
Abstract
Objectives
To determine the proportion of patients with spontaneous intracranial hypotension (SIH) who had a cerebrospinal fluid (CSF) pressure >6 cm H2O and to investigate the clinical and imaging variables associated with CSF pressure (PCSF) in this condition.
Methods
We retrospectively reviewed 106 patients with SIH. PCSF was measured by lumbar puncture prior to treatment. Clinical and imaging variables – including demographic data, brain imaging results, symptom duration, and abdominal circumference – were collected. Univariate and multivariate analyses were performed to determine the correlation of these variables with PCSF.
Results
Sixty-one percent of patients had a PCSF between 6 and 20 cm H2O; only 34% had a PCSF ≤6 cm H2O. The factors associated with increased PCSF included abdominal circumference (p < 0.001), symptom duration (p = 0.015), and the absence of brain magnetic resonance imaging findings of SIH (p = 0.003). A wide variability in PCSF was observed among all patients, which was not completely accounted for by the variables included in the model.
Conclusions
Normal CSF pressure is common in patients with SIH; the absence of a low opening pressure should not exclude this condition. Body habitus, symptom duration, and brain imaging are correlated with PCSF measurements, but these factors alone do not entirely explain the wide variability in observed pressures in this condition and this suggests the influence of other factors.
Keywords
Introduction
Spontaneous intracranial hypotension (SIH) is an increasingly recognized disorder characterized by a loss of cerebrospinal fluid (CSF) through defects in the spinal thecal sac (1). Classically, patients with SIH exhibit low CSF pressure (PCSF), defined as an opening pressure measured by lumbar puncture of ≤6 cm H2O; this association with low PCSF is often considered to be fundamental to the pathogenesis of the disease. For example, the International Classification of Headache Disorders, third edition (ICHD-3) defines SIH as “caused by low cerebrospinal fluid pressure of spontaneous origin,” noting that “It remits after normalization of CSF pressure” (2).
Despite the frequent observation of low PCSF in many patients with SIH, some investigators have observed, seemingly paradoxically, that some patients with SIH have pressures in the normal range (3). This observation challenges the concept that low PCSF is the primary etiology of the disorder, although previous reports have suggested that this phenomenon occurs in only a minority of patients with SIH, with estimates of the prevalence of a normal PCSF in patients with SIH of approximately 25% (3–6). Most of these estimates, however, have been based on case series with a limited size.
The purpose of this investigation was to evaluate the range of PCSF in patients with SIH using a large case series and to determine the proportion of patients with CSF opening pressures in the normal range. In addition, we sought to examine the demographic, clinical, and imaging factors that influence PCSF in this cohort of patients.
Methods
Patients
Diagnostic criteria for spontaneous intracranial hypotension, modified from Schievink et al. (7).

Demographic information and clinical history, including age, sex, duration of symptoms, and history of previous EBP, were recorded from the medical records of the patients. The investigation was approved by the authors’ local institutional review board and was compliant with HIPAA regulations.
CSF pressure measurements
CSF opening pressures were obtained from procedure reports from the initial computed tomography (CT) myelogram, which is obtained as part of the standard workup in all cases of suspected SIH at our institution. Pressure was measured by lumbar puncture performed at the L3–4 or L4–5 level using fluoroscopic or CT-fluoroscopic (CTF) guidance and either a 22- or 24-gage needle with the patient in the lateral decubitus position. Pressures were measured with the patient’s legs extended, after instructions not to talk or the Valsalva maneuver. The procedures were performed by one of two board-certified radiologists with 32 and 12 years of experience in performing image-guided lumbar punctures and who held a certificate of added qualification in neuroradiology.
Image analysis
Available pre-procedural brain imaging studies were reviewed to determine whether imaging signs of SIH were present. The review was carried out in the picture archiving and communication system by a board-certified radiologist who was a second-year fellow in neuroradiology. Brain MRI was considered to be positive for SIH if pachymeningeal enhancement or brain sagging was present according to the previously reported criteria (7). Brain sagging was judged on sagittal T1- or T2-weighted images and pachymeningeal enhancement was judged on axial or coronal post-contrast T1-weighted images. Borderline cases were adjudicated by a board-certified radiologist who held a certificate of added qualification in neuroradiology and had 12 years of experience interpreting brain MRI scans and extensive experience of treating patients with SIH. If the patient had only a non-contrast brain MRI scan, then the imaging was only considered positive if brain sagging was present.
Abdominal circumference was determined from imaging obtained as part of the CTF-guided lumbar puncture using the technique reported previously by Ciudin et al. (9) This technique uses bi-dimensional diameters from CT imaging to estimate the perimeter of an ellipse and has been shown to accurately predict standing waist circumference (9). Body mass index (BMI) was not used as these data were incomplete for a large number of patients. However, it has previously been shown that abdominal circumference and BMI are very highly correlated, with one analysis of four multicenter trials showing correlation coefficients between these two measures of 0.84–0.89 (10).
Statistical analysis
Univariate analysis
The dependence of PCSF on categorical variables (brain MRI findings, sex, and prior EBP) was assessed using a two-sample t-test. The dependence of PCSF on continuous variables (duration of symptoms, abdominal circumference, and age) was modeled using simple linear regression. For the duration of symptoms, a log transformation was used for the predictor due to its skewed distribution. The null hypothesis test of no effect of the predictor on the average PCSF levels was tested using a one-sample Wald test of the estimated slope.
Multivariate analysis
The joint effect of the six univariate predictors on PCSF was assessed using a multivariate linear regression model of the form:

The modeled outcome was the observed CSF pressure for patient i = 1, … , 106. The model explains this in terms of the baseline average µ, which represents a 47.6-year-old male patient with an abdominal circumference of 897.9 mm who had experienced symptoms for six months, did not display any brain imaging signs, and had no history of an EBP. In addition, we had effects for sex (α F ), imaging signs (α Pos.MRI ), history of EBP (α EBP ), and a linear effect of age, duration, and abdominal circumference. Finally, ɛ i was a measurement error and was assumed to have a zero mean Gaussian distribution. Model 1.1 was fitted to the data using multivariate linear regression. The significance of predictors was assessed using Wald tests. Values with p < 0.05 were considered statistically significant.
Results
Patient demographics
We identified 106 patients (69 women and 37 men) ranging in age from 18 to 83 years (mean ± SD 47.6 ± 13.2 years) who met the inclusion criteria for SIH. The mean ± SD abdominal circumference was 89.9 ± 13.8 cm (range 60.6–127.8 cm). The abdominal circumference could not be calculated in one patient because the images were technically inadequate.
A total of 44 (42%) patients had undergone EBP prior to opening pressure measurement at our institution; in all instances these patients either had no benefit from the prior EBP or had a relapse of their symptoms. Data about symptom duration were available in 95 (90%) patients. The mean ± SD symptom duration was 20.2 ± 38.5 months (range 0.3–240 months); however, the distribution was heavily skewed toward a symptom duration of <1 year, with 46% of the patients reporting symptoms of <6 months duration and 69% reporting symptoms of <12 months duration.
Brain imaging findings
Pre-treatment brain MRI data were available in 99 (93%) patients. Of those patients with available brain MRI data, 93 included both pre- and post-contrast images (94%), whereas six (6%) patients had only non-contrast images. Of the patients with available post-contrast brain images, 77 (82%) showed evidence of smooth, diffuse dural enhancement. Of all the patients with brain images, 60 (60%) showed evidence of brain sagging. A total of nine (9%) patients showed neither dural enhancement nor brain sagging on MRI and thus were considered to show no evidence of SIH on brain imaging.
Distribution of CSF pressure
Figure 1 shows histograms of the PCSF for all patients. The mean ± SD PCSF was 8.5 ± 6.0 cm H2O (range 0–31 cm H2O). A total of 34% of patients had a PCSF ≤ 6 cm H2O, the range considered to be diagnostic of low CSF pressure and typically associated with SIH. Sixty-one percent of patients had a PCSF between 6 and 20 cm H2O and 5% of patients had a PCSF > 20 cm H2O.
Histograms of PCSF in patients with spontaneous intracranial hypotension. (a) Distribution of PCSF based on a bin size of 2 cm H2O. (b) Distribution of PCSF based on common categorizations of CSF pressure (0–6, 6–12, 12–20, >20 cm H2O). Listed percentages within each bar indicate the percentage of the total number of patients falling into that bin.
CSF pressure correlations
Figure 2 shows the univariate analyses of categorical variables (i.e. positive brain MRI, prior EBP, and sex) and Figure 3 shows the continuous variables (i.e. duration of symptoms, abdominal circumference, and age). Table 2 gives the estimated effects from the multivariate model of PCSF.
Univariate analysis of categorical variables. Box-and-whisker plots comparing dependence of PCSF on brain (a) magnetic resonance imaging findings of spontaneous intracranial hypotension (SIH), (b) history of prior epidural blood patching (EBP), and (c) sex. Univariate analysis of continuous variables. Scatterplots of dependence of PCSF on (a) abdominal circumference, (b) duration of symptoms, and (c) age. Estimated effects from multivariate modeling of PCSF.

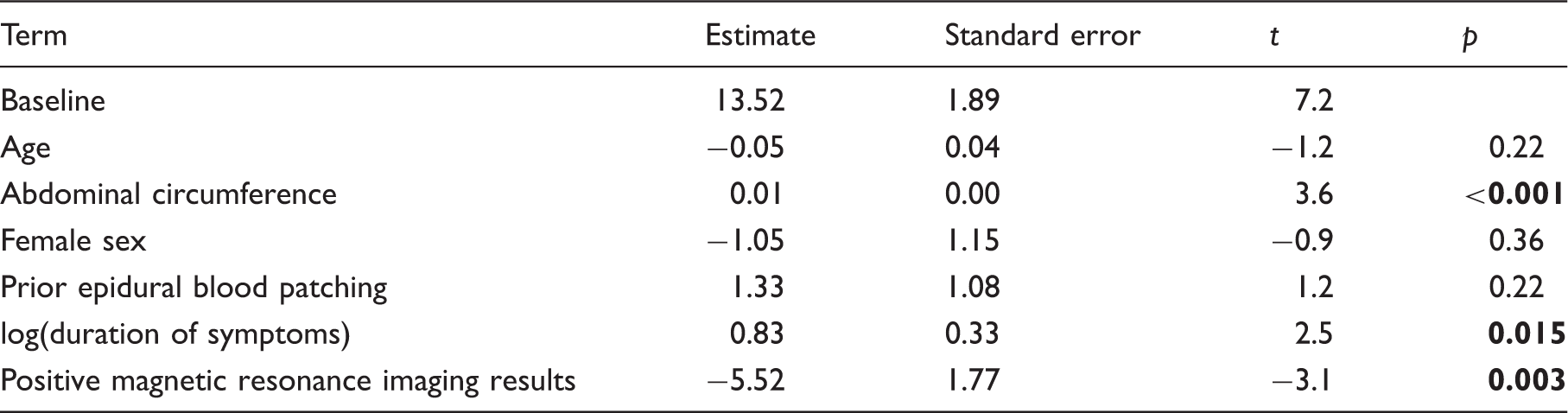
Abdominal circumference was positively correlated with PCSF in both the univariate (p = 0.001) and multivariate analysis (p < 0.001), increasing at a rate of 0.01 cm H2O/mm abdominal circumference.
The correlation between PCSF and brain MRI changes in SIH was not statistically significant on univariate analysis (p = 0.23), but was found to be highly significant on multivariate analysis (p = 0.003), where patients without brain MRI changes had an average increase in PCSF of 5.2 cm H2O compared with those with MRI changes.
PCSF increased slowly (i.e. on a log scale) with increasing duration of symptoms on both univariate (p = 0.002) and multivariate analysis (p = 0.015).
Female sex was marginally correlated with lower opening pressure on univariate analysis (p = 0.035), but was not significant in the multivariate model (p = 0.41). Age was not associated with PCSF on either univariate (p = 0.44) or multivariate (p = 0.26) analysis. A history of prior EBP was not significantly associated with PCSF on either univariate (p = 0.10) or multivariate analysis (p = 0.32).
Even for those terms that were found to be strongly correlated with PCSF (abdominal circumference, positive brain MRI, and duration of symptoms), there was a wide variability in PCSF reflected by a relatively low R2 of 0.31 for the multivariate model. For example, PCSF < 6 cm H2O was seen in patients both with and without changes of SIH on brain imaging and in patients along the entire spectrum of abdominal circumference and symptom duration.
Discussion
SIH has historically been understood to be a direct manifestation of low CSF pressure caused by leaks of spinal CSF. Despite this understanding, previous investigators have reported that, in some patients, the CSF pressure may be normal rather than low, observations that led Mokri (11) to propose the alternative terminology of CSF hypovolemia rather than intracranial hypotension for the syndrome. Still, the finding of PCSF of >6 cm H2O has been widely believed to occur only in a minority (perhaps up to one in four) of patients with SIH (4). Our investigation of a large series of patients with SIH indicates that CSF pressures in the normal range occur much more frequently than commonly believed, with 61% of patients exhibiting a PCSF between 6 and 20 cm H2O.
In contrast with conventional assumptions about CSF pressure in patients with SIH, only 34% of patients with SIH in our series actually had a low CSF pressure (PCSF ≤ 6 cm H2O). Perhaps most notable, however, was the finding of patients with symptoms typical of SIH and surgically or myelographically documented CSF leaks who presented with PCSF > 20 cm H2O (Figure 4). Although these patients constituted the minority (5%) of our population, such findings are a departure from the conventional understanding of CSF physiology in SIH and indicate that a single CSF pressure value cannot be used to exclude the diagnosis of SIH. Further, they imply that PCSF in this condition is determined in a manner more complex than has been generally understood.
A 37-year-old woman presented with a positional headache and a cerebrospinal fluid (CSF) opening pressure of 20.4 cm H2O. (a) Axial image from computed tomography myelogram obtained immediately after opening pressure measurement showing active leakage of CSF into the epidural space (arrowheads). (b) Sagittal image from the same computed tomography myelogram showing a calcified disk protrusion in the upper thoracic spine (arrow). Subsequent digital subtraction myelogram (not shown) confirmed that the CSF leak originated at this level. (c) Intraoperative photograph showing the dural tear (arrow) caused by the disk (photo courtesy of Wouter Schievink).
Our results differed from those of several previous smaller series. In a series of 40 patients with SIH diagnosed on the basis of orthostatic headache and diffuse dural enhancement on MRI, Mokri et al. (3) reported that normal pressure was only seen in seven (18%) patients. In a series of 30 patients with SIH, Chung et al. (12) found only four patients with opening pressures of >6 cm H2O and, of these four, only one had a pressure >10 cm H2O. In that series, patients were considered to have SIH if they demonstrated at least two criteria including orthostatic headache, low CSF pressure, or diffuse dural enhancement on MRI.
In a more recent series in which the opening pressure was measured in 76 patients referred for clinically suspected SIH, Luetmer et al. (13) found that 43% of patients had a pressure between 10 and 18 cm H2O and 8% had a pressure >18 cm H2O, results similar to our findings. These varied observations regarding the frequency of normal PCSF in patients with SIH may be because the earlier experience of patients with SIH preferentially identified patients at the more extreme end of the clinical spectrum. It is likely that patients are now being identified who exhibit greater phenotypic variation as a result of increased clinical experience with this condition and the subsequent recognition that there is often variability in the presented images, CSF pressure, and clinical findings (14).
To help explain the spectrum of pressures observed in our patients, we examined several factors that could potentially influence PCSF, including clinical factors (duration of symptoms, prior EBP), demographic factors (age, sex, abdominal circumference), and the presence of brain imaging findings of intracranial hypotension. The strongest correlations were observed with abdominal circumference, brain imaging findings, and duration of symptoms.
The effect of obesity on CSF pressure in normal patients remains controversial, with some studies showing a positive correlation between increasing CSF pressure and BMI and others showing no association (15–18). Of the variables investigated in our model, however, abdominal circumference was most strongly correlated with PCSF, with a tendency for those patients with a larger abdominal circumference to have a higher PCSF.
It is possible that some patients with clinical symptoms of SIH, but normal PCSF, represent cases where the patient’s PCSF was high before developing a spinal leak (or at least relatively higher than after the onset of the leak) and that it is the relative decrease in pressure in these patients that is responsible for provoking symptoms, rather than the absolute PCSF value. One potential explanation for our observed association between abdominal circumference and PCSF is that patients with a larger body habitus had a higher baseline premorbid CSF pressure. Alternatively, it is possible that increased abdominal circumference interacts with the pathophysiology specific to SIH to influence the pressure through the regulation of compensatory mechanisms involved with CSF homeostasis. Such effects could be related to the effect of abdominal adiposity on venous flow dynamics or to hormonal effects, both of which have been postulated to increase CSF pressure (19,20). An underlying high CSF pressure at baseline in a subset of patients may increase the likelihood of developing a spontaneous leak through a vulnerable region of dura, a concept suggested previously by Mokri (4). Indeed, a parallel situation has been encountered with patients with spontaneous skull base CSF leaks, a condition that does not result in intracranial hypotension, but where increased PCSF is known to be a risk factor (21,22).
Duration of symptoms was also associated with PCSF in both the univariate and multivariate analysis. These results suggest the possibility that the PCSF pressure tends to rise with time after the onset of symptoms of SIH. This observation could be the result of physiological compensatory mechanisms. Equilibrium of the CSF space is known to depend on several factors, including the rate of CSF production, craniospinal compliance, CSF reabsorption, cerebral blood flow, and venous pressure (23), any of which could potentially be altered by a state of chronic CSF depletion. Clinically, the suggestion that PCSF may increase with time agrees with the authors’ observation that in many patients with SIH, the symptoms may be most severe initially, but may decrease in severity over time, even though an ongoing CSF leak is confirmed at myelography.
Our investigation found significant correlations between the absence of brain imaging findings (i.e. either dural enhancement or brain sagging) and PCSF on multivariate modeling. This is not surprising in the light of the interpretation of changes in the imaging appearance of the brain based on the physiological principles of the Monro-Kellie hypothesis (24). For example, dural thickening and enhancement is thought to reflect increased blood volume secondary to vascular engorgement of the pachymeninges incited by decreased CSF volume from within the craniospinal system, which is rigidly enclosed and therefore must maintain an overall constant volume. Similar changes to the intracranial blood volume are thought to account for other findings, such as the venous distention sign (25) and pituitary glandular enlargement (1). Brain sagging is hypothesized to be a manifestation of the loss of buoyancy in the intracranial compartment caused by leaking spinal CSF (26).
Despite these physiological relationships, it is well known that brain imaging changes are not present in all patients with SIH (27). This may be of clinical significance because some evidence suggests that patients with clinical symptoms of SIH who lack MRI changes may be more refractory to treatment (28). It is equally notable that PCSF alone did not predict the brain imaging findings for a substantial number of our patients. For example, an opening pressure of 0 cm H2O was found in some patients with brain MRI changes, but also in some patients without such changes. Again, this observation suggests a much more complex interaction of various determinants of PCSF and intracranial physiology in SIH than has previously been assumed.
Specifically, it is likely that brain imaging findings in SIH are reflection of decreased CSF volume rather than a direct manifestation of low CSF pressure (11). Although, under normal circumstances, CSF volume and pressure are related by a monoexponetial curve (29,30), this relationship seems to be altered some cases of CSF leak – for example, some patients with myelographic CSF leaks (and therefore decreased CSF volume) have a normal CSF pressure. Compensatory mechanisms such as dilation of the intraspinal and intracranial venous structures, a process known to occur in SIH (25,31), could alter the compliance of the craniospinal compartment, thus altering the relationship between CSF pressure and volume. Changes in the relative rates of CSF production and reabsorption could also potentially affect this relationship. Greater understanding of these effects could potentially help in the management of patients with SIH refractory to treatment, as well as with the development of novel alternatives to epidural patching or surgery for those with the disease. Although it is beyond the scope of this investigation, further exploration of the relationships between individual brain imaging signs, myelographic findings, CSF pressure, and symptom duration in patients with SIH is also warranted.
Several factors may influence the reliability of a single CSF pressure measurement, potentially adding to the variation we have observed in our study cohort. It has been hypothesized that some cases of SIH may be due to intermittent leaks (32), which could, in theory, result in variability in the measured CSF pressure depending on whether the leak was active. However, a previous study by Luetmer et al. (13) showed that active CSF leakage on myelography was not associated with a lower CSF pressure than in patients in whom no leak was seen. This suggests that whether a leak was continuous or intermittent did not have a large effect on the CSF pressure. Another potential confounder may be the variability in CSF pressure in an individual patient throughout the day, a phenomenon suggested previously (33).
We conclude that PCSF is only helpful as a diagnostic criterion for SIH if it is clearly low. Patients with pressures that are normal or even borderline elevated may still have SIH. Our results suggest that such patients should undergo further evaluation with brain and myelographic imaging if the clinical symptoms strongly suggest the condition.
It is important to note that our multivariate model fitted our data moderately poorly (R2 = 0.31), suggesting substantial inter-patient variability due to additional, as yet unexplained, variables that were not included in our model. Defining what these variables are and how they interact with CSF pressure, volume, and clinical symptoms is important in constructing a more comprehensive picture of the CSF dynamics in patients with SIH.
This investigation has several limitations. First, our practice at a tertiary care referral center introduces the potential for referral bias, possibly selecting for some atypical variations in PCSF in patients who had had unsuccessful initial treatment at other centers. However, the majority of patients in our series had not been treated for SIH previously and we found no difference in CSF pressures between those who had and had not been treated initially at other institutions. Furthermore, we used strict inclusion criteria to ensure a representative population of patients with SIH with a highly confident diagnosis. An additional limitation is that we used abdominal circumference, rather than the more typically used BMI, as a marker of body habitus, because these data were available. Although an investigation of the relationship between PCSF and waist circumference has not yet been established for a normal population, waist circumference has previously been shown to be very highly correlated with BMI (10,34) and therefore may be a reasonable surrogate for habitus. Nevertheless, these data should be interpreted with caution until the relationship between abdominal circumference and CSF pressure can be directly explored.
Conclusions
Normal CSF pressure is common in patients with SIH; the absence of a low opening pressure should not be used to exclude the condition. PCSF in patients with SIH is correlated with abdominal circumference, symptom duration, and brain imaging findings, but these factors alone are not sufficient to predict PCSF in many patients. Other unidentified factors are likely to contribute to the physiology, clinical symptoms, and imaging features of SIH.
Clinical implications
CSF pressure >6 cm H2O is common in patients with spontaneous intracranial hypotension. Absence of a low opening pressure should not be used to exclude the condition. CSF pressure should be interpreted in the context of brain imaging findings and myelographic evaluation for CSF leakage in patients with symptoms suggestive of spontaneous intracranial hypotension.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.