
Abstract
Abstract
Background
Spontaneous intracranial hypotension is diagnosed with an increasing frequency, but epidemiologic data are scarce. The aim of this study was to determine the incidence rate of spontaneous intracranial hypotension in a defined population.
Methods
Using a prospectively maintained registry, all patients with spontaneous intracranial hypotension residing in Beverly Hills, California, evaluated at our Medical Center between 2006 and 2020 were identified in this population-based incidence study. Our Medical Center is a quaternary referral center for spontaneous intracranial hypotension and is located within 1.5 miles from downtown Beverly Hills.
Results
A total of 19 patients with spontaneous intracranial hypotension were identified. There were 12 women and seven men with a mean age of 54.5 years (range, 28 to 88 years). The average annual incidence rate for all ages was 3.7 per 100,000 population (95% confidence interval [CI]: 2.0 to 5.3), 4.3 per 100,000 for women (95% CI, 1.9 to 6.7) and 2.9 per 100,000 population for men (95% CI, 0.8 to 5.1).
Conclusion
This study, for the first time, provides incidence rates for spontaneous intracranial hypotension in a defined population.
Introduction
It is now well-recognized that spontaneous intracranial hypotension (SIH) is an important cause of new-onset daily headaches, particularly in young and middle-aged individuals (1–6). An orthostatic headache, i.e., a headache that is exacerbated by the upright position, is the prototypical manifestation of SIH, but the positional component often becomes less recognizable with the passage of time (1–6). Spontaneous intracranial hypotension may also cause various other more or less serious neurologic manifestations such as hearing loss, dizziness, diplopia, nuchal rigidity, coma, and bibrachial amyotrophy (1–6). Most, but not all, patients with SIH have an abnormal brain MRI showing one or more of the following features: subdural fluid collections, pachymeningeal gadolinium enhancement, engorgement of venous structures, pituitary enlargement, and brain sagging (2). A spontaneous spinal cerebrospinal fluid (CSF) leak is the underlying cause in the great majority of, if not all, cases of SIH (1–7). Much has been learned about this disorder especially over the last few decades, but epidemiologic data are scarce. The great majority of reported series have been from major referral medical centers. The present study was undertaken to examine the occurrence of SIH in a defined population.
Methods
This population-based incidence study was approved by our Medical Center’s Institutional Review Board. Requirement for written informed consent was waived by the Institutional Review Board.
Since 1 January 2001, all patients with SIH evaluated by us in person at Cedars-Sinai Medical Center in Los Angeles, California, have been enrolled prospectively in a registry by the patients’ treating physicians. Patients evaluated remotely with the use of telehealth were not included. In this registry, United States patient residency is captured by zip code and using zip codes 90210, 90211, and 90212, we identified all residents of Beverly Hills, California who received a diagnosis of SIH between 1 January 2001 and 31 December 2020. The diagnosis of SIH was based on the criteria of the International Classification of Headache Disorders, third edition (ICHD-III), with minor modifications (8). These criteria require objective evidence of SIH, consisting of brain MRI showing stigmata of SIH (i.e., pachymeningeal enhancement, brain sagging, or subdural fluid collections), spinal imaging showing a CSF leak (i.e., the presence of extradural CSF or a CSF-venous fistula), or low CSF opening pressure (i.e., <6.0 cm H2O). The modification consists of also including patients who do not have headaches but whose symptoms are best explained by SIH. The type of underlying spinal CSF leak was classified according to a previously published classification system (9). Briefly, type 1 CSF leaks are caused by a dural tear located ventral to the spinal cord (type 1a) or (postero-)lateral to the spinal cord (type 1b). Type 2 CSF leaks are associated with simple (type 2a) or complex (type 2b [dural ectasia]) meningeal diverticula. Type 3 CSF leaks are CSF-venous fistulas. Type 4 CSF leaks are of indeterminate origin.
Beverly Hills is a small city (5.71 square miles) within Los Angeles County in Southern California. The medical services for residents of Beverly Hills are provided by an unknown number of medical facilities. Our Medical Center is a quaternary referral center for SIH and is located within 1.5 miles from downtown Beverly Hills.
Patients with a history of trauma were not included. Patients who had been a resident of Beverly Hills less than six months before the onset of symptoms were also excluded, ensuring that individuals who may have moved to Beverly Hills because of their illness would not be counted.
Statistical analysis
Estimates for the average annual incidence of SIH and 95% confidence intervals were calculated based on the 2016 population census estimates for the city of Beverly Hills (n = 34,627) (10). The average annual incidence between 2006 and 2020 was calculated by taking the ratio of the total number of SIH cases and the 2016 census population, and averaging over 15, the numbers of years corresponding to the cases being reported. The average annual incidence is reported in terms of new cases reported per 100,000 population. Estimates by sex (male: 15,959; female: 18,668), and age in years (18–64: 21,003; ≥18: 27,740; ≥65: 6737) were similarly calculated considering census population estimates for the specific demographics (10). For calculating incidence rates, the entire population of Beverly Hills was considered to be at risk. The population of Beverly Hills at census has been steady and increased from 33,784 in 2000 to 34,109 in 2010 (2019 estimate: 33,921) (10). Statistical analyses were conducted using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
There were no missing data.
Results
Before 2006 no cases of SIH were diagnosed among residents of Beverly Hills. Nineteen residents of Beverly Hills who suffered SIH were identified from 2006 through 2020. These patients were diagnosed during this 15-year period at a stable rate of zero to four per year. Average annual incidence rates were calculated from 2006 through 2020 and were age- and sex adjusted to the estimated 2019 population.
The average annual incidence of SIH for all age groups was 3.7 per 100,000 population (95% confidence interval [CI], 2.0 to 5.3). The average annual incidence of SIH for those aged 18 years and older was 4.6 per 100,000 population (95% CI, 2.5 to 6.6). The average annual incidence of SIH for women was 4.3 per 100,000 population (95% CI, 1.9 to 6.7) and for men was 2.9 per 100,000 population (95% CI, 0.8 to 5.1).
Clinical and imaging characteristics of the 19 patients are presented in Table 1. The mean age at the time of onset of SIH of the 12 women and seven men was 54.5 years (range, 28 to 88 years). Among the 19 Beverly Hills residents, three patients were transferred from other hospital systems in Los Angeles County, six patients were first evaluated in our emergency department (two after being sent there following imaging at an outpatient facility showing subdural hematomas), and ten patients were evaluated in an outpatient setting. The duration of symptoms prior to the diagnosis of SIH ranged from five days to eleven years (median, ten days; mean, six months). Headache was the most common symptom and was noted by 17 patients (89.5%). The onset of headache was acute (thunderclap headache) in two patients. The headache was orthostatic in 12 patients (63.2%). Among these 12 patients, the headache occurred within ten minutes of assuming the upright position in seven patients, between 11 and 30 minutes in three patients, and between 31 and 60 minutes in two patients. Four of the five patients with non-orthostatic headaches had subdural hematomas. Associated symptoms such as aural fullness, neck pain, nausea, and dizziness were common. Uncommon manifestations included coma (Glasgow Coma Scale score: 8), bibrachial amyotrophy, and syringomyelia in one patient each. Three patients had a history of migraine. Two patients had a body mass index greater than 30 (obese). The diagnosis of SIH was established by the typical changes on brain MRI in 17 patients, the presence of an extradural CSF collection associated with a normal brain MRI in the patient with bibrachial amyotrophy, and a low opening pressure (2 cm H2O) associated with normal brain and spine imaging in one patient with orthostatic headaches. Initial symptoms of SIH developed during the study period in all 19 patients.
Clinical and radiographic characteristics of 19 patients with spontaneous intracranial hypotension.
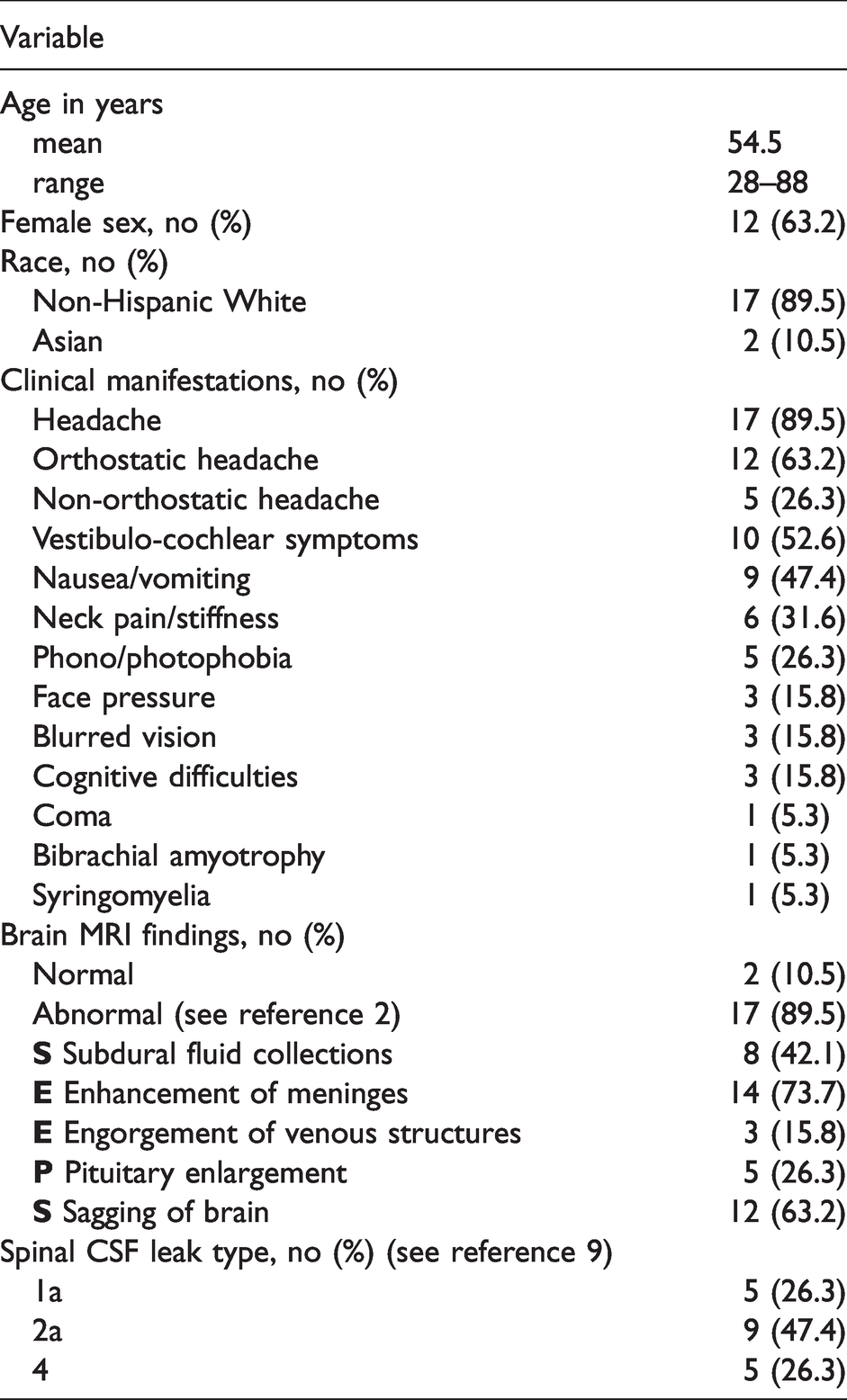
Brain MRI showed the typical findings of SIH in 17 patients and was normal in two patients. MR-myelography (heavily T2-weighted MRI) was performed in 14 patients, routine CT-myelography in three patients, and prone digital subtraction myelography in three patients. Extradural CSF was detected in five patients. Five patients had a type 1a leak, nine patients were classified with type 2a leak, and five patients had a leak of undeterminate cause (type 4). Opening pressure was obtained in seven patients and was low in three patients (2–5 cm H2O) and it was normal in four patients (7–13 cm H2O).
Treatment consisted of conservative measures (bed rest, oral hydration, abdominal binder) only in two patients. Improvement of symptoms was noted within one week by both patients. Sixteen patients underwent epidural blood patching. Improvement of symptoms was noted within three days by all patients. Ten patients underwent epidural blood patching once (mean volume of blood: 36 mL; range, 10–61 mL) and six patients underwent repeat epidural blood patching (mean total volume of blood: 88 mL; range, 80–95 mL). Percutaneous fibrin glue injections were used in two patients who failed repeat epidural blood patching. Surgery was performed in one patient who failed percutaneous procedures and in the patient with bibrachial amyotrophy.
Follow-up of at least one year was complete for all patients and the mean duration of follow up was 5.7 years (range, six months to 13 years). Complete symptom resolution was reported by 17 of the 19 patients. One patient with a ventral CSF leak has persistent symptoms following percutaneous procedures and is considering surgery and the patient with bibrachial amyotrophy did not improve following surgical closure of the ventral CSF leak although symptom progression was halted. Brain MRI normalized in 16 of the 17 patients, while persistent brain sagging was seen in one patient with symptom resolution.
Discussion
Spontaneous intracranial hypotension is not common. This was reflected in the relatively small number of cases that were diagnosed in the Beverly Hills community during the study period. These patients constitute less than 2% of the total number of patients with SIH evaluated at our Medical Center as a quaternary referral center for SIH.
We found the average annual incidence of SIH for all age groups to be 4 per 100,000 population. This is similar to an estimated annual incidence of 5 per 100,000 for SIH in the only previously published study on the epidemiology of SIH. In that study, we tracked all cases of SIH and aneurysmal subarachnoid hemorrhage (SAH) seen in the Emergency Department of our Medical Center (11). During the four-year study period, we identified 11 patients with SIH and 23 with SAH and we used the incidence rate for SAH of 10 per 100,000 per year to estimate the incidence for SIH (11). There was no overlap between cases reported in the Emergency Department study and the current community-based study.
Although not common, this study shows that SIH is not rare. The presently reported incidence figures for SIH in our community-based study are likely to be an underestimation because it is unlikely that all patients with SIH from Beverly Hills have been evaluated at our Medical Center. The annual incidence of 4 per 100,000 for SIH compares with 2–8 per 100,000 for idiopathic intracranial hypertension (12), 2–10 per 100,000 for cluster headache (13), and 4 per 100,000 for trigeminal neuralgia (14).
The community of Beverly Hills is not representative of Los Angeles County or of the Unites States in general and our results cannot be easily extrapolated to other communities. For example, the race/ethnicity of distribution of the population of Beverly Hills is 79% Non-Hispanic white, 9% Asian, 6% Hispanic, and 2% Black compared to 28% Non-Hispanic white, 14% Asian, 48% Hispanic, and 9% Black in Los Angeles County (10). Although the percentage of foreign-born residents is identical (35%), this population mainly consists of European and Middle-Eastern immigrants in Beverly Hills and Latin American immigrants in Los Angeles County.
This community-based study provides some contrasts to findings reported for our entire cohort of patients, most of whom have been referred to us from outside of California. In our entire cohort of patients, about 50% required surgery (9) compared to only about 10% of residents of Beverly Hills. Conservative measures and epidural blood patching provided excellent symptom relief in about 80% of patients and the remaining 10% of patients required percutaneous fibrin glue injections. The reason for this discrepancy probably is due to referral bias where patients with recalcitrant symptoms in spite of more widely available treatments such as epidural blood patching are most likely to be referred. In our entire cohort of patients, spine imaging showed extradural CSF collections in about 50% of patients (9) compared to only about 20% of residents of Beverly Hills. The reason for this discrepancy is unknown, but may be due to physicians rejecting the diagnosis of SIH if no clear evidence of a CSF leak is found on routine spine imaging.
Limitations
The main limitation of this study is that it is unlikely that all patients from Beverly Hills with SIH have been evaluated at our medical center. Although our medical center is a quaternary referral center for SIH and is situated adjacent to Beverly Hills, Beverly Hills is a small city surrounded by numerous medical centers, and medical services for residents of Beverly Hills are provided by an unknown number of medical facilities. In addition, Veteran Affairs patients are not routinely evaluated at our medical center. The potential ascertainment bias would have resulted in an underestimation of the true incidence of SIH. This study also was limited by the relatively small size of the study population. No data were available on in-and-out migration to estimate person-time for the denominator necessitating the use of census-based population numbers for denominators. Finally, Beverly Hills is not representative of Los Angeles County with regard to, for example, racial distribution, nation of origin, income, and access to medical care. Thus, our results cannot be easily extrapolated to other communities.
Conclusions
We found an annual incidence rate for SIH of 4 per 100,000 in the community of Beverly Hills, California, demonstrating that SIH is not a rare disorder.
Article highlights
The incidence of spontaneous intracranial hypotension is 4 per 100,000 per year Spontaneous intracranial hypotension is not rare. It is as common as trigeminal neuralgia and about half as common as aneurysmal subarachnoid hemorrhage Surgical repair of the underlying spinal CSF leak is infrequently necessary
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.