
Abstract
Background
Orthostatic headache (OH) is a common feature of various conditions, including spontaneous intracranial hypotension (SIH), but no precise definition currently exists outlining the typical OH characteristics. This ambiguity risks misdiagnosis with unnecessary investigations and delay in institution of treatment. The present study aimed to carry out structured phenotyping of OH in patients with SIH with the aim of outlining its typical characteristics.
Methods
Eligible patients with clinico-radiological confirmed SIH underwent a structured interview, after which a specialist interest group utilised the modified Delphi process to analyse the data and achieve consensus on defining the typical characteristics of OH in SIH.
Results
In total, 137 patients were recruited. OH was present in 75.9%. Typical OH characteristics in SIH were defined as having a baseline severity (lying flat) on waking up of ≤3 (0–10, verbal response scale), headache onset-time of ≤4.5 h on becoming upright, time to peak severity of ≤7.5 h and an offset to baseline severity within 1.5 h of recumbency. Intra-individual consistency in the onset and offset-time was deemed a necessary characteristic.
Conclusions
Defining typical OH characteristics has the potential of enhancing SIH diagnostics and management, at the same time as minimising unwarranted invasive procedures.
This is a visual representation of the abstract.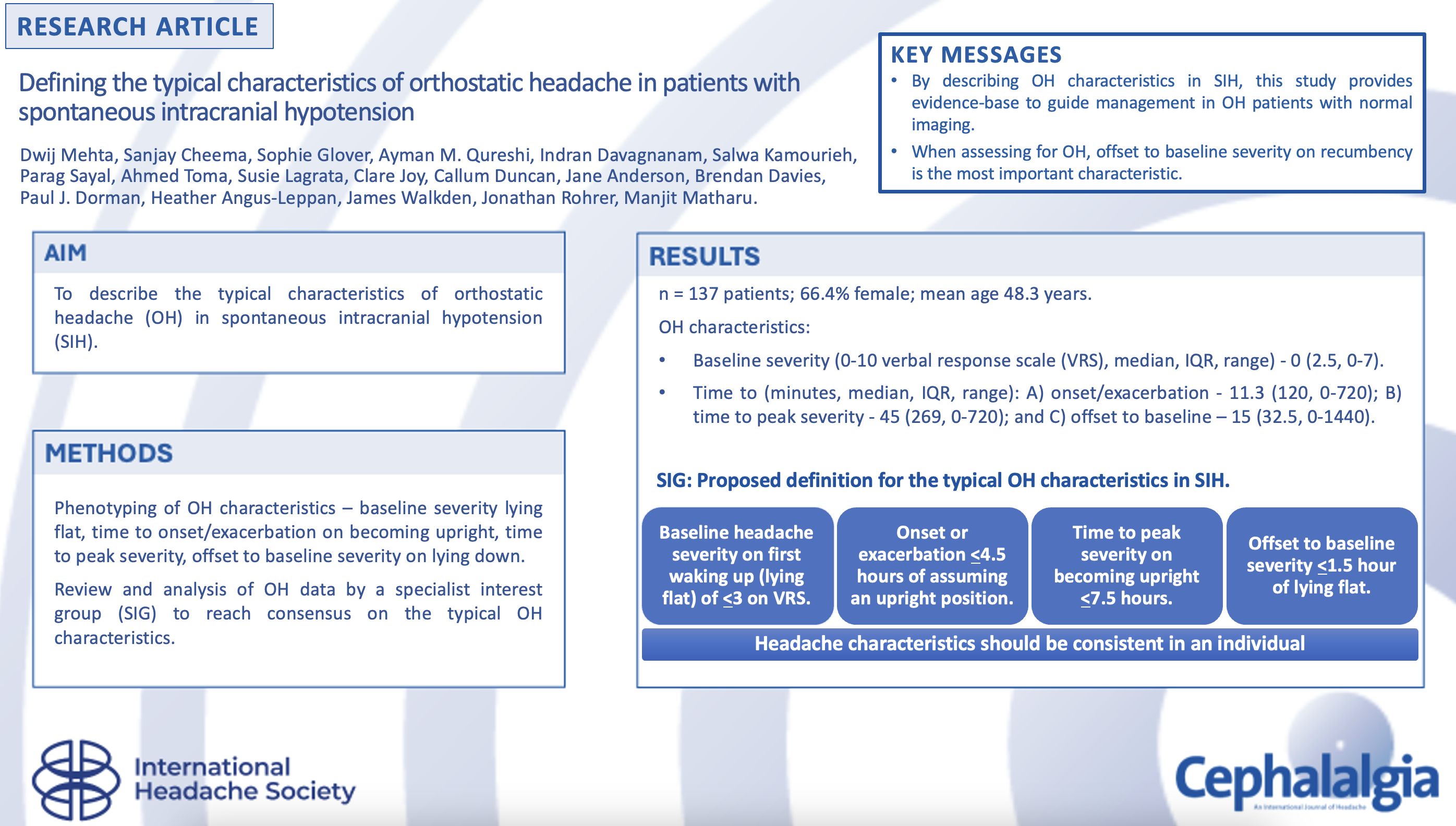
Keywords
Introduction
Background
Headaches described as “orthostatic” typically refer to those that are exacerbated, or triggered, by assumption of an upright posture, and alleviated by recumbency. Orthostatic headache (OH) is a hallmark feature of some of the most disabling neurological conditions commonly affecting a young population in the form of spontaneous intracranial hypotension (SIH) and postural tachcyardia syndrome (PoTS); other important differentials for OH include cervical pathology and migraine (1,2). It frequently necessitates prolonged bedrest with subsequent impact on the patient's level of independence, financial status, interpersonal relationships and mental wellbeing (3).
Despite OH being reported in over 96% of SIH patients, no detailed phenotyping studies reviewing the typical OH characteristics, or, more broadly, attempting to define what constitutes a typical OH in SIH exist (4). In clinical practice, there is often a great degree of variation in the onset and offset-times of the headache in relation to change in posture. Specifically, there is no consenus, or an evidence-base, for maximum permissible duration for the headache to start or worsen on becoming upright, the maximum time for return to baseline on lying down, whether the continuance of a mild persistent headache when lying down is acceptable, and whether there are any distinct phenotypic characteristics and symptoms specific to OH in SIH.
A review of available literature highlights the uncertainty surrounding OH. Diagnostic criteria for headache associated with SIH in the International Classification of Headache Disorders, 2nd edn (ICHD-2) required the headache to worsen within 15 minutes of being upright (5); however, this requirement was removed in ICHD-3. This was changed to a broader, less precise, description in ICHD-3 where headache can worsen and ameliorate within seconds to even hours after a change in vertical position, reflecting the variability that is commonly encountered in clinical practice, as well as the absence of detailed OH phenotyping studies in the literature to guide the description (6).
Interestingly, some patients with SIH are recognised as having second-half-of the-day (SHOD) headaches and this is distinguished from the more typical OH based on the delayed time of onset after being upright (7,8). Despite this common clinical differentiation from OH, there is no established timeframe for when a headache transitions from being orthostatic to being classified as a SHOD headache. Considering that these headaches are also triggered by sustained upright activity and alleviated by lying down, it poses the question of whether SHOD headaches are simply a delayed-onset subtype of OH.
The paucity of research in the field also leaves a gap in our knowledge about whether distinct headache characteristics, and/or accompanying symptoms, can accurately distinguish between the various causes of OH. Identification of these potential differences can play a critical role in helping a clinician instigate early and targeted management for their patients presenting with OH, particularly in the context of a normal magnetic resonance imaging (MRI) of brain and spine, ensuring timely identification of cerebrospinal fluid (CSF) leaks, while limiting unnecessary, expensive, and frequently invasive procedures, such as epidural blood patches (EBPs) and myelograms, in those without a leak.
Despite the frequent utilisation of EBPs in spinal CSF leaks, they are not without potential risks. Common side-effects include transient backache, radicular symptoms and neck pain lasting up to a few weeks. More serious complications include, but are not limited to, spinal arachnoiditis, spinal haematoma, cauda equina syndrome and infection (9). Similarly, myelograms can lead to a postdural puncture CSF leak, spinal cord or conus injury, and more rarely an allergic reaction to iodinated contrast (10). With digital subtraction myelograms, there are added risks relating to use of general anaesthetic, when utilised. Thus, careful consideration is required, particularly in the management of OH cohort with normal MRI; better appreciation of the typical OH characteristics in SIH will aid the decision-making process.
From the academic viewpoint, lack of consensus on what constitutes a typical OH in SIH translates to reporting of heterogeneous and non-comparable data, and thus hampering efforts to further our understanding in SIH.
To the best of our knowledge, the present study is the first phenotyping study to propose an objective working-definition for the typical OH characteristics observed in patients with SIH.
Objectives
To delineate the clinical phenotype of OH in patients with SIH, with the aim of developing a working definition for its typical characteristics.
Methods
Study design
An observational cohort study of patients with SIH using prospectively collected clinical and radiological data.
Participants
We included consecutive patients with a diagnosis of SIH corroborated by typical MRI findings, seen at a tertiary-referral headache clinic by a single multidisciplinary team at The National Hospital for Neurology and Neurosurgery, London, UK between 2008 and 2024.
Inclusion criteria for the study required patient to have current neuroimaging consistent with SIH, with or without current symptoms, or an ongoing clinical syndrome suggestive of SIH with past radiological evidence of SIH. In accordance with recent UK-based consensus guidelines on diagnosis and management of SIH, opening pressure was not routinely measured when diagnosing SIH due to the recognition that pressures are frequently normal, or even raised, and lumbar punctures risk exacerbating the symptoms through a post-dural puncture leak (11).
Clinical features deemed compatible with SIH, present in isolation or in combination, included OH, Valsalva-induced headaches, exercise-induced headache and frontotemporal brain sagging syndrome (FBSS) (1,4,8,12).
MRI features considered typical for SIH included at least one of: diffuse smooth pachymeningeal enhancement, subdural collections (SDC), brain sagging, the venous distension sign and spinal epidural fluid collection (4,12,13). This was assessed by two experienced consultant neuroradiologists with an interest in CSF leak. Although enlargement of the pituitary gland is a well-recognised radiological feature of SIH, it was not included in isolation because this is a relatively common incidental finding in the normal population.
Exclusion criteria were age under 18 years, history of a craniospinal procedure within the preceding month of symptom-onset, and patients with clinically and radiologically resolved SIH at time of presentation. Patients were also excluded if they were unable to provide a clinical history.
Patient assessment
All patients had a structured assessment for clinical features, response to treatments, and risk factors of SIH.
When present, headaches were categorised into orthostatic and non-orthostatic types. In absence of an evidence-base differentiating OH and SHOD, headaches with a consistent onset or exacerbation on assumption of an upright position, and improvement or resolution with recumbency, were labelled as being orthostatic. Non-orthostatic headaches were further subclassified into categories, including tension-type headache, new daily persistent headache (NDPH), Valsalva-triggered headaches and those with migraine-like features. For those with OH, data on the headache severity upon awakening while still recumbent, the latency to headache-onset, or worsening, on assuming an upright position, the duration to reach peak severity when upright and the time taken to return to baseline severity on lying down, were collected. Headache severity was rated between 0–10 using the verbal response scale (VRS). When provided with a range for timings or severity scores, the mean value was used.
We also recorded the headache location, lateralisation, pain quality, and associated non-headache symptoms (Table 1). Retrospective review of headache-type at onset, when present, was also performed.
Data fields for headache and associated symptoms.

Abbreviation: VRS = verbal response scale.
Data analysis
Patients were stratified based on their headache phenotype (orthostatic or non-orthostatic), and the duration of their symptoms at time of clinic review.
For the duration of the condition (Table 2), categories of acute (≤10 weeks), subacute (11–52 weeks) and chronic (>52 weeks) were used in keeping with previous literature to allow meaningful comparisons (14).
Changing headache presentation in SIH with increasing chronicity of symptoms.
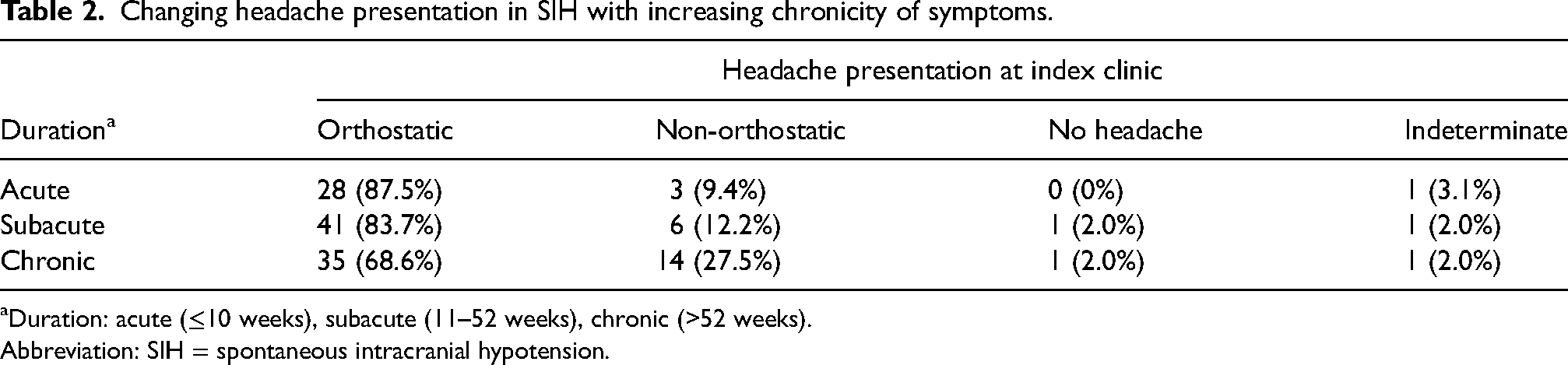
Duration: acute (≤10 weeks), subacute (11–52 weeks), chronic (>52 weeks).
Abbreviation: SIH = spontaneous intracranial hypotension.
A specialist interest group (SIG), which was composed of five neurologists, three neurosurgeons, one senior headache nurse specialist and a SIH patient representative from the CSF Leak Association charity, was convened.
The SIG formulated and addressed the following questions:
Which orthostatic characteristic is the most important when defining the typical OH in SIH? Rank the aforementioned orthostatic characteristics from most to least important when defining the typical OH in SIH. Which centile values represents the best working definition for typical OH characteristics in SIH? Should consistency in time of onset and offset of headache with change in vertical posture be part of the proposed definition?
Employing a modified Delphi process, the SIG analysed and debated the data, formulating responses. These proposals were voted on anonymously; those failing to secure a 70% consensus initially were re-discussed, revised and voted upon again until this threshold was met.
Statistical analysis
Statistical analysis of the clinical data was performed using SPSS, version 28 (IBM Corp., Armonk, NY, USA) and Excel (Microsoft Corp., Redmond, WA, USA). Normality assumptions were based on visual inspection of histograms and Kolmogorov–Smirnov test. Missing data were not imputed. Descriptive data were summarised as the mean ± SD, or medians with interquartile range (IQR), and range depending on the distribution of data. For categorical variables, chi-squared or Fisher’s exact test were used. A Mann–Whitney U-test was used for the analysis of non-paramaetric continuous variables. Spearman's rank correlation was employed to assess the relationship between disease duration and OH characteristics. p < 0.05 (two-tailed) was considered statitically significant.
Results
Participants
We identified 144 patients with SIH. Seven patients were excluded from the study: two with severe FBSS preventing a reliable history; four could not provide onset and offset times for their postural headaches; and one died from an unrelated cause. Of the remaining 137 patients, 91 (66.4%) were female. Mean ± SD age was 48.3 ± 12.0 years (range 19–79 years). Presentation to the clinic was in the acute stage in 23.4%, subacute in 35.8% and chronic in 37.2%. Onset time was indeterminate in five patients due to either incidental radiological finding of SIH, or an insidious non-orthostatic headache presentation. The median duration between onset of symptoms and the index clinic assessment was 32.6 weeks (IQR = 121.8 weeks, range 1333 weeks).
Diagnosis of a coexisting headache disorder, which included migraine, tension-type headache and cluster headache, was present in 40.9%. History of joint hypermobility was present in 13.9%. A prior history ≥1 EBP was present in 38% of patients at time of clinic review; median number of EBP pre-assessment was 0 (IQR = 1, range = 6). Complication of cerebral venous sinus thrombosis (CVST) was documented in three patients, while SDC on MRI was observed in 45.3%.
Headache types
At presentation in clinic, OH was the commonest type, being present in 75.9%, followed by non-orthostatic headache in 19.7%, and no headaches at time of clinic review in 2.2%. In another three patients, it was not possible to reliably categorise the headache-type (reported as “indeterminate”). In four of the five patients without a defined onset time, the headache was non-orthostatic at the time of clinic evaluation. Non-orthostatic headache presentations are summarised in Table 3. Incidence of OH did not significantly differ between patients with a history of EBP and those without (p = .544).
Non-orthostatic headache presentations at time of review in clinic.
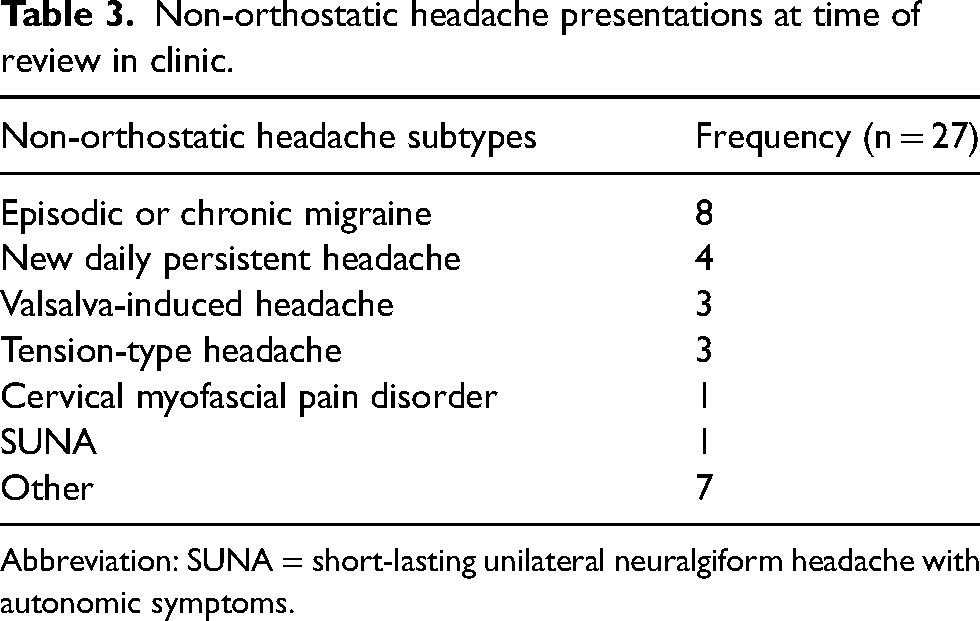
Abbreviation: SUNA = short-lasting unilateral neuralgiform headache with autonomic symptoms.
At onset of SIH, OH remained the commonest headache-type (82.5%). This was followed by Valsalva-induced (8.0%), NDPH (7.3%), exercise-induced (1.5%), paradoxical headache consistent with intracranial hypertension (0.7%) and other non-specific headaches (3.6%). It was not possible to reliably determine the headache type at onset in two patients (1.5%), while in 3.6% of the cohort, main presentation was either related to non-headache symptoms, or SIH was diagnosed incidentally. Two patients had a thunderclap onset.
Orthostatic headaches
There was no statistical difference (p = 0.071) in the frequency of OH across the disease-duration categories (Table 2). Headaches were bilateral in 88.5%, unilateral in 6.7% and either unilateral or bilateral in 4.8%. Occipital region was most frequently affected (Table 4), while neck pain was present in 76%. Most common headache quality was throbbing (Table 4) and headache was exacerbated by Valsalva manoeuvres in 69.2%.
Orthostatic headache quality and location.

Patients were frequently headache-free on first waking up when lying flat and had a rapid onset and offset of the headache within minutes (Table 5) with change in posture. Table 6 highlights the centile-specific values for the OH characteristics.
Orthostatic headache characteristics.

Abbreviations: IQR = interquartile range; VRS = verbal response scale.
Centile values for orthostatic headache characteristics.

Abbreviation: VRS = verbal response scale.
A Mann–Whitney U-test showed a significant difference (U = 933.0, p = 0.024) between the time to peak severity for cohort with history of previous EBP compared to those without. The median time to peak severity for the EBP cohort was 135 minutes compared to 17.5 minutes for those without a history of EBP, suggesting that previous EBP is associated with an increased time to peak severity.
The frequency of OH in patients with and without SDC was 75.8 and 76% (p = .979), respectively. Mann-Whitney U testing revealed no statistically significant differences between these groups regarding baseline severity (U = 1499.5, p = 0.271), time to onset/exacerbation (U = 1350.5, p = 0.692), time to peak severity (U = 732.5, p = 0.661), peak severity (U = 1237.0, p = 0.827) and offset to baseline severity (U = 1173.5, p = 0.917).
Similar comparison for potential differences in OH characteristics was also made between patients with and without history of migraine. Again, no statistically significant difference was observed on Mann–Whitney U-test for baseline severity (U = 1450.5, p = 0.093), time to onset/exacerbation (U = 1130.5, p = 0.682), time to peak severity (U = 701.0, p = 0.992), peak severity (U = 1061.0, p = 0.438) and offset to baseline severity (U = 1184.0, p = 0.544) between the groups.
On Spearman's correlation, a weakly positive correlation between the disease duration and the time to headache onset (rs = 0.212, n = 102, p = 0.032), time to peak severity (rs = 0.322, n = 79, p = 0.004) and offset time (rs = 0.236, n = 98, p = 0.019) was noted.
To investigate potential differences in offset duration for patients with notably prolonged onset times, we reviewed data for those with onset/exacerbation time in ≥85th centile. The median offset time to baseline severity was 30 minutes for this group compared to 15 minutes for the rest of the cohort (U = 741.0, p = 0.241).
Associated symptoms are shown in Table 7. Besides phonophobia and muffled hearing, which were more common in the OH cohort compared to those without, no other significant differences were observed in the frequency of associated symptoms between the two groups.
Frequency of non-headache symptoms in the overall SIH cohort compared to those with current orthostatic headaches.

*Comparing patients with orthostatic headache to those without.
Abbreviation: SIH = spontaneous intracranial hypotension.
Specialist interest group
Following the modified Delphi consensus process by the SIG, there was strong consensus on the following points (proportion of votes in brackets):
The time to headache resolution or return to baseline on lying flat is the most important when defining typical OH characteristics (90%). The orthostatic characteristics, in descending order of importance, are: offset-time to baseline severity, latency to onset or worsening, time to peak severity and baseline headache severity when lying flat. Peak headache severity was deemed to be the least informative and distinguishing feature. The 85th centile values provide the best working definition for typical OH characteristics in SIH; balancing the need for the definition to reflect the vast majority of OH cohort in SIH without being excessively inclusive as to lose its specificity (70%). Consistency in the onset- and offset-times is required as part of the definition (100%).
Proposed definition for the typical OH characteristics in SIH
Typical OH in SIH is characterised by a postural headache that has a baseline headache severity on first waking up (lying flat) of ≤3 on VRS, has an onset/exacerbation ≤4.5 hours of assuming an upright position, time to peak severity on becoming upright ≤7.5 hours and an offset to baseline severity ≤1.5 hours of lying flat. These headache characteristics should be consistent in an individual patient.
Discussion
Currently, no detailed phenotyping study in SIH outlining the typical OH characteristics exist. Recent publication of the multidisciplinary consensus guideline for the management of SIH attempts to address this by proposing a working definition for OH in SIH that considers the various orthostatic characteristics outlined in our study. However, the described criteria were based on consensus amongst a group of experts in absence of any prospective data, which we now have available to help refine this further (11). We propose the first data-driven definition of the typical OH characteristics observed in SIH, which we hope will facilitate earlier recognition of this often-misdiagnosed disorder, while also potentially minimising unwarranted invasive investigations.
In our study, headache was present in 97.8% of patients; orthostatic at index clinic and initial onset in 75.9 and 82.5%, respectively. The systematic review by D’Antona et al. (4) reported that 96.3% of patients with SIH had an OH, a significantly higher proportion than that observed in the present study. The most probable explanation for this discrepancy is that the ICHD-2 criteria for SIH mandated the presence of an OH, thus excluding patients with non-orthostatic headache presentations, or those without headaches, potentially contributing to this difference. Other explanations include: inconsistencies in classification of OH between studies; recall bias regarding the initial headache type in our cohort; and a referral bias towards more atypical presentations to our tertiary headache clinic. Additionally, 38% of our cohort had undergone a prior EBP, which may have influenced the headache phenotype.
Hani and colleagues (14) noted a decline in incidence of OH with increasing disease chronicity. Since the authors (14) limited OH to only those that had an onset and offset “within minutes”, the aforementioned positive correlation between disease duration and time to onset, and offset, may explain the time-dependent decline in OH frequency in their study. The pathophysiological basis for the time-dependent changes in headache characteristics remains unknown but the findings emphasise the need for retrospective review of the headache phenotype at symptom-onset to help improve identification of the condition.
In our study, the time to onset/exacerbation and offset with postural changes were frequently rapid with the offset-time being more consistent, as indicated by a narrower IQR of 32.5 minutes compared to 120 minutes for the time to onset/exacerbation. Figure 1 graphically represents this data.

Violin plot highlighting the distribution of data for the three orthostatic headache characteristics: (1) time to onset/exacerbation of headache on becoming upright; (2) time to peak severity; and (3) offset-time to baseline headache severity on recumbency.
Traditionally, OH is typically recognised by the rapid development of headache upon assuming an upright posture rather than by the rapid resolution of the headache with recumbency. Our results challenge this notion, supporting our clinical observation, that headache-offset can occur as rapidly as, if not more rapidly than, its onset. Furthermore, in our clinical experience, the offset frequently remains the most consistent feature for any individual patient, despite changes in their other headache characteristics over time.
Vilming and Kloster (15) reviewed OH in post-lumbar puncture patients and found the median time of onset/exacerbation to be 20 seconds (range 0–265 minutes) and a median offset time to baseline of 20 seconds (range 0–11 minutes). This is significantly less than the values in our study, which may be indicative of possible phenotypic differences in the OH between spontaneous and iatrogenic CSF leaks. Another reason for the differences may be that the patients with post-dural puncture headache tend to present earlier than SIH, as a result of greater recognition of the condition and its temporal association with a medical procedure, which is known to affect the headache phenotype as also seen in our study (14). Similar to our study, the offset-time was rapid with lesser variability between patients in comparison to the onset-time.
The centile values indicate that our time to onset/exacerbation of OH on assuming an upright position are comparable to the findings by Mea et al. (16), where 75% developed a headache within two hours, and is in contrast to the study done by Chung et al. (17), who noted all 39 patients had an onset within five minutes. However, accurate interpretation is difficult as different criteria for what constitutes an OH might have been applied, as well as differences in study design and population.
Figure 1, alongside Table 6, also highlight that a small, but significant, proportion of the OH cohort in SIH have an atypically lengthy onset and/or offset. We explored the possibility of whether a prior history of migraine may be implicated in the atypical presentations. However, there was no statistical difference in the OH characteristics between the two groups.
In an attempt to address the question regarding whether SHOD headache represents a separate entity to OH, we compared the offset-time, which tends to be more consistent, between those with a “delayed onset/exacerbation of headache” (>85th centile value) and those without. There was no statistically significant difference (p = 0.241) between the two groups. Although it is not possible to make a definitive statement at this juncture, due to the small numbers (n = 15) in the delayed-onset cohort, it is suggestive of SHOD being part of the OH continuum.
The outlined working definition for the typical OH characteristics in SIH, as per consensus of the SIG, was set at the 85th centile with the aim of delicately balancing the need for adequately capturing presentation of the vast majority of OH in SIH, without being overly inclusive in order to avoid outliers clouding the typical orthostatic phenotype. It is our view that the proposed working definition should be seen as a supportive aid, rather than as a diagnostic tool, since atypical onset and offset do occur in SIH, and comparative data from other causes of OH are lacking, which are necessary to ascertain presence of clinically distinct phenotypes. Nonetheless, this represents a critical initial step towards the objective characterisation of OH typically seen in SIH, serving the vital clinical and academic interests already outlined above.
Associated non-headache symptoms are also common in SIH and can sometimes dominate the clinical picture instead of headache as the main source of disability (4,8). This is reflected by the missing data on time to maximum headache severity when upright as patients are frequently more disabled by the non-headache symptoms, which can force them to lie down instead of the headache.
Audiovestibular features were highly prevalent in our SIH cohort regardless of the headache phenotype. It was also interesting to note the high prevalence of migrainous features in SIH patients; in the appropriate clinical context where OH is typical for SIH, presence of migrainous features should therefore not dissuade a clinician from considering CSF leak as the diagnosis.
Presence of rhinorrhoea in a patient with other clinical and radiological findings suggestive of SIH can lead to undue concern of a cranial CSF leak. In our study, almost 14% of patients with a spinal CSF escape had rhinorrhoea, which we propose is part of the autonomic symptomology patients experience with both primary and secondary headache syndromes. Consequently, pursuing additional diagnostic procedures to identify a cranial leak is expected to be of limited benefit in this context.
Limitations
Our study has notable limitations. First, participants were drawn from a specialised tertiary clinic, which often experiences delayed presentations, potentially skewing the characteristics of reported headaches, including the orthostatic phenotype. Additionally, 38% of patients also had a previous non-targeted EBP. Despite observation of statistically significant difference being limited to time to peak severity, our study was not adequately powered to identify subtle differences in the other OH characteristics.
Lastly, the study includes three patients with history of complicating CVST, and 45.3% of patients had history of SDC; it is conceivable that they can affect the headache phenotype, including the orthostatic characteristics. Given the small number of patients with CVST, the overall impact on the results is likely to be negligible, particularly since two of the three patients had already been treated with anticoagulation for over six months. Regarding SDC, they are understood to represent a sequelae of brain sagging and thus, the clinical syndrome is invariably consistent with CSF hypovolaemia rather than intracranial hypertension. In our study, there was no difference in frequency of OH in relation to presence of SDC (p = 0.979), nor were there any statistically significant differences in the OH characteristics. Moreover, our study represents real-world data reflective of what is frequently encountered by a clinician, and SDC are a common feature of SIH.
Conclusions and future work
This is the first detailed clinical phenotyping study for OH that has outlined an objective definition for what constitutes a typical OH in SIH.
By defining the typical OH characteristics, in the right clinical context, this study will provide clinicians with an evidence-base for appropriate and timely identification and therein work-up of SIH, which has the potential of improving outcome and reducing disability associated with the disorder (18). In particular, we anticipate its utility when faced with a patient who has clear postural headaches but where MRI is negative for CSF leak, and other differential diagnoses have been excluded. This is a commonly encountered situation where there is limited evidence-base to guide further management, including searching for, or treatment of, an occult spinal CSF leak, since a normal MRI does not exclude the diagnosis in up to 20%. In such a scenario, knowledge of the typical OH characteristics in SIH will help support the clinician with this difficult decision-making process. Given SIH patients can be headache-free, experience non-orthostatic headaches, and have OH with atypically long onset and offset times, this definition is not intended to be used in isolation as a diagnostic tool.
This research also challenges the conventional approach to assessing OH with the time for headache-offset on recumbency being shown to be the most important and consistent factor.
On the academic front, standardised use of the term OH will allow for comparable data between studies, and thus improving our overall understanding of this highly disabling condition. This study represents an important initial step in this regard.
Future work include OH phenotyping studies for the other differential diagnoses, particularly PoTS, cervicogenic headache and migraine, to investigate for phenotypic differences between these disorders; if unique phenotypic signatures are identified, it will greatly aid the diagnostic process and ensure early optimal management. Within the SIH cohort, a sufficiently powered phenotyping study exploring potential differences in OH characteristics between patients presenting at different stages of the disease is also required.
Time to baseline headache severity on lying down is the most important factor when assessing for an orthostatic headache. In patients with chronic headaches, retrospective history of orthostatic headache at onset should be sought as this quality can be lost with time. Rhinorrhoea can be present in almost 14% of patients with spontaneous intracranial hypotension.
Footnotes
Acknowledgements
We thank our cohort of patients for participating in this study, as well as the Lysholm Department of Neurology at the National Hospital for Neurology and Neurosurgery. We also extend our thanks to the specialist interest group for their invaluable input.
Author contributions
MM was involved in the design and inception of the study. Clinical interviews were conducted by MM, SK, SC and DM. SC, SG and DM performed data collection. AQ and ID were involved in the review of neuroimaging. DM, with help from SC, was involved in analysis and write-up of the study. JA, CD, AT, PS, SL, CJ, PD, BD, HAL and JW were part of the specialist interest group. JR played a key role in the review and phenotyping of patients with cognitive and behavioral disturbances. All authors contributed to the editing and production of the final version of manuscript submitted for publication.
Data availability
Data can be made available upon reasonable request to the corresponding author.
Declaration of conflicting interests
DM, SC, SG, SK, PS, AT, CD, AQ, ID and JW have no competing interests.
MSM is chair of the medical advisory board of the CSF Leak Association; has served on advisory boards for Allergan, Autonomic Technologies Inc, Eli Lilly, Novartis, Pfizer, Salvia and TEVA; has received payment for educational presentations from Allergan, electroCore, Eli Lilly, Novartis and TEVA; has received grants from Abbott, Medtronic and electroCore; and has a patent on system and method for diagnosing and treating headaches (WO2018051103A1, issued). JA has received remuneration for consultancy advice and education provision from Allergan/AbbVie and TEVA. HA-L has lectures and education paid by International Medical Press, Sanofi and Eisai. BD has received remuneration for consultancy advice and education provision from TEVA, Allergan and Lilly. PJD has received fees or educational support from Abbvie, Lilly, Novartis, Pfizer and TEVA, and has shareholdings in Novo Nordisk, Lilly, Regeneron, Alnylam and Ionis Pharma. SL has received fees for attending advisory meetings, presentations and preparing presentation materials from Abbvie, TEVA, Eli Lilly, Tillots Pharma, Salvia and Novartis. CJ is a member of CSF Leak Association. JDR has received funding from a Miriam Marks Brain Research UK Senior Fellowship, an MRC Clinician Scientist Fellowship (MR/M008525/1) and the NIHR Rare Disease Translational Research Collaboration (BRC149/NS/MH), as well as the MRC UK GENFI grant (MR/M023664/1), the Bluefield Project and the JPND GENFI-PROX grant (2019-02248).
Ethical statement
Research ethics committee approval has been obtained from the London – Chelsea Research Ethics Committee (REC number: 21/PR/0827). All patients gave informed consent for their anonymised clinical data to be included in the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.