pain pathway (29,30). In contrast to A1 and A3 receptors which are considered to have anti-nociceptive effects, activation of A2A and A2B receptors induces nociception (9) due to different signaling pathways (Table 1, Figure 1 and Figure 2).
The role of adenosine receptors in migraine pathophysiology has previously been questioned due to the effect of caffeine on headache. Caffeine is a non-selective adenosine A1 and A2A antagonist (31) that is used in combination with other analgesics for treating pain including migraine attack (31,32). The analgetic effect is mainly mediated by inhibiting adenosine A2A receptors (32). Caffeine withdrawal can result in caffeine withdrawal headache, and caffeine overuse is a risk factor for migraine chronification, while coffee consumption can be a migraine trigger in some migraine patients (31,33). Interestingly, caffeine overuse upregulates adenosine levels and sudden withdrawal results in increased sensitivity to adenosine, which potentially causes caffeine withdrawal headache (9,34). It is suggested that caffeine may trigger migraine attacks due to dehydration, inhibition of adenosine A1 receptors, which leads to increased nitric oxide and/or decreased magnesium levels (31). Although the effect of caffeine on headache is ambiguous, it is suggested that the role of caffeine in headache is mediated through adenosine A1 and A2A receptors (34).
In human models of pain (trigeminal nociception with blink reflex), GR79236, an adenosine A1 receptors agonist, partially inhibited the trigeminal nociceptive pathway (18). Similarly, adenosine A1 receptors agonist, GR79236 and GR190178, inhibited activation of the trigeminovascular system induced by pain stimuli in cats (35). In rats, electrical stimulation of the TG caused a reduction of adenosine A1 receptors in the TG and TNC (30), while intrathecal administration of adenosine A1 agonist decreased nonevoked pain behavior and evoked mechanical hyperalgesia following surgical paw incision (36). The findings suggest that adenosine A1 receptor agonists plays a role in pain modulation and might be effective for pain management (18,37).
Application of adenosine inhibited serotonin uptake by platelets in vitro. The inhibition was eliminated in the presence of adenosine A2 receptor antagonist, CSC, and therefore adenosine A2 receptor antagonists were suggested as a potential complementary migraine treatment (16). In rats, a highly selective A2A receptor antagonist, SCH58261, blocked adenosine-induced dilation of the middle meningeal artery (38). An increased in adenosine A2A receptors in TG and TNC was seen following electrical stimulation of TG in rats (30) implicating the role of the receptor in pain transmission.
To further implicate adenosine in headache and migraine pathophysiology, a case report described that infusion of regadenoson, a selective adenosine A2A receptor agonist, triggered a hemiplegic migraine attack in a patient with a known history of hemiplegic migraine (39). The attack started eight minutes after start of infusion with left sided numbness and weakness, and after 20 minutes a typical, pulsating migraine headache had followed. The attack subsided within 24 hours. Interestingly, pre-clinical studies suggest that adenosine contributes to cortical spreading depression (40,41).
Limitations and future perspective
The major limitations of studies included were the small sample sizes, the different study designs and that almost half of the studies included investigated dipyridamole which increases adenosine concentration (12,19,20). Only a few studies on headache and migraine inducing abilities of adenosine are currently available (15–19), and no new studies have been conducted in the last 15 years.
A case report showed that adenosine administration triggered migraine attack (42). Furthermore, preclinical studies indicate that accumulation of adenosine and an adenosine A2A receptor haplotype may contribute to migraine aura (40,41,43). These findings should be further investigated in future clinical and pre-clinical studies. To further elucidate the role of adenosine in migraine pathophysiology, investigating the effect of intravenous adenosine infusion in migraine patients and clinically differentiating the receptor subtypes would be of great interest.
Conclusion
In conclusion, adenosine signaling might be involved in migraine pathogenesis, but current knowledge is limited by relatively low level of evidence in clinical studies. Plasma adenosine levels are elevated during migraine attacks (15,16) and administration of adenosine or positive modulators of adenosine signaling pathway induced headache in healthy volunteers and migraine patients (12,17,19,20). Adenosine A1 receptor agonists and adenosine A2 antagonist are potential strategies for future migraine treatments.
Clinical implications
Adenosine is a purinergic signaling molecule involved in a wide range of pathophysiological mechanisms including inflammation. Adenosine infusion induced headache, and endogenous plasma adenosine levels were increased during ictal compared to interictal periods of migraine patients Targeting adenosine A1 and A2 receptors might be a new potential strategy for the treatment of migraine.
Glossary
Footnotes
Declaration of conflicting interests
The authors, JT, LK and MMK, declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. M.A. is a consultant, speaker, or scientific advisor for AbbVie, Amgen, Eli Lilly, Lundbeck, Novartis, and Teva and a primary investigator for ongoing AbbVie, Amgen and Lundbeck trials. M.A. has no ownership interest and does not own stocks of any pharmaceutical company. M.A. serves as associate editor of Cephalalgia, associate editor of the Journal of Headache and Pain, and associate editor of Brain.
Funding
M.A. was supported by the Lundbeck Foundation Professor Grant (R310-2018-3711).