
Abstract
Background/Hypothesis
Mindfulness practice has gained attention in managing chronic migraine with medication overuse headache (CM-MOH), showing clinical improvements and functional connectivity reorganization. However, the relationship between these effects and the underlying neurotransmitter systems remains unexplored.
Methods
Thirty-four CM-MOH patients were divided into treatment as usual (TaU, N = 17) and mindfulness-added-to-TaU (TaU + MIND, N = 17) groups. Participants underwent resting-state fMRI scans before treatment and after one year. We adopted the neurotransmitter-related functional connectivity framework to investigate longitudinal functional changes associated with the distribution of serotonin, dopamine, and norepinephrine systems by comparing TaU + MIND with TaU groups.
Results
When compared with TaU, TaU + MIND patients longitudinally showed increased serotonin-enriched functional connectivity in the caudate and accumbens nuclei, and increased dopamine-enriched functional connectivity in the right insular cortex.
Conclusion/Interpretation
These regions are involved in emotional, cognitive, and sensory modulation of pain and addiction. Our findings suggest the impact of mindfulness practice on serotonin and dopamine systems with potential beneficial effects in chronic pain management.
This is a visual representation of the abstract.
Introduction
Chronic migraine is often associated with medication overuse headache (CM-MOH), a secondary headache characterized by the overuse of acute analgesic medications (1). Its standard treatment typically involves drug withdrawal combined with tailored prophylaxis. Recently, non-pharmacological strategies, such as mindfulness practice, have been attracting growing interest as a way to complement or enhance pharmacological therapies for chronic pain patients. Neuroimaging studies have started to uncover the neurofunctional mechanisms involved in the therapeutic effects of mindfulness on pain perception and modulation (2–4). Notably, a recent study (5) showed that, compared to treatment as usual (TaU) alone, adding on a mindfulness-based treatment (TaU + MIND) in CM-MOH patients led to a greater improvement in headache frequency, medication intake, quality of life, and healthcare costs. These changes are accompanied by a longitudinal functional re-organization of the salience network connectivity with the insular cortex and the sensorimotor face area (6). Such modifications involve brain regions that are altered in CM-MOH patients and are likely entwined with the mechanisms of emotional reappraisal of nociceptive information, self-regulation, non-judgmental acceptance, and body-awareness promoted by mindfulness practice.
Additionally, this practice has also been associated with epigenetic changes of the serotonin transporter (5-HTT) gene (7). Moreover, mindfulness practice alone longitudinally normalizes (i.e., increases at one year from baseline) the plasma levels of catecholamines (i.e., norepinephrine, epinephrine, and dopamine) of CM-MOH patients, similar to those due to pharmacological prophylaxis (8).
Specifically, serotonin, dopamine, and norepinephrine systems are implicated in both the pathophysiology and pharmacological treatment of CM-MOH (9,10), and are also modulated by meditation and mindfulness practices (i.e., increased serotonin and dopamine levels, and reduced norepinephrine levels) (11), suggesting promising opportunities for integrative therapeutic approaches.
However, the relationship between mindfulness-induced functional connectivity (FC) modifications and the brain's underlying neurotransmitter systems has not been systematically investigated yet in CM-MOH patients. Receptor-Enriched Analysis of functional Connectivity by Targets (REACT) (12) is a recent approach that estimates subject-specific FC patterns related to molecular systems using open-source density maps of molecular targets, obtained from healthy subjects PET templates (13). To the best of our knowledge, only one study has adopted this approach to investigate neurotransmitter-related functional abnormalities in a cohort of migraine patients, reporting altered serotoninergic connectivity with respect to controls (14).
In this study, we aim to integrate previous clinical and neurofunctional findings (5,6) investigating one-year longitudinal FC changes associated with key neurotransmitter systems (i.e., serotonin, dopamine, and norepinephrine), using REACT framework, in a cohort of CM-MOH patients, by comparing TaU + MIND with TaU groups. We hypothesize stronger longitudinal neurotransmitter-related FC changes in TaU + MIND patients as compared to TaU patients, since serotonin, dopamine and norepinephrine systems are specifically modulated by mindfulness practice. We also expect TaU + MIND group to show better clinical outcomes after one year.
Methods
Participants
CM-MOH patients, who visited our specialized headache center for a structured withdrawal treatment, were included as part of a previous study (5). The following inclusion and exclusion criteria were considered: diagnosis of CM-MOH (codes 1.3 and 8.2) (1); absence of neurological and severe psychiatric comorbidities, pregnancy, other-than-MOH secondary headaches, withdrawal from MOH twice or more in the last two years, and any previous experience with mindfulness practice. Patients were randomized to TaU and TaU + MIND in a 1:1 ratio, using a computer-generated list (simple randomization). The enrolling and evaluating neurologist (D.D.) remained blind to the allocation; the randomization list was prepared by A.R. Further details are reported in Grazzi et al., (5) and in Fedeli et al., (6). The study was approved by the local Ethical Committee of Neurological Institute C. Besta (approval 51/2018).
Interventions
The TaU protocol involved withdrawing overused symptomatic medications, tailored prophylaxis (i.e., antidepressants or neuromodulators), and education on medication usage and healthy lifestyle. The TaU + MIND protocol included TaU with the add-on of six 90-min-long weekly guided sessions of mindfulness-based intervention. These sessions were followed by daily home self-practice guided by a 12-min audio file for the entire year. All patients underwent both a clinical evaluation and MRI scan at enrolment (T0) and after one year of treatment (T1). A full description of the TaU and TaU + MIND clinical protocols is reported in detail in the Online Supplementary Materials and in Grazzi and colleagues (5).
MRI acquisition
Subjects underwent an MRI scan using a 3T Philips Achieva scanner. The imaging protocol included a high-resolution 3D T1-weighted image (TR = 8.11 s; TE = 3.71 ms; FOV = 240 × 240 mm; voxel size = 1 × 1 × 1 mm3; flip angle = 8°; 185 sagittal slices) and a resting-state fMRI scan (15 min, eyes-opened; T2*-weighted BOLD echo-planar imaging gradient-echo sequence; Repetition Time [TR] = 2000 ms; Echo Time [TE] = 30 ms; Field-of-View [FOV] = 80 × 80 mm; voxel size = 3 × 3 × 3.2 mm3; interslice gap = 0.4 mm; flip angle = 80°; 34 axial slices; 450 volumes; Phase Encoding direction = posterior/anterior). All patients were in interictal migraine phase at the time of MRI acquisition.
Preprocessing of MRI functional data
Resting-state fMRI data were analyzed using the CONN toolbox (https://web.conn-toolbox.org/; v. 20.b; running in Matlab 2020b) with the “Default-MNI” preprocessing pipeline (slice timing correction, realignment, coregistration, spatial smoothing = 6 mm3), denoised with aCompCor method, and bandpass-filtered (0.008–0.1 Hz).
Neurotransmitter-related functional connectivity analysis
For each patient and each session, preprocessed resting-state fMRI data were used to estimate neurotransmitter-related FC maps using REACT-fMRI toolbox (https://github.com/ottaviadipasquale/react-fmri)12. REACT uses a two-step regression analysis (i.e., dual regression) to estimate subject-specific FC maps informed by neurotransmitters distribution using open-source molecular templates obtained from healthy subject PET scans. For each neurotransmitter of interest (i.e., serotonin, dopamine, and norepinephrine) molecular templates were used as reference maps (13). The serotonin atlas included maps of 5-HT1a, 5-HT1b, 5-HT2a, 5-HT4 receptors, and the 5-HT transporter (5-HTT). The dopamine atlas included maps of D1 and D2 receptors, and the dopamine transporter (DAT). The norepinephrine atlas included only the norepinephrine transporter (NET). The cerebellum was removed from the serotonin atlas and the D1 and D2 templates, while the occipital cortex was removed from the DAT and NET maps as they were used as reference regions in radioligands kinetic models (12). In addition, since endogenous opioid and endocannabinoid systems are involved in pain modulation, neurotransmitter-related FC maps were investigated also in these neurotransmitter systems. The opioid atlas included a map of μ-opioid receptors (MOR). The endocannabinoid atlas included a map of cannabinoid receptor 1 (CB1). The occipital cortex was removed from the MOR map as it was used as reference regions in radioligands kinetic models. No reference regions were removed from CB1 map (13). Then, intensity values of subject-specific neurotransmitter-related FC maps were normalized (values ranging from 0 to 1) and constrained with a MNI gray matter binary mask (12) provided within the REACT toolbox. Between-group neurotransmitter-related FC differences were assessed at the baseline (TaU + MIND T0 vs. TaU T0). Then, longitudinal neurotransmitter-related FC maps were generated for each subject and each neurotransmitter of interest by subtracting T0 maps from the same map obtained at T1. Longitudinal neurotransmitter-related FC maps were entered into a second-level general linear model using SPM12 (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/) to investigate differences between TaU and TaU + MIND patients, considering age, sex assigned at birth, and assigned prophylaxis (i.e., antidepressants or neuromodulators) as covariates. Results were thresholded with a p < .001 uncorrected at the voxel level and Family-wise Error Rate (FWE) corrected for multiple comparisons at p < .05 at the cluster level. Moreover, correlations between longitudinal neurotransmitter-related FC changes and improvements in clinical variables (i.e., monthly headache days - 3 months; monthly doses of acute drug intake – 3 months; state and trait anxiety; depression; allodynia; trait mindfulness; see Fedeli et al., (6)) were performed separately for each group.
Results
Participants
Thirty-four (N = 34) CM-MOH patients, attending our specialty headache center for a structured withdrawal treatment, participated in the present study and have also been reported in previous work (5,6). Participants were randomly assigned to TaU group (N = 17), and TaU + MIND group (N = 17). The two groups were comparable for demographic and clinical variables (see Table 1). Both groups improved in clinical variables at the follow-up (see Online Supplementary Table 1). Longitudinal between-group comparisons in clinical changes showed a greater improvement in TaU + MIND patients compared to TaU patients for the monthly headache days (see Online Supplementary Table 1).
Clinical and demographic data.
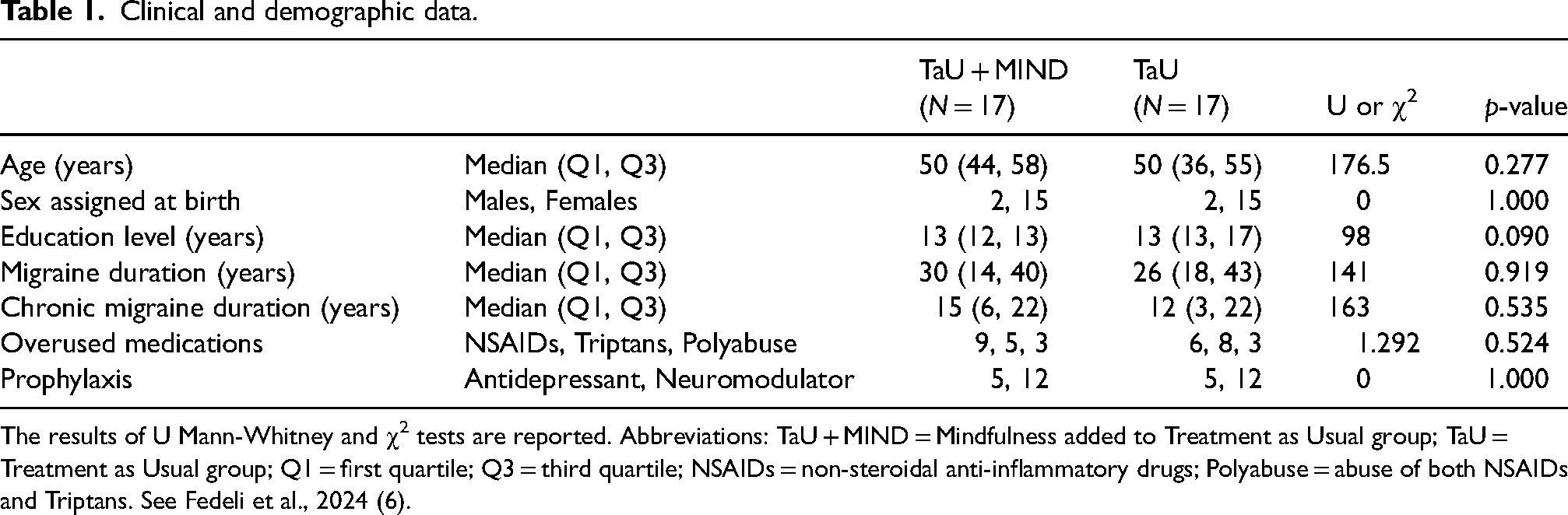
The results of U Mann-Whitney and χ2 tests are reported. Abbreviations: TaU + MIND = Mindfulness added to Treatment as Usual group; TaU = Treatment as Usual group; Q1 = first quartile; Q3 = third quartile; NSAIDs = non-steroidal anti-inflammatory drugs; Polyabuse = abuse of both NSAIDs and Triptans. See Fedeli et al., 2024 (6).
Neurotransmitter-related functional connectivity analysis
At T0, no differences were found between TaU + MIND and TaU groups in the serotonin, dopamine and norepinephrine systems, ensuring that the longitudinal results reflect treatment differences rather than pre-existing group effects.
Longitudinally, between-group differences were observed in neurotransmitter-related FC patterns associated to serotonin and dopamine systems, while no significant changes were found in the norepinephrine circuit. In addition, no results were reported in opioid and endocannabinoid systems (see Online Supplementary Materials). In the serotonin system, enhanced connectivity in the right (5-HT1b receptor) (Figure 1a, Table 2) and bilateral (5-HTT transporter) caudate and accumbens nuclei (Figure 1b, Table 2) was observed in TaU + MIND patients when compared with TaU patients. In the dopaminergic system, TaU + MIND group compared with TaU group showed increased longitudinal neurotransmitter-related FC in the right insular cortex (D1 receptor and DAT transporter; Figure 1c and d, Table 2). All results are detailed in Table 2 and Figure 1. Unthresholded z-maps and significant cluster masks are available at Neurovault (https://identifiers.org/neurovault.collection:17391). No significant correlations between longitudinal neurotransmitter-related FC changes and improvement in clinical variables were observed.

Longitudinal neurotransmitter-related functional connectivity results. Significant between-group (TaU + MIND > TaU) longitudinal differences are reported for 5-HT 1b serotonin receptor (a), 5-HTT serotonin transporter (b), D1 dopamine receptor (c), and DAT dopamine transporter (d). Results are corrected at p-FWE < 0.05 at the cluster level and p < 0.001 uncorrected at the voxel level. MNI coordinates of axial slices are reported (z). Significant subcortical clusters are reported as solid color volumes in 3D subcortical meshes. Significant cortical clusters are reported as semi-inflated 3D brain surface meshes. Abbreviations: L = left hemisphere; R = right hemisphere; T = t-values (degrees-of-freedom); CN = caudate nucleus; NAcc = nucleus accumbens.
Neurotransmitter-related functional connectivity longitudinal comparisons results.

TaU + MIND = mindfulness added to treatment as usual group; TaU = treatment as usual group; Δ = longitudinal change (T1–T0); Hem. = Hemisphere; R = Right; FWE = Family wise Error Corrected for multiple comparisons; k = cluster size in mm3; Unc. = uncorrected for multiple comparisons; MNI = Montréal Neurological Institute spatial coordinates; 95% CI = 95% Confidence Interval. Region atlas labeling was performed with the Harvard-Oxford atlas.
Discussion
Our findings showed significant longitudinal increases in serotonin-enriched FC in the caudate nuclei extending to the accumbens nuclei, and dopamine-enriched FC in the right insular cortex for the TaU + MIND compared to TaU group.
With respect to serotonin, the caudate and accumbens nuclei are dense in 5-HT receptors (15). Alterations (i.e., decreased levels of platelet serotonin, suggesting a suppression of 5-HT function) in the serotonin system in CM-MOH have been associated with cortical hyperexcitation, trigeminal nociceptors sensitization, migraine chronification, and pain perception facilitation (10). On these grounds, our results seem to suggest a normalization of the 5-HT system after mindfulness treatment in TaU + MIND patients. Moreover, alterations in caudate FC with regions integrating emotional and cognitive aspects of pain and involved in sensory pain modulation and suppression have been reported in literature on CM-MOH patients (16). Additionally, the accumbens nucleus is involved in reward processing and in the formation of behavioral habits (17). Therefore, these findings might suggest that mindfulness-related FC remodulation could help in breaking the pain-pill cycle of medication reliance, overuse, and dependency, facilitating more adaptive responses to pain.
Concerning the dopamine system, the insular cortex is rich in the expression of D1 receptors (18). Our dopamine-enriched FC findings in this region provide a new insight into the underlying mechanism of our previous observation of FC reorganization between salience network and the insula in TaU + MIND patients (6). As insular cortex emotionally processes painful information (19) and plays a pivotal role in pain chronification (20), our result points towards the emotional reappraisal and acceptance of painful experience (rather than reacting or avoiding). This could potentially modulate the “suffering” component associated with painful states (21). Moreover, dopamine transmission is involved in the modulation of addictive behavior and drug withdrawal mechanisms (18), and previous evidence showed normalized dopamine levels in blood samples in another cohort of CM-MOH patients after one year of mindfulness practice (8). In line with these observations, our results indicate a possible impact of mindfulness practice on specific regions of the dopaminergic system which play a key role in medication overuse in these patients.
Taken together, the longitudinal changes in neurotransmitter-enriched FC suggest that mindfulness practice could influence multidimensional aspects of pain processing and medication overuse, by regulating the activity of regions involved in serotonin and dopamine systems of CM-MOH patients (11).
Nevertheless, our findings should be considered in light of some limitations. First, since REACT uses healthy participants open-source templates, this approach is not equivalent to a subject-specific PET scan. However, neurotransmitter-related FC still represents a promising non-invasive tool to investigate the still largely unexplored relationship between FC and the brain's neurotransmitter systems (22). Second, data on subjective pain were not considered in our analyses since patients claimed to be attack-free at the moment of MRI acquisition. Third, despite the longitudinal design, our study is limited in sample size. Therefore, we cannot exclude that changes in the norepinephrine system or other systems involved in pain modulation might emerge with larger samples. Thus, we invite the readers to consider our results with caution.
In conclusion, our study provides evidence that mindfulness practice could modulate dopamine and serotonin-enriched FC in key brain regions involved in pain processing, addictive behavior, reward processes, and emotional regulation. While preliminary, these results highlight the relevance of mindfulness practice as a non-pharmacological approach that could be added to pharmacological treatment in chronic pain management.
Clinical implications
Mindfulness longitudinally modulates serotonin- and dopamine-enriched functional connectivity in the caudate and accumbens nuclei, and in the insular cortex, respectively.
These regions are involved in pain processing, addiction, and emotional regulation in chronic migraine with medication overuse headache.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251332561 - Supplemental material for Neurotransmitter-related functional connectivity changes in serotonin and dopamine systems after mindfulness in medication overuse headache
Supplemental material, sj-docx-1-cep-10.1177_03331024251332561 for Neurotransmitter-related functional connectivity changes in serotonin and dopamine systems after mindfulness in medication overuse headache by Davide Fedeli, Giuseppe Ciullo, Greta Demichelis, Jean Paul Medina Carrion, Maria Grazia Bruzzone, Emilio Ciusani, Alessandra Erbetta, Stefania Ferraro, Marina Grisoli, Erika Guastafierro, Danilo Antonio Montisano, Domenico D’Amico, Alberto Raggi, Anna Nigri and Licia Grazzi in Cephalalgia
Footnotes
Acknowledgments
We would like to thank our participants for generously taking part in this research. The Authors are grateful to the GARR consortium for the high-performance infrastructure used for the analyses at Neuroradiology Department of Fondazione IRCCS Istituto Neurologico Carlo Besta (Milan, Italy).
Availability of data and materials
Authors’ contributions
LG, DD, and AR conceived and designed the study; AR, LG, DD performed patient recruitment, randomization and data curation; DD, LG performed patient clinical evaluation; LG conducted mindfulness sessions; AN, GD, JPMC, SF, DF, and GC contributed to neuroimaging data collection and curation; AE performed neuroimaging data clinical assessment; DF, GC, and JPMC performed statistical and neuroimaging data analyses; DF, GC, AN, and GD drafted the manuscript; MGB, EC, AE, SF, MG, EG, DAM, DD, AR, and LG conducted a rigorous review of the manuscript and provided critical feedback; LG, DD, AR, AN, and MGB, contributed to funding acquisition; MGB and MG provided MRI facility resources; AR, AN, LG, MGB supervised the project.
All authors contributed toward the revision and writing of the final draft and approved the final version of the manuscript before submission. AN performed manuscript submission and author correspondence.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministero della Salute (grant number RF-2016-02364801, RRC), NextGenerationEU (NRRP Mission 4 Component 2 Investment 3.3 Call for tender No. 117 of 02/03/2023), Key Research and Development Projects of Sichuan Province (M112022YFWZ0003).
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Fondazione IRCCS Istituto Neurologico Carlo Besta (approval no. 51/2018). The participants provided informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.