
Abstract
Abstract
Introduction
Spontaneous intracranial hypotension due to a spinal cerebrospinal fluid leak causes orthostatic headaches and impacts quality of life. Successful closure rates are often reported, whereas data on long-term outcome are still scarce.
Methods
Between April 2020 and December 2022 surgically treated patients completed the Headache Impact Test-6 prior to surgery and at 14 days, three months, six months, and 12 months postoperatively. In addition to the Headache Impact Test-6 score, we extracted data related to orthostatic symptoms.
Results
Eighty patients were included. Median Headache Impact Test-6 score preoperatively was 65 (IQR 61–69), indicating severe and disabling impact of headaches. At three months headache impact significantly improved to 49 (IQR 44–58) (p < 0.001) and remained stable up to 12 months (48, IQR 40–56), indicating little to no impact of headaches on quality of life. The need to lie down “always” or “very often” was reduced from 79% to 23% three months postoperatively (p < 0.001).
Conclusions
Surgical closure of spinal CSF leaks significantly improves the impact of headaches in the long term. At least three months should be expected for recovery. Despite permanent closure of the CSF-leak, a quarter of patients still have relevant long-term impairment, indicating the need for further research on its cause and possible treatment.
Introduction
Spontaneous intracranial hypotension (SIH) caused by a spinal cerebrospinal fluid (CSF) leak has an estimated incidence of 5 in 100,000. While a broad range of manifestations like visual symptoms, nausea, vestibulocochlear symptoms, “brain fog”, fatigue and chronic subdural hematomas can occur, the most common and suggestive clinical feature is orthostatic headache (1–3). Diagnosis of SIH is made based on clinical features and confirmed with imaging, such as magnetic resonance imaging (MRI), dynamic myelography and computed tomography (CT) myelography (4,5). The management of SIH is multifaceted and interdisciplinary. Treatment options include conservative measures, epidural blood patching, transvenous embolization, CT-guided fibrin glue occlusion and microsurgical sealing of the leak.
Patients report a high impact on their quality of life because of their symptoms (6,7). Assessing the outcome of SIH treatment can be challenging, as it is a complex and heterogeneous condition with a wide range of symptoms and presentations. Although many different headache scores are established, a specific score for the assessment of the predominantly orthostatic headaches in SIH patients does not currently exist. Reports on outcomes after SIH treatment are usually limited to a relatively short follow-up of several weeks (8–10). There is no data about the long-term results of more extensive surgical series. However, reliably assessing outcomes is crucial to effectively monitor the treatment success and for improving the counseling and treatment of future patients.
The self-administered 6-item Headache Impact Test (HIT-6) questionnaire was introduced and validated in 2003, with translations from English into German and French (11,12). The score consists of six questions assessing the impact of headaches on different aspects of life, including work, school, social life, and psychological functioning. No distinction is made between different types of headaches (tension-type headaches, migraines, etc.). Each question has a five-point ordinal scale with “never”, - “rarely”, - “sometimes”, - “very often”, - “always”. Higher scores indicate a more significant impact of headaches on the patient’s quality of life. The lowest possible score of 36 represents no impact, and the highest score of 78 the most severe impact of headaches. Changes considered clinically relevant are 2.5 in patients with migraine, 2.3 in patients with chronic daily headache and 8 in patients with tension-type headache (13–15). One question in the score (“When you have a headache, how often do you want to lie down?”) addresses the avoidance of movement during headache episodes, a common feature in different types of headache. The question, however, also seems very suitable to evaluate the impact of orthostatic headaches among SIH patients. A special regard to this “orthostatic item” may be useful in assessing and quantifying the burden of the orthostatic headache component in the SIH population.
Patient-reported outcome measures (PROMs) represent an innovative approach to evaluate the effect of an intervention. Electronic devices such as tablets or smartphones for collecting PROMs have been shown to be feasible and reliable in different patient populations, including those with chronic pain or chronic diseases and traumatic brain injury (16,17).
Our study aimed to analyze the long-term outcome of surgically treated SIH patients via a digital PROM system, explicitly focusing on the HIT-6 score with special emphasis on orthostatic headaches.
Methods
Study design
This single-center study was conducted using data from a prospectively maintained database of patients who met the ICHD-3 criteria for SIH (18) and underwent surgical treatment for a spinal CSF leak between April 2020 and December 2022. Spinal CSF leaks were confirmed based on a previously described diagnostic protocol (4). The study followed the STROBE statement and guidelines (19). The local Ethics Committee approved the study (22-1512-S1-retro), and all subjects provided informed consent for using the collected PROM data.
Patients eligible for inclusion had:
Microsurgical sealing of the ventral or lateral CSF leak or the CSF venous fistula Completed HIT-6 score preoperatively and available follow-up of at least 14 days. Consent for evaluation of the data
Exclusion criteria:
Linguistic or intellectual problems with the completion of the questionnaires. No reliable contact possibility for electronic follow-up No consent
HIT-6 scores were clustered in the categories “no or only little impact” (score ≤49), “some impact” (score 50–55) and “substantial or severe impact” (score ≥56) as applied in previous studies (8,10). The question “When you have a headache, how often do you want to lie down?” was singled out as being explicitly important in SIH-patients and rated separately as “orthostatic item”. The answers “always” and “very often” were considered as relevant and limiting daily life and therefore pooled together and compared to the pooled answers “sometimes”, “rarely”, and “never”.
Patients were asked to complete the HIT-6 score preoperatively on a tablet and postoperative at 14 days, three, six and 12 months, respectively, via an automated follow-up system. All questionnaires were filled out using a digital automated PROM software (Heartbeat Medical, Berlin, Germany). Patients were contacted directly once in case of an incomplete follow-up after three months or more. If the patients were still lost to follow-up, their data were censored at the date of the last completed questionnaire.
Patient-specific data and data regarding imaging findings, surgery and the perioperative course were prospectively collected and analyzed retrospectively.
Statistical analysis
Analyses were performed using SPSS Statistics (IBM, Version 29) and the R software (version R 4.0.4) through the studio interface Version 1.4.1106. As Shapiro-Wilk-testing ruled out normal distribution in almost all follow-up dates, the median with interquartile range (IQR) was reported. Changes in HIT-6 scores, the HIT-6 score clusters and the “orthostatic item” were compared using nonparametric tests as appropriate (Friedman’s test or Wilcoxon signed-rank test). All time points were separately compared to each other with pairwise Conover post-hoc test comparisons. P-values <0.05 were considered statistically significant.
Results
Patient selection and demographics
Between April 2020 and December 2022, 110 patients underwent surgery for spinal CSF loss. Of these, 30 were excluded from the analysis, nine because of linguistic difficulties in completing the questionnaires, seven because of lack of electronic contact via email, and 14 because of lack of consent to participate in the study. Therefore, 80 patients (49 female, 31 male) were included in the final analysis (Figure 1).
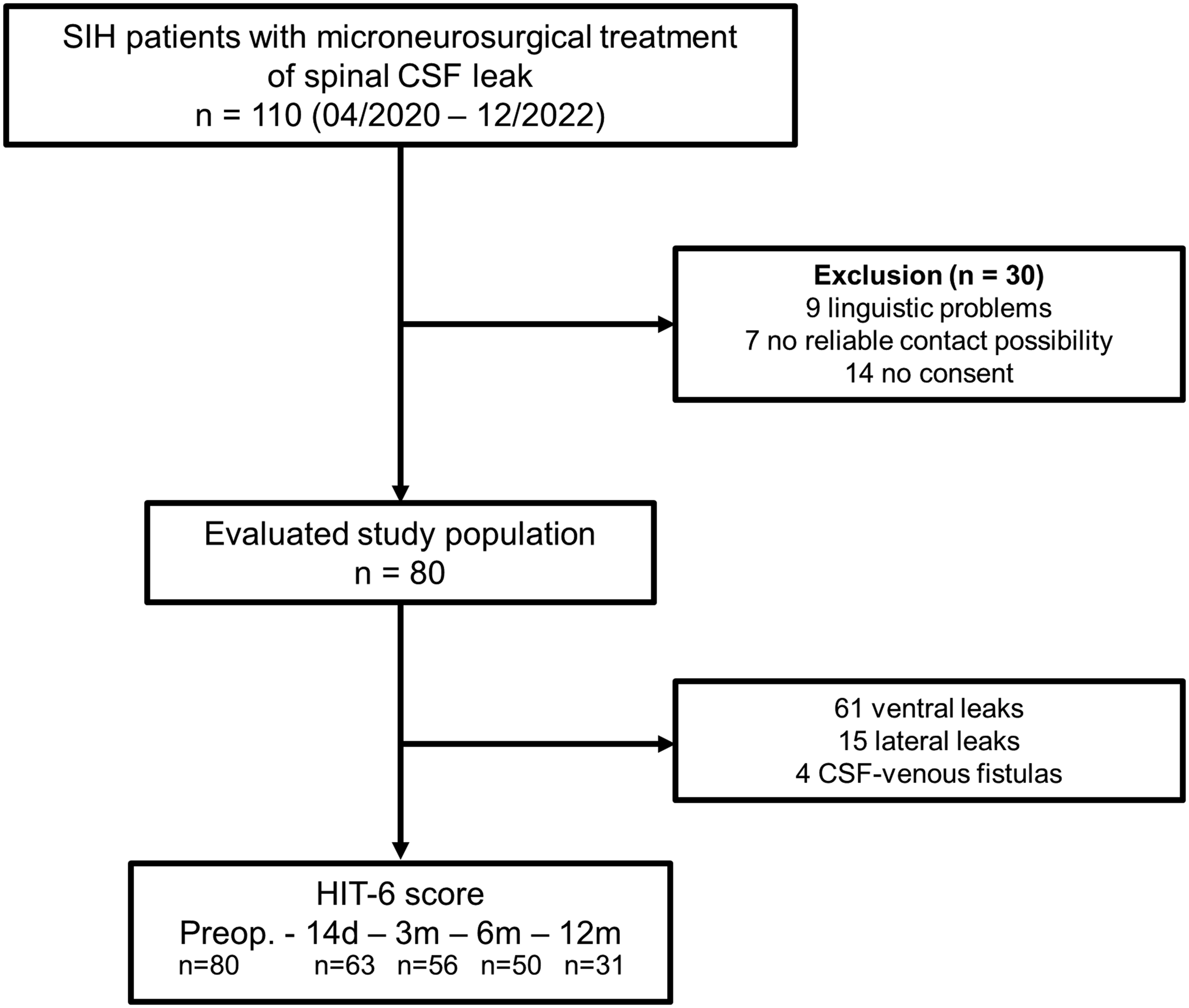
Flowchart displaying patients’ selection.
The mean age was 44.1 ± 11.1 years (range 24–77 years). Sixty-one (76%) had a ventral leak, 15 (19%) had a lateral leak, and four (5%) had a CSF-venous fistula, all at the thoracic spine, respectively (20). Median Bern SIH-score (21) before the surgery was 5 (IQR 2–8) (Table 1).
Cohort demographics.

In 78/80 patients, typical predominant symptoms, such as orthostatic headaches, mostly accompanied by posture-related change in hearing, dizziness, led to the diagnosis of SIH. Two patients (1%) had no predominant but still subtle orthostatic headache: one presented with a multifactorial gait disorder, and the second with cerebellar superficial siderosis. The median symptom duration before surgical treatment was four months (IQR 2.0–13.5 months). The most prolonged period of symptoms before surgery was 13 years.
Treatments
Initially and before admission to our center all patients reported prior treatments with either bed rest, fluid substitution, and/or caffeine intake for at least two weeks or a combination of the mentioned options, either as outpatients or in another institution. Before surgery, 43 patients underwent epidural blood patching, three had an unsuccessful surgery for a suspected spinal CSF leak at other institutions, and one had an unsuccessful embolization of the CSF-venous fistula. Finally, 34 patients (43%) had no specific treatment before the surgery.
Regarding surgical management, all surgeries were performed in prone position using a minimally invasive approach with a non-expandable tubular device. Treatment for all ventral leaks (n = 61) was via a transdural approach and intra-/extradural sandwich-patching previously described in detail by Beck et al. 2022 (22). For the lateral leaks, treatment was extradural dura-augmentation and fibrin-patching with additional clipping of the nerve root (n = 10) or without clipping (n = 4). In one case, a transdural sandwich-patching technique with dura-augmentation was performed. Surgery for CSF-venous fistulas consisted of transdural disconnection of the fistula, dura-augmentation, and fibrin-patching (n = 2) or extradural disconnection of the fistula dura-augmentation and fibrin-patching and additionally clipping of the affected nerve root (n = 2).
Eight patients (five ventral leaks, three lateral leaks) needed revision surgery. Two patients (one ventral leak, one lateral leak) had an epidural hematoma, without a permanent neurological deficit after evacuation. A persisting or recurrent leak was suspected in six patients (three ventral leaks, three lateral leaks); thus, revision surgery was performed after repeated imaging. A persisting leak at the original location was found in three patients (two lateral and one ventral leak), which could successfully be closed. In one revision surgery (initially classified as a lateral leak), a ventral leak was identified one level below the initial surgical site and was successfully sealed using the transdural sandwich patching technique. In two cases, the revision surgery revealed an unremarkable situs without any indication of a persisting CSF loss and was compatible with a seroma. All these patients did well after the second intervention, and there was no case of a third surgical intervention.
Postoperatively, no permanent neurologic deficit was found in any of the cases. In the patients where a nerve root had been clipped an expectable unilateral localized hypesthesia in the corresponding thoracic dermatome was observed.
HIT-6 score
Follow-up rates were 79% (63/80) at day 14, 70% (56/80) at three months 63% (50/80) at six months and 39% (31/80) at 12 months, respectively.
The median preoperative HIT-6 score was 65 (IQR 61–69), indicating severe impact of headache. Postoperatively there was a significant decrease to a median of 56 (IQR 51–64) at day 14 (p < 0.001), and a further significant decrease to 49 (IQR 44–58) at three months (p < 0.001). This effect remained stable up to 12 months: HIT-6 score 52 (IQR 40–61) at six months, and 48 (IQR 40–56) at 12 months, without significant changes after three months (p > 0.05, respectively). (Figure 2). Clustering the HIT-6 score in the three categories “no or only little impact” (score ≤49), “some impact” (score 50–55) and “substantial or severe impact” (score ≥56) showed a significant shift towards the little or not at all affected subgroups (p < 0.001) (Figure 3). Subanalysis of cohorts stratified by the leak type showed no differences in severity of the headache impact, nor in the postoperative course.
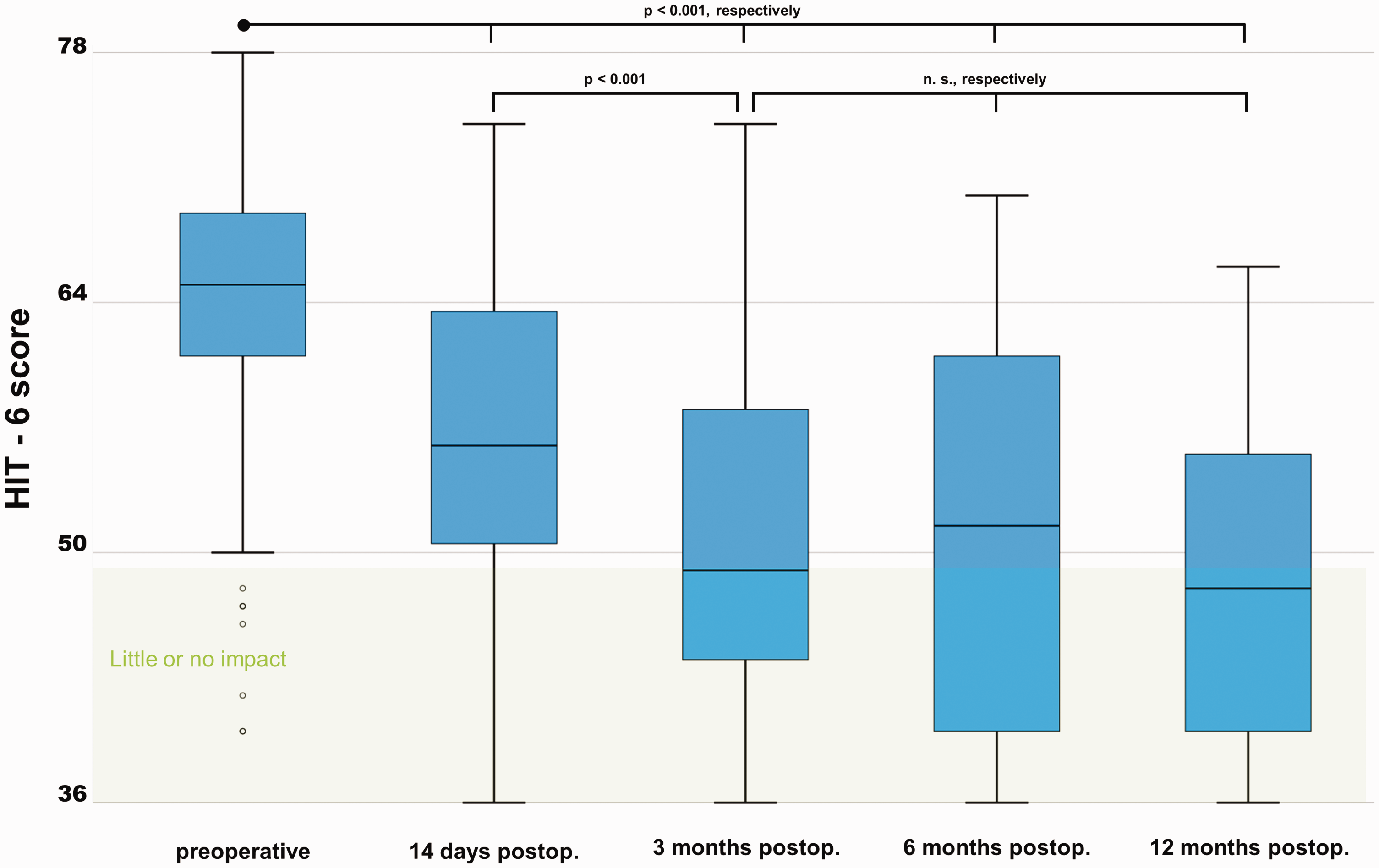
Boxplot representing the HIT-6 scores at different time points. A HIT-6 score ≤49 indicates no or only little impact of headaches in daily life. The preoperative HIT-6 score indicated severe impact of headache. Postoperatively there was a significant improvement already at day 14 (p < 0.001), and a further improvement at three months (p < 0.001). This effect remained stable up to 12 months, without significant changes after three months (p > 0.05, respectively).

Pie chart representing HIT-6 score. The areas of the circles represent the size of the follow-up collective. The rate of patients with substantial or severe impact of headaches (HIT-6 score ≥56, red color) drops after surgery. There is a relevant decrease of severely affected patients observed at all follow-up time points (85% preoperatively to 51% on day 14, 30% at three months, 38% at six months and 26% at 12 months, p < 0.001, respectively). Despite this clear improvement, approximately 25% of patients continue to have substantial or severe impact of headaches after three months and at the one-year follow-up.
The “orthostatic item” applied to SIH
The “need to lie down” as a subitem of the HIT-6, hence labelled as the “orthostatic item”, significantly improved after surgery (Figure 4). Preoperatively, a total of 78% (62/80) of patients reported severely disabling position-dependent headaches (need to lie down “very often” in 37/80 and “always” in 25/80 patients, respectively). Fourteen days postoperatively, the “orthostatic item” was significantly improved to 37% (23/63); three months postoperatively, there was a further improvement to only 23% (13/56) (p < 0.001, respectively) of severely disabling position-dependent symptoms. At 12 months, improvements remained stable at 23% (7/30).
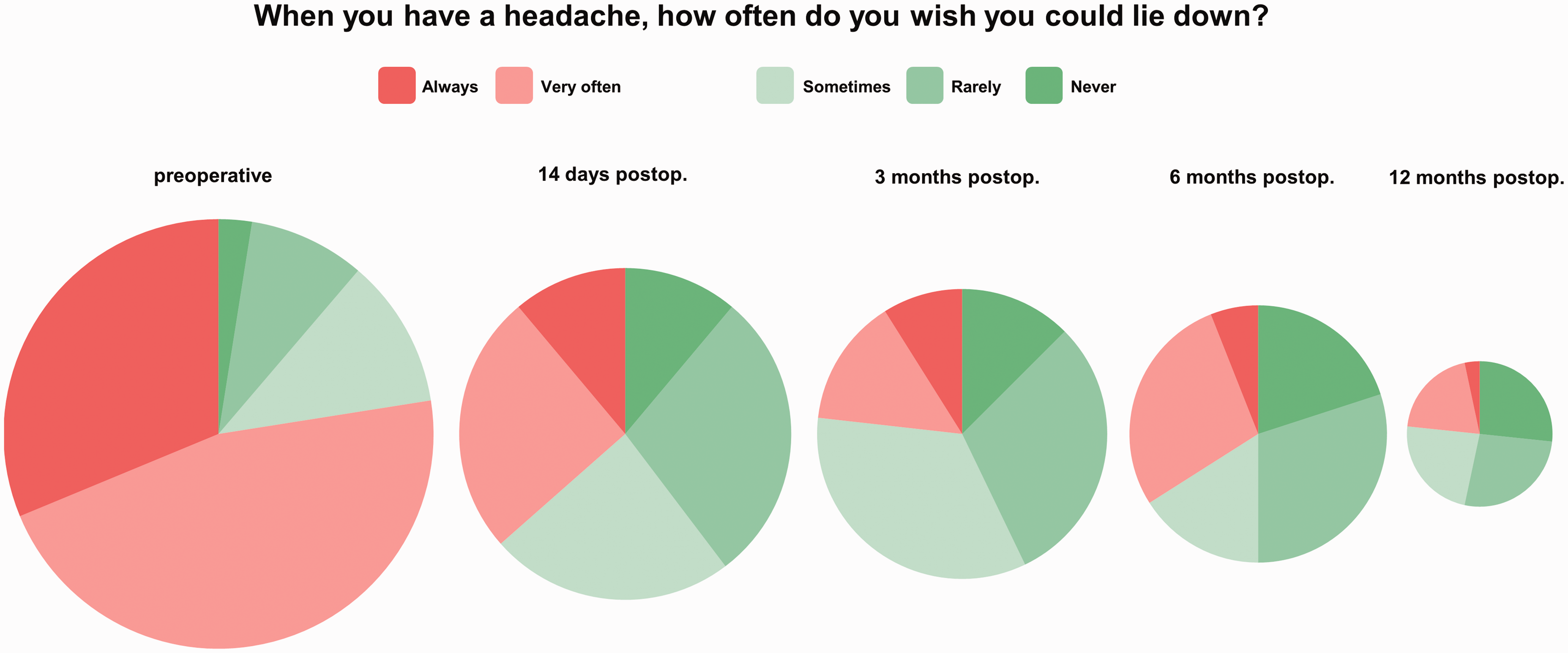
Pie chart representing the “orthostatic item” within the HIT-6 score: The areas of the circles represent the size of the follow-up collective. Red color indicates relevant impairment (stated as “always” and “very often” by the patient). The relevant orthostatic headache component is significantly reduced after sealing of the leak (79% preoperatively to 37% on day 14, 23% at three months, 34% at six months and 23% 12 months, p < 0.001, respectively).
Discussion
Our study showed a significant improvement in the HIT-6 scores from preoperatively 65 (representing a severely disabling impact of headaches) to 49 at three months and 48 at 12 months postoperatively (representing little to no impact of headaches, respectively) with an average improvement of 16 points (Figure 2). This improvement can be considered definitely relevant as it clearly exceeds the generally accepted values for clinically relevant HIT-6 changes (2.3 for chronic daily headache, 2.5 for migraine and 8 for tension-type headache [13–15]). Improvement occurred as early as 14 days after surgery, continued to improve up to three months and remained stable during subsequent follow-up periods. However, despite this unequivocal improvement in the overall patient cohort, one quarter of patients continued to experience headaches with substantial or severe impact (HIT-6 score ≥56) on daily life after one year (Figure 3).
In the literature, the HIT-6 was used to evaluate the treatment success of CSF-venous fistula either by embolization in 40 patients (8), by CT-guided fibrin glue occlusion in 35 patients (9) or by surgical ligation in 20 patients (10). These studies showed a significant improvement in the HIT-6 score after the respective treatment, without paying special attention to the orthostatic headache component. After surgical treatment of SIH patients with mixed pathologies, Häni et al. reported a significant improvement in headaches measured by the Numerical Rating Scale (NRS) in a series of 69 patients at three months of follow-up (7).
There is no consensus yet on the exact time point at which the success of treatment can be assessed. Mamlouk et al. (9) report a mean follow-up of 10.3 months (0.5 – 20 months) after fibrin glue sealant occlusion, Brinjiki et al. (8) of two to four months after transvenous embolization, Wang et al. (10) do not mention the exact time of postoperative evaluation and follow-up. Considering the possible rebound hypertension effect after CSF spinal leak sealing and a usual postoperative recovery period, a follow-up time of at least three months seems reasonable. This is in line with our findings, pinpointing the significant improvement of the median HIT-6 score up to three months.
In the studies mentioned above, the HIT-6 after the respective treatment modality was assessed at one follow-up date. Our study is the first one with a systematic follow-up including multiple follow-up sessions up to one year. As a result, our study offers a more comprehensive evaluation of the timeline of change after surgery, as well as the long-term outcomes. However, due to the limited number of patients even in a dedicated reference center, our results emphasize the need of more prospectively and systematically collected outcome data in surgically treated SIH patients.
It is not uncommon to encounter residual headaches even after successful CSF-leak closure. This does not seem to restrain the quality of life of patients and certain patients may have a good quality of life despite these residual headaches. One might suppose that other types of headaches (migraine, tension-type headaches) and post-therapeutic rebound hypertension may be the cause. A commonly used definition of rebound hypertension is headaches that worsen while lying down and improve while standing (“reverse orthostatic headache”) and respond to acetazolamide. The rebound hypertension rate is described to be around 27% (23), however, the exact pathogenesis is not yet completely understood (24,25). This rebound hypertension, which is indeed the very evidence of successful leak closure, may nevertheless result in an elevated or not completely normalized HIT-6 score.
As mentioned, the HIT-6 questionnaire does not distinguish between different types of headache. There is no specific score to assess the classic orthostatic headache in SIH. Although the question “When you have a headache, how often do you want to lie down?” was originally intended to capture the general avoidance of movement rather than an orthostatic component of headaches, a separate and special consideration of this “orthostatic item” could help to better discriminate between persistent low-pressure headache and new rebound-hypertension headache after surgery. As a result, the “orthostatic item” could easily guide subsequent steps, such as ensuring successful sealing of the leak or initiation of pressure-lowering drugs. The time-consuming de-novo establishment and validation of a new score for this rare clinical picture seems hardly justified. A separate assessment of the “orthostatic item” within the HIT-6 seems more reasonable and is instantly applicable in clinical practice. For patients, there is the benefit of sparing an additional questionnaire.
Limitations
All the constraints of a single center, retrospective study apply. The cohorts of patients with SIH are usually from referral centers and, therefore, highly selected. Although outcome data were collected prospectively and systematically, loss of follow-up is present, partly due to the fact, that up to this point not all patients have reached the appropriate follow-up time. Therefore the results from six to 12 months follow-up need to be regarded preliminary. However, these follow-up rates permit a first insight of possible outcome in long-time follow-up. Still, the present study to our knowledge is the largest prospectively recorded series in SIH patients treated with surgery. However, the number of patients with this rare disease is still limited, so follow-up studies, ideally as prospective multicenter trials, are needed to confirm our findings.
Conclusion
Surgery permanently closes the CSF spinal leaks in SIH patients and significantly improves the impact of headaches in the long-term. An automated digital PROM platform using the HIT-6 is an easy and feasible way for long-term follow-up. A recovery period of at least three months should be expected and discussed with the patient preoperatively. Special consideration of the “orthostatic item” within the HIT-6 score is a simple and useful addition in the follow-up of SIH patients. Despite the encouraging results, one quarter of patients still have relevant impairment one year after surgery, indicating the need for further research to improve outcomes.
Article highlights
Surgery permanently closes spinal CSF-leaks in SIH patients and significantly improves long-term impact of headaches measured with the HIT-6 score. A recovery period of three months should be expected before an assessment of treatment success. The HIT-6 score with special regard of the “orthostatic item” is a simple and efficient way for follow-up of SIH-patients.
Footnotes
Author’s Contributions
FV, AER, CF, JB: Design of the study. FV, AER KW, MO: Data acquisition and analysis. JB, FV, CF, NL, HU: Providing of infrastructure. Manuscript writing and corrections with contributions of all authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Ministry of Research, Science and Arts Baden-Württemberg. AER received a scholarship grant from the Nuovo-Soldati oncology research foundation. No author received financial support for the research, authorship, or publication of this article.